





Abstract
Aim The aim of this study was to investigate occupational, environmental, early life and other risk factors associated with respiratory infections and antibiotics use in a general population and among asthmatic individuals.
Method This study included 15 842 participants of the Respiratory Health in Northern Europe (RHINE) study aged 25–54 years from five Nordic countries, who answered a questionnaire covering respiratory outcomes, exposures, demographic characteristics and numbers of infections and courses of antibiotics in the last 12 months. Multiple logistic regression with and without adjustment for age, sex, smoking status, body mass index and centre were used to study the risk of infection and antibiotics in relation to asthma, and also the association between infection and antibiotics and occupations.
Results In the whole population, 11.6% reported having three or more respiratory infections, and 14.7% had used antibiotics because of respiratory tract infections within the last year. Asthmatic participants reported tripled odds for such infections (adjusted OR 2.98, 95% CI 2.53–3.52) and antibiotics use (adjusted OR 3.67, 95% CI 3.18–4.24) as compared to non-asthmatic participants. Both in the general and the asthmatic population, female sex, obesity and exposure to building dampness were associated with respiratory infections. Female sex and current smoking and living in Tartu were associated with antibiotic use. The use of antibiotics was doubled in people hospitalised for severe respiratory infection in childhood.
Conclusion In this study we identified several factors associated with increased respiratory infections and use of antibiotics in a general population and among asthmatic individuals. The frequency of respiratory infections and subsequent antibiotic treatment were increased among those with asthma.
Abstract
The main findings of this study are that asthmatics reported three times higher odds for respiratory tract infections and more than three times higher odds for subsequent antibiotics than subjects without asthma https://bit.ly/3hwsH67
Introduction
Acute respiratory tract infections are a main cause of morbidity and mortality globally [1] and a leading cause of ambulatory consultation and work sick leave [2, 3]. The majority of respiratory tract infections are caused by virus [4]. Virus respiratory tract infections or colds are estimated to occur on average 2–5 times per year in adults [5]. Respiratory tract infections may be attributed to >200 types of virus or bacteria, with different clinical manifestation from being asymptomatic to fatal [6]. Many patients with respiratory tract infections are treated with antibiotics [7] despite the fact that viruses, and not bacteria, are the most common cause [8]. This results in an overuse of antibiotics [9] with negative consequences, including antibiotic resistance and adverse drug events [10].
Individuals with respiratory disease, including asthma, may be particularly vulnerable to respiratory tract infections [11, 12]. Other confirmed or suspected risk factors for respiratory tract infections in adults are active and passive smoking [13, 14], low serum vitamin D levels [15], lack of physical activity [16], children in household at daycare [17], sudden changes of temperature at work [18], lack of handwashing, psychological stress, shift work [19, 20], and duration and quality of sleep [21]. A review concluded that occupational exposure to various physical, chemical and other hazards might trigger exacerbations in people with asthma [22–24]. Obesity and Type 2 diabetes are also associated with higher susceptibility for respiratory tract infections [25, 26]. People living in the Nordic countries tend to have more respiratory tract infections, possibly due to exposure to low temperatures [27] and low vitamin D levels during the winter [28].
The aim of this study was to investigate how occupational, environmental, early life and other risk factors were associated with respiratory tract infections and subsequent antibiotics use in a general population and among asthmatic individuals.
Material and methods
Study design and population
This study is based on subjects that participated in the second survey of the Respiratory Health in Northern Europe study (RHINE) II (www.rhine.nu). The participants from five Northern European countries, Norway (Bergen), Sweden (Umeå, Uppsala, Gothenburg), Iceland (Reykjavik), Denmark (Aarhus) and Estonia (Tartu), answered a questionnaire in 1999–2001. The data collection procedure has been described elsewhere [29, 30]. A total of 15 842 subjects (born between 1945 and 1973) answered a postal questionnaire [31]. RHINE II is a followed-up study of participants from the European Community Respiratory Health Survey (ECRHS) that took place between 1990 and 1994 [32].
