





Abstract
Tidal-breathing methacholine challenges are now recommended by guidelines, to avoid the bronchoprotective effects of deep inhalation. This study compared different tidal breathing methacholine challenge methods; assessed the agreement between tidal dosimetric and continuous output challenges; and assessed challenge repeatability with different methods.
15 asthma patients performed dosimetric challenges and a continuous-output breath-actuated challenge, all ≥3 days apart. All subjects had a pre-bronchodilator forced expiratory volume in 1 s (FEV1) ≥65% predicted, and a cumulative dose causing a 20% reduction in FEV1 (PD20) <1.2 mg.
Of the dosimetric challenges, one method increased methacholine concentration (standard dosimetric challenge), and one adjusted nebuliser output time to increase dose (adjusted dosimetric challenge). The adjusted dosimetric and continuous output challenges were performed twice on separate days to assess for repeatability. All challenges were matched for dose at each dose step. The mean PD20 ratio of the standard dosimetric challenge to the adjusted dosimetric challenge was 0.90 (95% CI 0.66–1.23, p=0.49) and intraclass correlation coefficient (ICC) was 0.82. Repeated adjusted dosimetric challenges had an ICC 0.62 for PD20. Repeated continuous output challenges had an ICC 0.74 for PD20. The adjusted dosimetric and continuous output challenges correlated (r=0.69, p=0.0043; ICC 0.65), but PD20 was higher for the adjusted dosimetric challenge (mean PD20 ratio 2.31, 95% CI 1.57–3.40; p=0.0004).
Tidal dosimetric methacholine challenge using adjustment of nebuliser output produces results with good repeatability. The results of this adjusted dosimetric method differed from the continuous output method, underscoring that the results of different methacholine challenge methodologies may not be directly comparable.
Abstract
Tidal breathing challenges are now the preferred method to administer a methacholine challenge. This study reports a tidal dosimetric methacholine challenge method that adjusts nebuliser output, which can be used to obtain results with good repeatability. https://bit.ly/3fX0F3f
Introduction
Asthma is characterised by variable airflow obstruction, airway inflammation and hyperresponsiveness [1]. Bronchial hyperresponsiveness (BHR) can be assessed with methacholine, a muscarinic receptor agonist that directly constricts airway smooth muscle [2]. Bronchoprovocation testing with methacholine is widely used in clinical trials to assess the effects of novel compounds on BHR in asthma patients [3–5]. In addition, methacholine challenge testing is used to help diagnose asthma [2, 6]. The concentration or cumulative dose causing a 20% reduction in forced expiratory volume in 1 s (FEV1) (PC20 or PD20, respectively) is the measured end-point for methacholine challenges [6].
Methacholine challenges have commonly been performed using dosimeter-controlled nebulisers involving five deep inhalations [7, 8], or continuous-output nebulisers with tidal breathing [8]. However, it is now accepted that deep inhalations can cause bronchoprotection against methacholine-induced airway narrowing [9], leading to the exclusion of the five-breath deep inhalation method in the European Respiratory Society (ERS) 2017 guidelines [2].
Continuous-output nebulisers using tidal breathing protocols may lead to considerable differences between individuals in the dose received due to variations in tidal volume and frequency. In order to address this issue, the ERS 2017 guidelines recommended that methacholine inhalation by tidal breathing should use a dosimeter-controlled or continuous-output breath-actuated nebuliser [2]. When calculating dose, the latter uses a pre-determined set tidal volume and frequency performed under simulation, rather than the patient's own, whereas the former allows for control of the actuation time per breath. The ERS 2017 guidance advocates that escalating dose should be achieved by changing the methacholine concentration, although there are alternatives such as changing the nebuliser output, or number of breaths taken. Alternative approaches may offer advantages in terms of practicality and cost-effectiveness, using fewer methacholine concentrations.
We have investigated methodological aspects of methacholine challenge testing relevant to the use of this technique in clinical practice and clinical trials. This study had three aims: to assess 1) the agreement between two tidal dosimetric challenge protocols (increasing concentration versus variation of both concentration and nebuliser output); 2) the agreement between tidal dosimetric challenges and continuous-output breath-actuated challenges; and 3) the repeatability of tidal dosimetric challenges and continuous-output breath-actuated challenges.