Questionnaire
Sociodemographic data included age and sex. Smoking history was based on the question “Do you smoke? Yes (current smoker)/No; If No, are you an ex-smoker? Yes (ex-smoker)/No (never-smoker)”. Socioeconomic index was calculated based on the participant's current or most recent occupation: 1 – managers and professionals, non-manual as legislators, senior officials, managers and professional; 2 – other non-manual as technicians and associate professionals, clerks, service workers and market sales workers; 3 – skilled manual as skilled agricultural and fishery workers and craft and related trades workers; 4 – semi-skilled or unskilled manual as plant and machine operators and assemblers and elementary occupations; 5 – unclassifiable or unknown including housewife, student, not classifiable job, unemployed, not working because of poor health and retired. [33]. The number of children under 7 years old in the household was reported. Body mass index (BMI) was calculated from reported height and weight and stratified into four groups: <20, 20–25, 26–30, >30 kg·m−2. The participants also answered questions on morbidities such as allergic rhinitis (self-reported previous nasal congestion without a cold and coexistent allergy), diabetes, hypertension and heart disease. Childhood history of otitis and hospital admission because of severe respiratory infection was reported.
Asthma definition
Subjects were considered to have current asthma if they reported that they currently were using asthma medication and/or had had an attack of asthma in the past 12 months [34, 35]. Information on asthma symptoms such as wheeze and nocturnal symptoms within the last 12 months was also reported.
Occupational and environmental exposure
The occupations reported by subjects were coded in accordance with the International Standard Classification of Occupations (ISCO-88) by an experienced occupational hygienist (ADH) [36]. These codes were connected to an asthma Job Exposure Matrix (JEM) based on exposure patterns from the Nordic counties [32]. JEM classifications included high molecular weight agents (HMW), low molecular weight agents (LMW) and irritating agents [31]. In addition, we included self-reported exposure to dampness and mould defined as visible water damage, visible mould or smell of mould in the last 12 months [37].
Main outcome variables
The two infection variables assessed were based on the following questions:
1) How many respiratory tract infections have you had in the last 12 months? (the number was classified as “less than three” and “three or more than three”);
2) Have you had any antibiotics for respiratory tract infection in the last 12 months? Yes/No
The presented analyses included participants that had answered at least one of the infection questions (n=15 842).
All participants gave written informed consent. The study was approved by the regional committees of medical research ethics in Aarhus (reference number 2011/M-20110106), Bergen (reference numbers 42.91, 149.2000 and 2010/759), Reykjavik (reference number VSNb2011090016/03.15), Tartu (reference numbers UT REC 60/3–1998, UT REC 209 T-17, UT REC 225/M-24) and Uppsala (reference numbers 1990/257, 1998/495 and 2010/068).
Statistics
The categorical variables were presented as prevalence with percentage, and the continuous variables were presented as mean with standard deviation (sd). Multiple logistic regression models with and without adjustment for selected confounding factors such as age, sex, smoking status, BMI and centre were used to study the association infection/antibiotics and asthma, as well as the association between infection/antibiotics and the JEM-assessed occupational exposures and self-reported exposure factors. The results of the regression analysis were presented as odds ratios with 95% confidence intervals. All statistical analysis was performed with R program version 4.0.2, applying a 5% level of significance.
Results
Characteristics of the study population
Of the 15 842 participants included in the study, 53% were women, and the age span was between 25 and 54 years. Around half of the population had a BMI between 20 and 25 kg·m−2 and were never-smokers. The prevalence of asthma was 6.6%. Other characteristics are presented in table 1.
Characteristics of the study population according to study centres
Infections and antibiotics
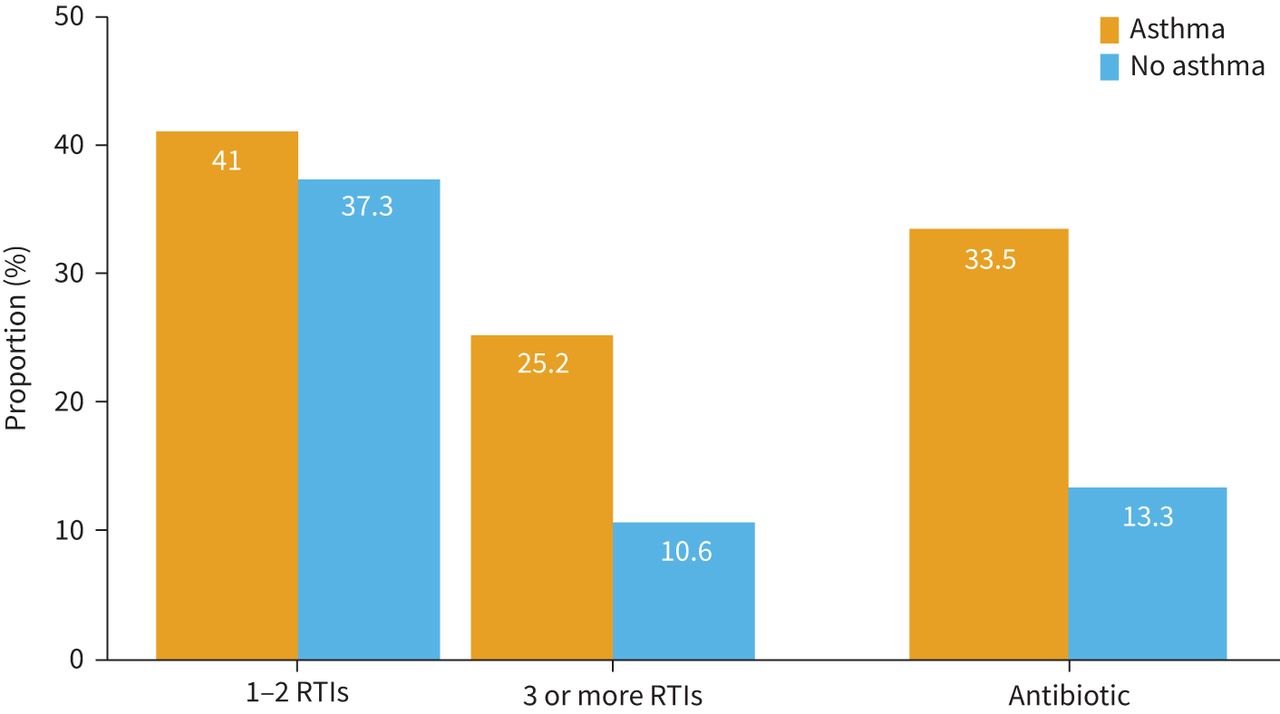
In the whole population, 11.6% reported having three or more respiratory tract infections and 14.7% had used antibiotics because of a respiratory disorder within the last 12 months. Both respiratory tract infections and the use of antibiotics was significantly more common in subjects with asthma (figure 1, table 2, Supplemental Table 1).

The occurrence of self-reported respiratory tract infections (RTIs) (one to two times or three or more times or no infection) and the use of antibiotics for respiratory tract infections (at least once, no antibiotic) in the past 12 months in asthmatic and non-asthmatic subjects.
Multiple logistic regression models for respiratory infections (at least three or more) and antibiotic (any) use for respiratory infections in the whole population in the past 12 months, adjusted for age, sex, smoking status, body mass index and centre
Factors associated with respiratory infections in the general population and asthmatic subjects
Multiple logistic regression models with adjustment to age, sex, smoking status, BMI and centre showed that subjects with asthma had almost a three-fold increased odds ratio for respiratory tract infections in the past year compared to non-asthmatic subjects (table 2). The odds for antibiotic treatment were about 3.5 times higher in asthmatic than in non-asthmatic subjects.