Materials and methods
Participants
This study recruited male and female asthma patients, with a pre-bronchodilator FEV1 ≥65% predicted, and a methacholine PD20 value of <1.2 mg. Eligible patients were nonsmokers or ex-smokers with a smoking history of <5 pack-years. All patients were prescribed either inhaled corticosteroid (ICS) and short-acting β2-agonist (SABA), or SABA only. Patients taking ICS were on a stable dose for ≥4 weeks prior to the study and for the study duration. Patients were excluded using the following criteria: known respiratory disorder other than asthma; current aortic aneurysm; recent myocardial infarction or stroke; hypertension; respiratory infection or use of antibiotics within 4 weeks; or presence of a contraindication to any the procedures, that in the investigator's opinion made it unsafe for the patient to participate. All patients provided written informed consent using a protocol approved by Greater Manchester East Research Ethics Committee (05/Q1402/41).
Study design
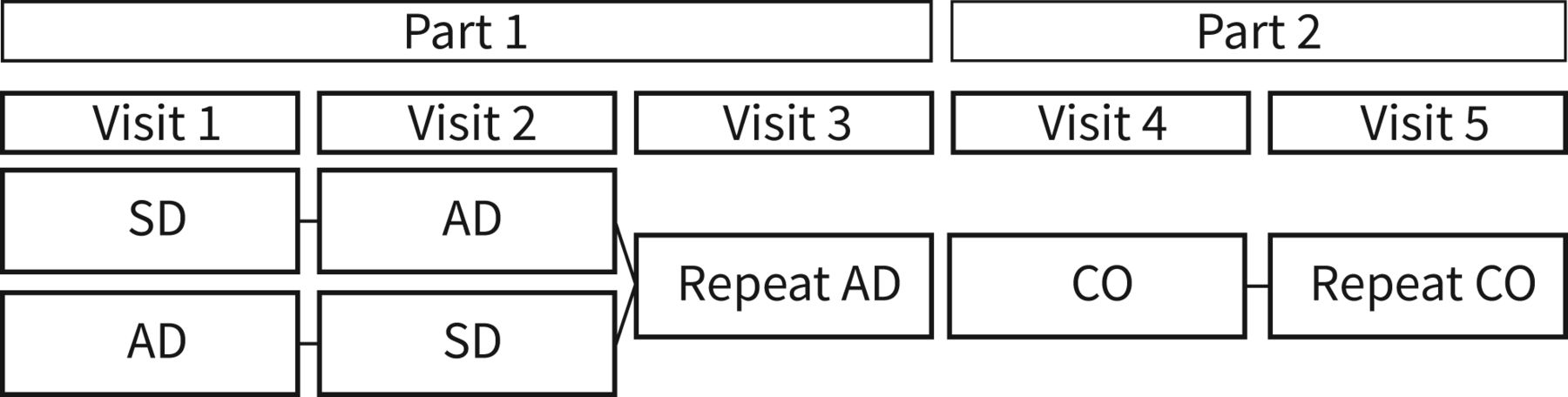
The study was conducted in two parts (figure 1). In part 1, participants attended for three visits, where tidal dosimetric challenges were performed. Each patient was randomised to perform a standard dosimetric (SD) challenge, using different methacholine concentrations at each step, at visit 1 followed by an adjusted dosimetric (AD) challenge at visit 2, or vice versa. The AD challenge used fewer methacholine concentrations, but adjusted the nebuliser output (table 1). At visit 3, a repeated AD challenge was performed. In part 2, patients returned to complete two more visits, where a continuous-output breath-actuated tidal breathing challenge was performed at each visit, here referred to as the continuous-output (CO) challenge. All visits were performed ≥3 days apart.

Study design. At visit 1, patients were randomised to perform one of the dosimetric challenges, followed by the alternative at visit 2. SD: standard dosimetric challenge; AD: adjusted dosimetric challenge; CO: continuous-output breath-actuated challenge.
Dose escalation in the standard dosimetric challenge (SD), the adjusted dosimetric challenge (AD) and the continuous-output challenge (CO)
Study procedures
Spirometry was performed on the NDD Easy On-PC system (NDD Medical Technologies, Zurich, Switzerland), according to American Thoracic Society (ATS)/(ERS) standards [10]. During post-challenge time points, FEV1 only was measured. Predicted values were calculated using the Global Lung Function Initiative 2012 equations [11].