Women with and without asthma reported more respiratory tract infections and antibiotic use than men (tables 2 and 3). In the general population, the frequency of reported respiratory tract infections occurred less with increasing age. In contrast, in asthmatic subjects, the odds of respiratory tract infections and antibiotics increased with age. The odds for respiratory tract infections and antibiotics increased with decreasing socioeconomic status and low education in the general population. Overweight (BMI >30 kg·m−2) and underweight (BMI <20 kg·m−2) were associated with a higher occurrence of respiratory tract infections and antibiotic treatment in people with and without asthma. Daily smokers used antibiotics to a higher extent compared to ex- and never-smokers.
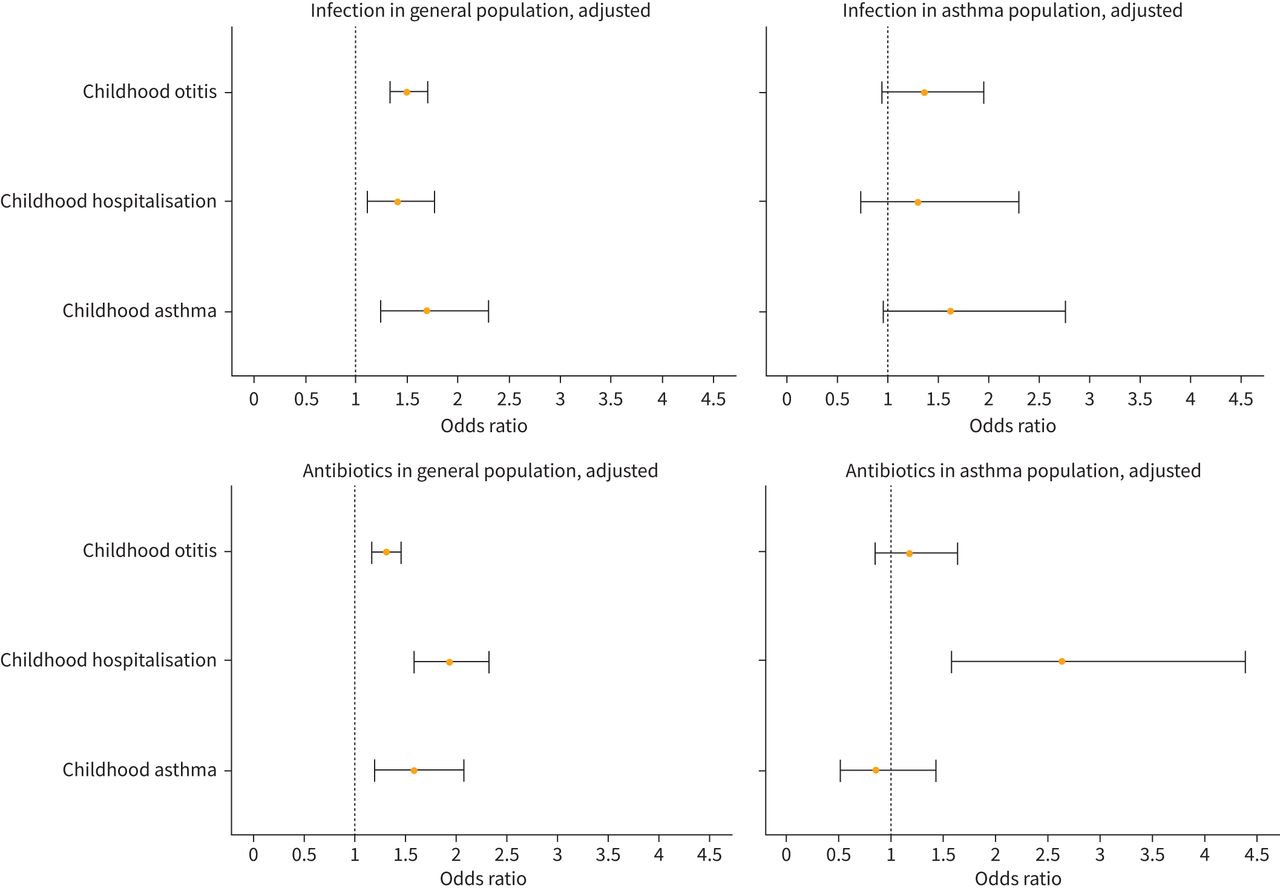
Subjects with asthma, allergic rhinitis, heart disease, hypertension and diabetes mellitus had increased odds of respiratory tract infections and antibiotic use (table 3). In asthmatic subjects, the coexistence of heart disease particularly increased the odds of respiratory tract infections. Also, participants with asthma that reported wheeze and night symptoms had a higher occurrence of respiratory tract infections and the use of antibiotics. The highest occurrence of respiratory tract infections and use of antibiotics was reported by subjects from Tartu in both study populations (table 3). All study subjects who had been hospitalised due to severe respiratory infections or had had otitis in childhood had increased odds of respiratory tract infections and use of antibiotics in adulthood (figure 2, supplementary Table 3) and the differences varied between the centres. In the general population, early life infection increased the presence of respiratory infection in adulthood in particularly in Gothenburg, Uppsala and Aarhus (supplementary table 4A), whereas the highest use of antibiotics in adults was seen in subjects that reported early life infection in Aarhus and Bergen (supplementary table 4B).
Multiple logistic regression models for respiratory infections (at least three times) and antibiotic use (at least once) in the subjects with asthma

Multiple logistic regression models (odds ratio) for infection (at least three infections) and antibiotic (any) use in relation to childhood otitis, childhood hospitalisation and childhood asthma in general population and asthmatic subjects. Adjusted for age, sex, smoking status, body mass index and centre.
Occupational and environmental exposure in the general population and in asthmatic individuals
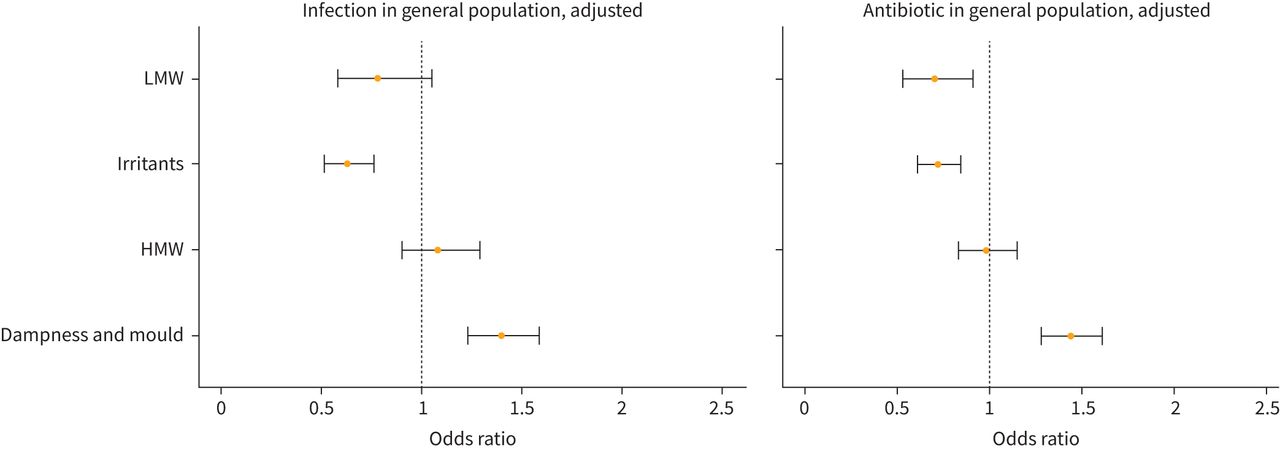
In the general population, exposure to dampness and mould was associated with more frequent respiratory tract infections and the use of antibiotics, whereas no associations were found for occupational exposure to LMW, HMW or irritants (figure 3, supplementary Table 2). Asthmatic individuals exposed to dampness and mould had a higher odds of respiratory tract infections. There was a borderline significant association between exposure to HMW (adjusted OR 1.58, 95% CI 0.98–2.54) and respiratory tract infections and exposure to dampness and use of antibiotics (adjusted OR 1.37, 95% CI 0.97–1.93) in the asthmatic population (figure 3, supplementary Table 2).