Each patient complied with the ERS pre-test guidelines [2] prior to each challenge. The SD challenge was performed using ProvoX system (Ganshorn, Niederlauer, Germany) with an 8900 nebuliser (Salter Labs, Arvin, CA, USA). This setup provides nebulised methacholine for a defined time during the initial portion of each tidal inhalation. The nebuliser output time was set to 0.4 s per inhalation, with 15 inhalations per dose step, using doubling methacholine concentrations (0.03125–16 mg·mL−1). The AD challenge was performed using the same equipment, with 15 inhalations per dose step, and four dose steps per methacholine concentration (0.25 and 4 mg·mL−1), other than the final concentration (16 mg·mL−1), which was utilised for two dose steps. The nebuliser output time was doubled, as shown in table 1 for each concentration, to achieve a doubling dose challenge that matched that of the SD challenge. Methacholine was diluted to the required concentrations prior to each challenge, using Provocholine (Methapharm, Coral Springs, FL, USA).
In part 2, the CO challenge was performed using the AeroEclipse breath actuated nebuliser II (Trudell Medical International, Ontario, Canada), with a 20-s dose duration, and doubling methacholine concentrations (0.03125–16 mg·mL−1), matching the doses of the part 1 challenges (table 1). This breath-actuated device provides a continuous output of nebulised methacholine during the whole inhalation phase of each tidal breath. Subjects were instructed