{kind=link}
{kind=link}
{kind=link}
Multiple logistic regression models (odds ratio) for infection (at least three infections) and antibiotic (any) use in relation to occupational and environmental exposure (in the past 12 months) in general population and asthmatic subjects. Adjusted for age, sex, smoking status, body mass index and centres. LMW: low molecular weight agents; HMW: high molecular weight agents.
Discussion
The main findings of this study are that asthmatic subjects reported three times higher odds for respiratory tract infections and more than three times higher odds for subsequent antibiotics than subjects without asthma. Female sex, obesity and exposure to building dampness were independently associated with respiratory tract infections, and female sex, current smoking and living in Tartu increased the probability of antibiotic use both in the general and in the asthmatic population.
There are several reasons why participants with asthma report more respiratory infections and higher use of antibiotics than those without asthma. Several studies have shown that asthma is associated with a dysregulation of the immune response and impaired production of antiviral interferons [38]. Participants with asthma are also more likely to have severe respiratory symptoms during an infection, which may increase the likelihood of getting antibiotics prescribed. It is also possible that persons with asthma are more aware of infections, which could lead to over-reporting.
In the present study, 33% of participants with asthma had used antibiotics because of respiratory infection within the last year. The increased prevalence of use of antibiotics for respiratory infection in asthma in our study is in accordance with a previous study based on an antibiotic register that reported a more frequent prescription of antibiotics in asthmatic compared to non-asthmatic patients from France and Italy [12]. The high use of antibiotics in asthmatic participants in our study is also in accordance with data from a trial in the UK where 45% of asthma patients received antibiotics for exacerbations in primary care [39].
We also showed that the probability of frequent respiratory tract infections and the use of antibiotics varied in different research centres. Reported respiratory tract infections and antibiotic use were the highest in Tartu, Estonia and the lowest in Umeå, Sweden. This is in accordance with our previous study using IgG measurement, where we found that there were geographical differences with a higher infectious burden in Estonia than in Sweden and Iceland [40]. Another study on infections in children reported that the use of antibiotics was two times higher in Estonian children compared to Swedish children [41]. The higher prevalence of infections in children might be explained by the hygiene hypothesis, which suggested that a low exposure to microbes in early life disables the maturation of the immunological system [42]. The geographical difference in reported infections and antibiotics could also be explained by the combination of different factors such as genetic susceptibility, geographic variations in resistance level and difference in adherence to guidelines [42, 43].
In this study, women report respiratory tract infections and antibiotic use more often than men. Our results are in line with a previous study where significantly more females than males (both asthmatic and non-asthmatic subjects) were prescribed antibiotics in both France and Italy [12]. On the contrary, females were significantly less likely, in comparison to males, to be prescribed antibiotics in both asthmatic and non-asthmatic subjects in the UK [11].
In this study, individuals with lower socioeconomic status tend to report more infections and use of antibiotics. It was previously shown that sociodemographic factors including educational level, income and occupation influence the prevalence of infectious disease [44]. We found that current smokers used more antibiotics because of respiratory tract infections. This is in accordance with previous studies reporting that active smoking and passive smoking had an increased incidence of upper respiratory tract infections [45, 46]. It was also shown that nonsmokers and ex-smokers were more vulnerable to tobacco smoke than active smokers that were more adapted [13]. In a previous analysis of part of this population, we also found that smoking increased the likelihood of having been hospitalised for pneumonia [47].