to perform spontaneous quiet tidal breathing while maintaining a seal on the nebuliser mouthpiece. For all challenges, FEV1 measurements were performed at 30 and 90 s post-end of administration, with the highest value used to calculate response. Incremental doses were administered at 4-min intervals (between start times of each administration) for all methods.
Statistical methods
The primary end-point was PD20, which was calculated for each challenge by linear interpolation, using cumulative dose, as per standard guidelines [6]. Dose was calculated using nebuliser output, as determined by the manufacturer (ProvoX system) or by testing using methacholine solution (AeroEclipse BAN II), as reported previously [12]. The natural log-transformed PD20 values were calculated and compared between challenge methods using paired t-tests. These values were back-transformed to report the ratio of one challenge method to another. Intraclass correlations (ICC) were performed; these are interpreted as excellent (>0.75), fair to good (0.40–0.75) or poor (<0.40) [13]. Bland–Altman plots were constructed as the difference between the natural log-transformed PD20 values (y-axis) versus the mean untransformed PD20 values (x-axis). Repeatability using doubling dose (DD) difference was calculated as reported previously; [14] briefly, within-subject standard deviation (WSTD) was calculated using the log-transformed mean difference and standard deviation of differences. DD was then calculated using the formula DD=(2(WSTD))/(log10(2)). t-tests were performed using Prism 5 (Graphpad, CA, USA), and ICC analysis was performed using SPSS 25.0 (IBM, Armonk, NY, USA). p<0.05 was considered statistically significant. No formal sample size calculation was performed; however, a sample of 15 was considered suitable given the study design.
Results
Participants
17 patients participated. Two patients were excluded with methacholine PD20 >1.2 mg at visit 1 (one who received SD challenge and one who received AD challenge), leaving 15 patients who continued to visit 2 (these 15 patients all completed the study). Patient characteristics are shown in table 2. The mean FEV1 was 92% pred, with approximately half of the patients using ICS. Baseline FEV1 at each visit was within 10% of the mean value for each patient (data not shown).
Patient characteristics
Comparison of tidal dosimetric protocols
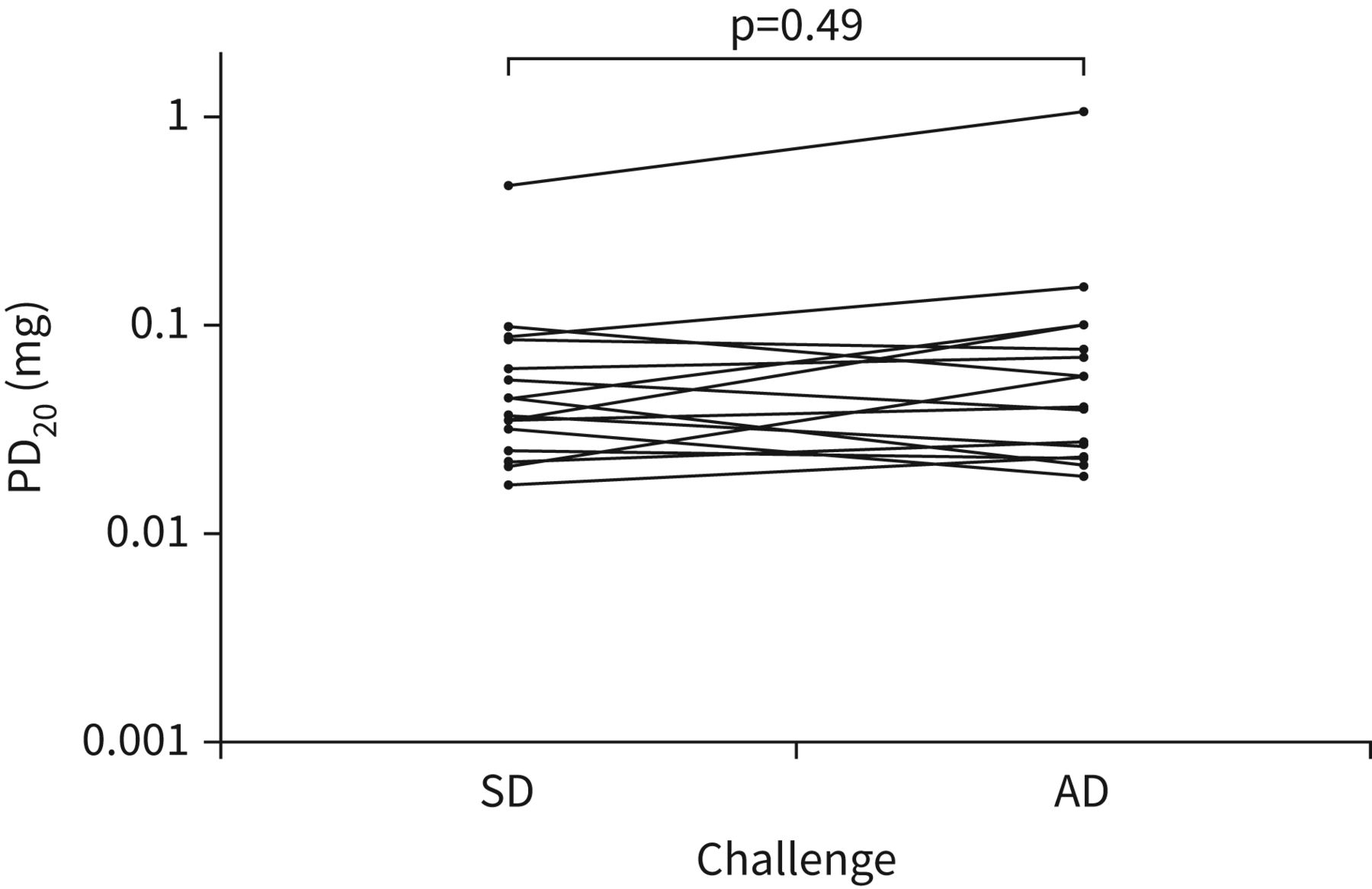
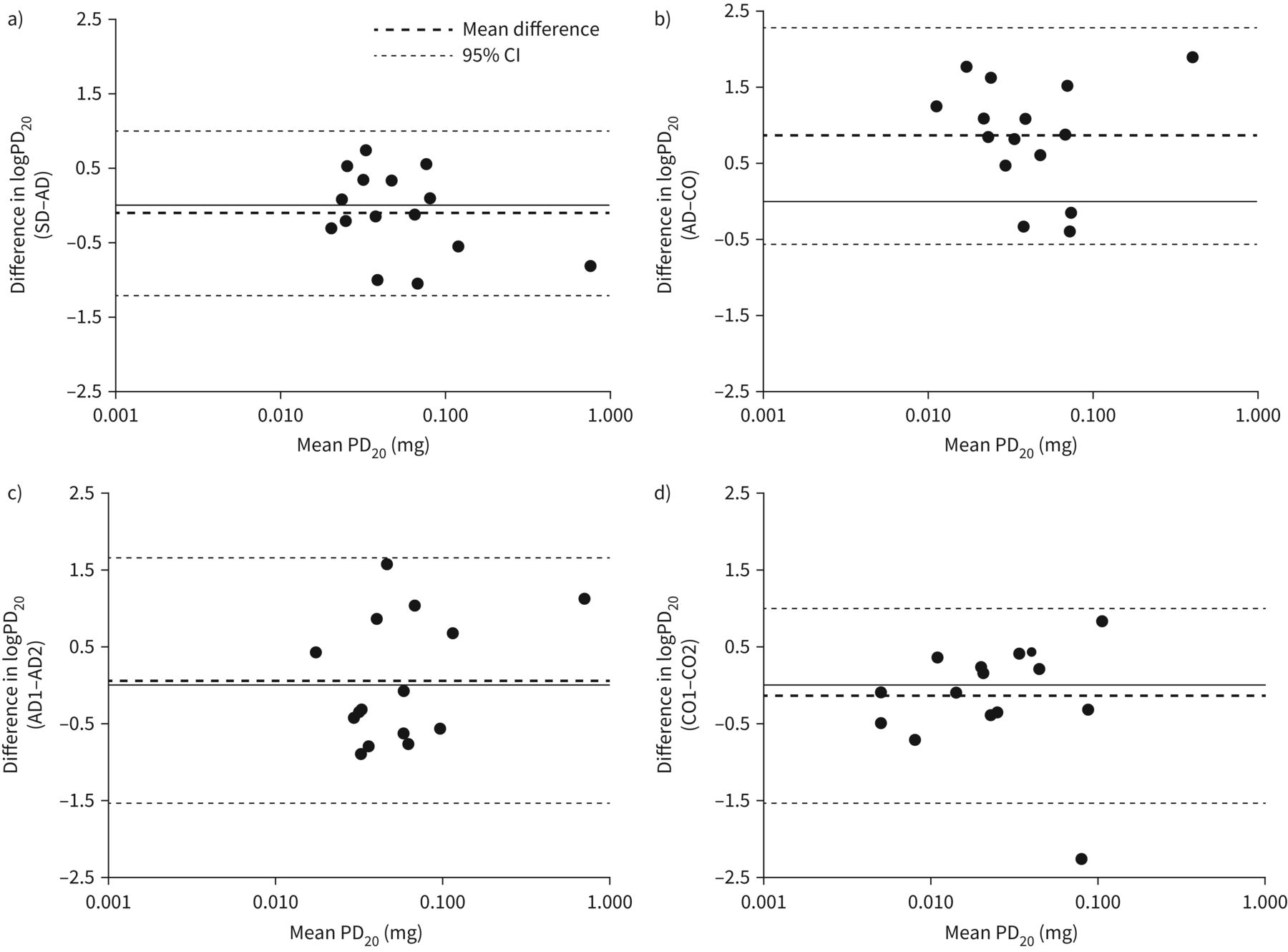
The results from the AD challenge were similar to the SD challenge (figure 2). The ratio of the SD challenge PD20 to the AD challenge PD20 was 0.90 (95% CI 0.66–1.23, p=0.49), and the results from these different protocols had an excellent correlation (ICC 0.82). The Bland–Altman plot (figure 3a) showed that the limits of agreement on the log scale were from −1.21 to 1.00, which (back-transformed) gave ratios between challenges of 0.30–2.73 (SD:AD).

Cumulative dose causing a 20% reduction in forced expiratory volume in 1 s (PD20) values for the standard dosimetric challenge (SD) and the adjusted dosimetric challenge (AD).
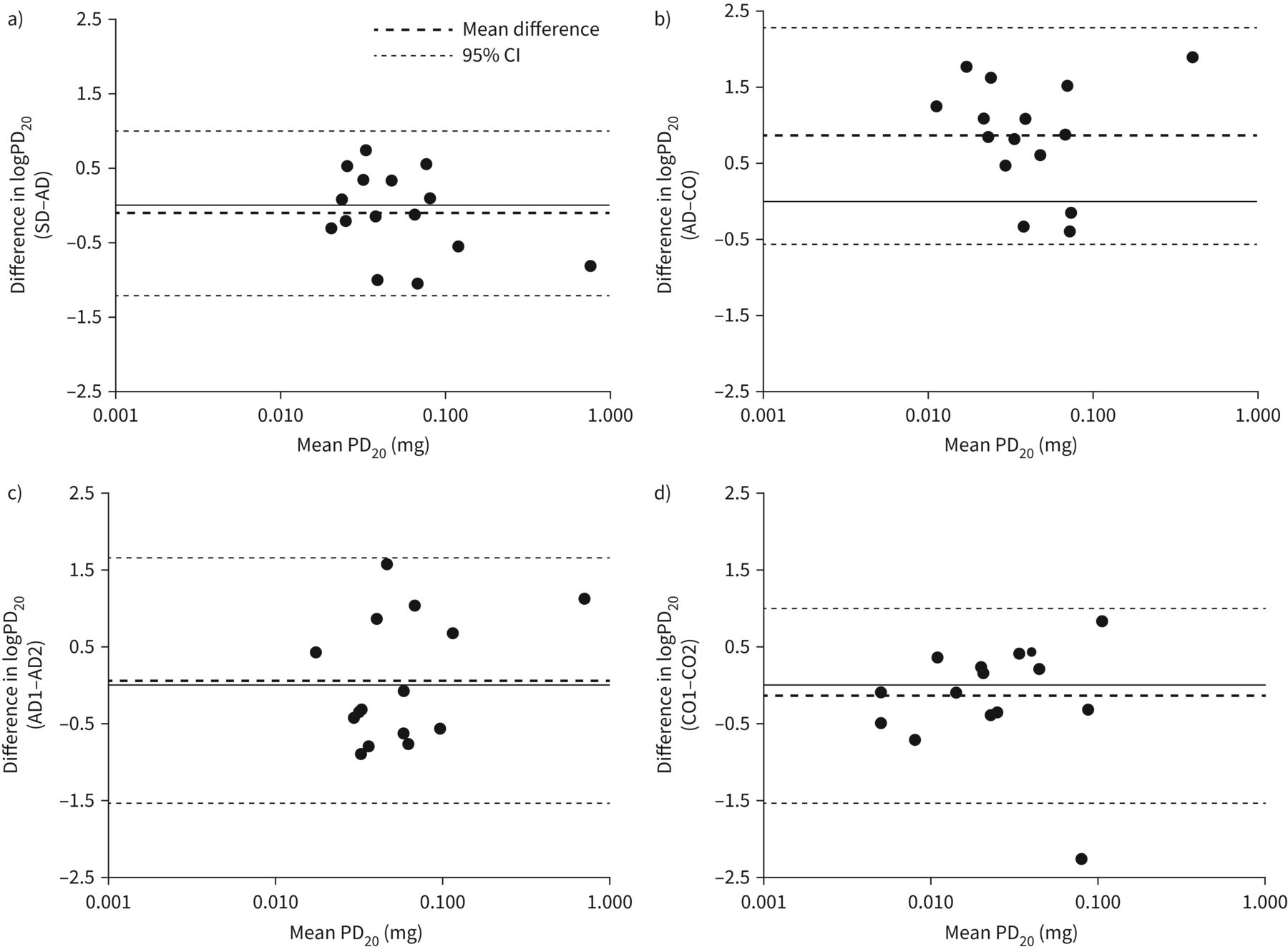
Bland–Altman plots for comparison of challenge methods. a) Standard dosimetric challenge (SD) versus adjusted dosimetric challenge (AD); b) averaged AD challenges (mean of two tests) versus averaged continuous-output breath-actuated challenge (CO) challenges (mean of two tests); c) the first AD challenge versus the second AD challenge; d) the first CO challenge versus the second CO challenge. y-axis is reported as the log (natural) difference in cumulative dose causing a 20% reduction in forced expiratory volume in 1 s (PD20) values between the two values.
Comparison of AD and CO protocols
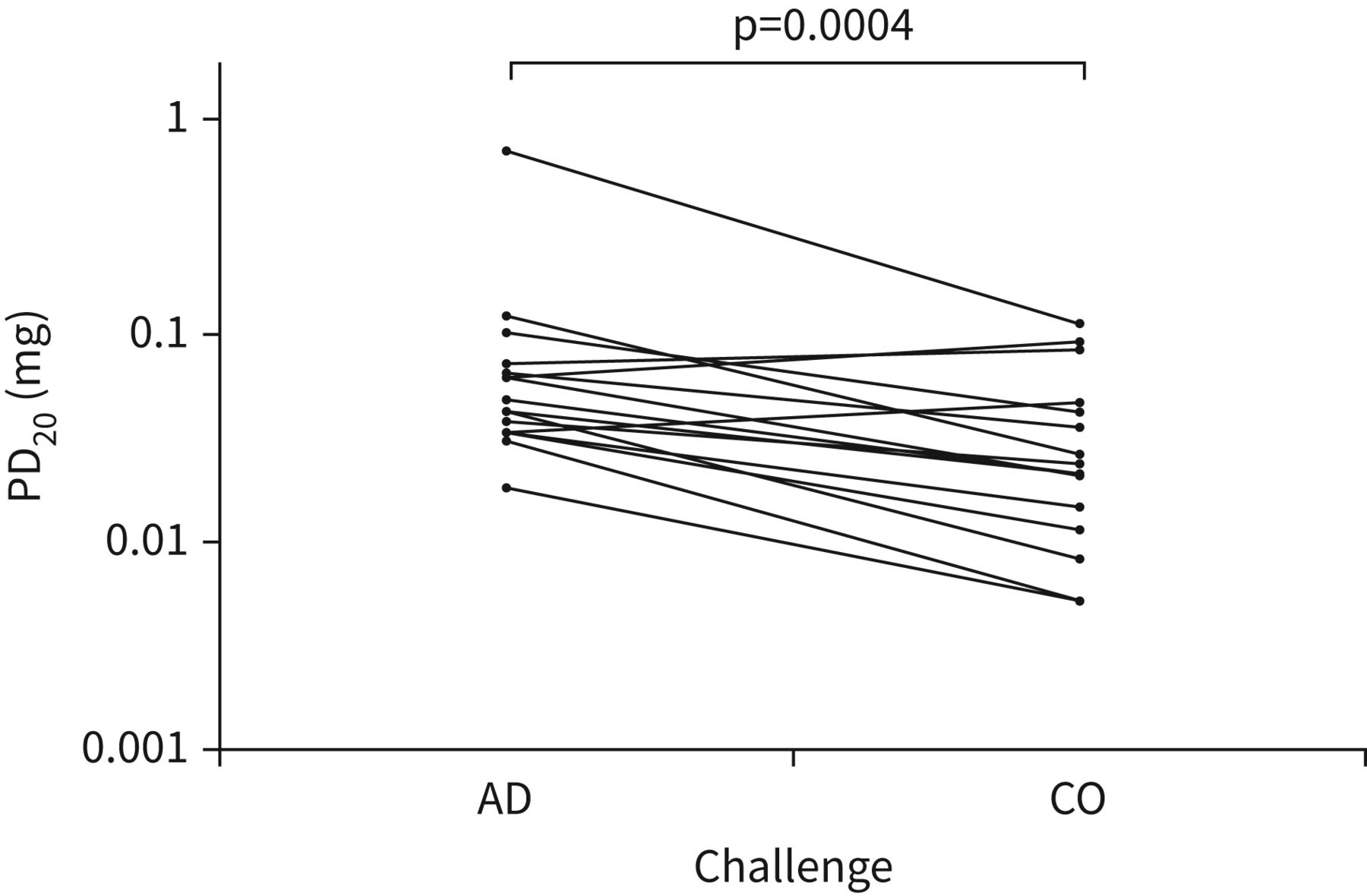
The results from the AD challenge were higher than the CO challenge (figure 4). The ratio of the AD challenge PD20 to the CO challenge PD20 was 2.31 (95% CI 1.57–3.40, p=0.0004). There was a correlation between the methods (ICC 0.65). The Bland–Altman plot (figure 3b) showed that the limits of agreement on the log scale were from −0.57 to 2.28, which (back-transformed) gave ratios between challenges of 0.57–9.78 (AD:CO).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Averaged cumulative dose causing a 20% reduction in forced expiratory volume in 1 s (PD20) values (mean of two tests) for the adjusted dosimetric challenge (AD) and the continuous-output breath-actuated challenge (CO).
Repeatability
There were no differences between the first and second AD challenges (ratio 1.07, 95% CI 0.68–1.68; p=0.76). Furthermore, there were no differences between repeated CO challenges (ratio 0.86, 95% CI 0.58–1.29; p=0.45). The ICC value for the AD protocol was 0.62, and for the CO protocol 0.74. The repeatability between the first and repeat challenge was ±1.61 DD for the AD protocol and ±1.45 DD for the CO protocol. 87% and 93% of patients were within 1.5 DD on repeat, for the AD protocol and CO protocol, respectively. The Bland–Altman plots (figure 3c and d) of the repeated challenges showed that the limits of agreement on the log scale were from −1.53 to 1.66 for the AD challenge, and −1.56 to 1.27 for the CO challenge. When back-transformed, these gave ratios for the first challenge versus the second of 0.22–5.25, and 0.21–3.55, respectively.
Discussion
We have demonstrated that an AD challenge, where concentration and nebuliser output were altered to increase dose, produced similar results to challenge methodology where only concentration was increased. The results from this AD challenge methodology correlated (ICC 0.65) with results obtained from the CO method supported by current ERS guidelines. However, the AD challenge gave higher PD20 values, therefore reporting patients as being less hyperresponsive. Therefore, the AD and CO challenge methods are not interchangeable in clinical trials. Nevertheless, the variability of repeated AD and CO challenges was similar.
We compared two methods of incremental dosing using the same equipment (SD versus AD). Similar PD20 results were obtained by increasing the concentration or duration of exposure to methacholine. Adjusting the duration of the nebuliser output has several practical advantages over increasing the concentration; challenges can be completed in a faster time, as removing frequent concentration changes streamlines the procedure. This affords the operator more time to ensure adequate spirometry results are obtained during the procedure. There are also important cost advantages as less methacholine solution needs to be prepared.
The PD20 for AD challenge was different to the CO method. In contrast, previous studies have reported that methacholine PD20 was not affected by the challenge method [6, 7, 15], but these previous observations are not generalisable to all challenge protocols. Regarding the challenge methods used in our study, the respirable delivered dose for the CO method has previously been estimated by calculating the respirable fraction (defined as particles <5 μm in size) using nebulised methacholine itself [12]. In contrast, the respirable fraction from the 8900 nebuliser used for the dosimetric methods has been estimated using nebulised saline, primarily due to lack of any data for methacholine output with this system. The respirable fraction is reported to be as high as 97–98% with saline for the dosimetric nebuliser [16], while Hatley and Byrne [17] found this to be as low as 30% with salbutamol sulfate. This indicates that saline data may overestimate the respirable fraction of methacholine administered. The continuous-output nebuliser has been shown to have similar respirable fractions with salbutamol sulfate (73%) [17] and methacholine (76%) [12]. Hence it is likely that the respirable fraction of methacholine produced by the AD nebuliser is lower than calculated, resulting in the higher PD20 values obtained. This underscores the importance of quantifying the respirable fraction for specific nebulisers using methacholine itself in future.
It is important to know the within-subject variability of repeated methacholine challenges in clinical trials, as this influences statistical power. We investigated whether improved (theoretically at least) control of dose using the AD method would result in less variability compared to the CO method (which may be affected by the patient's tidal volume and frequency). We found that dosimetric control did not improve the repeatability of a tidal breathing challenge, with majority of patients within ±1.5 DD on repeat for both methods. The Bland–Altman plots also showed similar levels of agreement for repeated challenges with these different methods. This suggests that inherent within-subject variability is the predominant factor in determining response to methacholine, and that the contribution of tidal volume and frequency is only minor.
The threshold of ±1.5 DD to define a clinically acceptable difference between methacholine challenges is stated in previous guidelines, based on 95% confidence intervals of ±1.5 DD [8]. This threshold has been used practically as a benchmark for identifying variability resulting from the equipment and/or the procedure used. Changes beyond this level on an individual basis may be clinically meaningful and have implications for clinical management. The analysis of repeated challenges with the AD method and repeated challenges with the CO method reassure that the variability of the methods is generally within the 1.5 DD difference.
There were a number of limitations to our study. Randomisation was only performed between the first two challenges, to compare the two dosimetric protocols. This approach was chosen in order to reduce the variability in timeframe between repeated challenges, which would have been larger if all visits were randomised. Our sample size was 15 patients, and replication with larger groups would be of value.
Conclusion
In conclusion, this study reports a tidal dosimetric methacholine challenge using adjustment of nebuliser output can be used to obtain results with good repeatability. This is a practical and cost-saving method for use in clinical trials and clinical practice. Interestingly, the results of the AD method differed from the CO method, underscoring that the results of different methacholine challenge methodologies may not be directly comparable.
Acknowledgement
The authors would like to thank Lucy Connor (Medicines Evaluation Unit, Manchester, UK) for her assistance during data collection.
Footnotes
Provenance: Submitted article, peer reviewed.
Ethics approval and patient consent: All patients provided written informed consent using a protocol approved by Greater Manchester East Research Ethics Committee (05/Q1402/41).
Availability of data and material: The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author contributions: J. Dean and D. Singh were the major contributors to study design, interpretation of the data and writing the manuscript. All authors contributed to collection and analysis of the patient data, and read and approved the final manuscript.
Conflict of interest: J. Dean declares no competing interests.
Conflict of interest: N. Jackson declares no competing interests.
Conflict of interest: B. Keidel-Morgan declares no competing interests.
Conflict of interest: D. Hamer declares no competing interests.
Conflict of interest: D. Singh has received sponsorship to attend international meetings, honoraria for lecturing or attending advisory boards, and research grants from Aerogen, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, CSL Behring, Epiendo, Genentech, GlaxoSmithKline, Glenmark, Gossamerbio, Kinaset, Menarini, Novartis, Pulmatrix, Sanofi, Teva, Theravance and Verona.
Support statement: The study was funded by the Medicines Evaluation Unit.
- Received April 23, 2021.
- Accepted August 4, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org