We also showed that having allergic rhinitis increased the odds of respiratory tract infections and antibiotic use. There are several potential causal relationships between atopic conditions and microbial infections: protective (hygiene hypothesis), provocative (rhinovirus or bacterial colonisation), microbiome hypothesis and reverse causality (the risk for infection in atopic conditions). Previous studies indicate that asthma exacerbation caused by virus infection may be more severe in patients with coexisting allergies [48, 49].
Obesity (BMI >30) was associated with higher odds for self-reported respiratory tract infections and the use of antibiotics in both the general and asthma population. Being underweight was linked to higher odds of respiratory tract infections and antibiotics in asthmatic individuals. We have, in previous analyses, found that both obesity and underweight increases the risk of hospitalisations for pneumonia [47]. In the present study, we found that having diabetes (OR 1.45, 95% CI 1.03–2.04) increased the likelihood of using antibiotics because of associations with respiratory tract infections. This is in accordance with previous studies [50]. We also found that cardiovascular conditions were associated with more reported respiratory tract infections and the use of antibiotics. Previous studies showed that cardiovascular disease was associated with an increased risk of respiratory tract infections [51, 52].
We found that childhood hospitalisation for respiratory infections before age 2 years and frequent otitis were associated with higher odds for respiratory tract infections and the use of antibiotics in adulthood. It is notable that the associations with the use of antibiotics were more pronounced than the associations with respiratory tract infections; among asthmatic participants who had been hospitalised for respiratory infection in childhood, reported use of antibiotics was doubled while reported respiratory tract infections increased only insignificantly. A previous analysis on subjects from 22 counties found that adults reporting severe childhood respiratory infections had increased risk for asthma and wheeze as well as lower lung function in adulthood. Lower lung function was also shown in adults without asthma and wheeze who had severe respiratory childhood infection [53].
In our study, living in damp housing significantly increased the odds of respiratory tract infections and antibiotics compared to non-exposed in both asthma and the general population. This is in accordance with several previous studies showing that exposure to damp and mould is associated with a higher prevalence of respiratory symptoms and asthma [33] and a previous meta-analysis showing that residential dampness and mould were linked to a significantly higher risk of respiratory infections [54]. Environmental and occupational allergens may act in synergy with viral pathogens, damage airways epithelium and facilitate viral invasion [23, 24]. In turn, viral infection impairs antibacterial innate immune response [55] and increases bacterial adherence to bronchial epithelium [56].
In the present study, a borderline significant association was found between occupational exposure to HMW and respiratory tract infections in the asthmatic population. No significant association between occupational exposure divided into agents with different molecular weights and respiratory tract infections or use of antibiotics was found in the previous studies. Other studies have, however, found that certain kinds of occupational exposures increase the risk of pneumonia [57].
Strengths and limitations
This study has several strengths and limitations. A key strength was that we used a very large population of randomly selected subjects from different research centres in five Nordic countries. Also, the subjects answered detailed questionnaires that enable robust analyses with several important confounders.
One important limitation was that this study had only self-reported information from the RHINE standardised questionnaire and no objective clinical measures. The asthma diagnosis was not validated against medical records, and we also lacked information on asthma medication. This might lead to some degree of misclassification in the assessment of asthma. Furthermore, the cross-sectional analysis did not allow us to make any causal inference. Another weakness is that we did not have information on severe infections leading to hospitalisation. We also lacked drug prescriptions data and could not study whether asthma medication such as inhaled corticosteroids modified the risk of infection. However, it is the subjective symptoms that affect the individual's life and work status, and therefore the subjective outcome is more relevant for public health [58].
Conclusion
In this study, we identified several factors that may be considered to increase the risk of respiratory tract infections and the use of antibiotics in the general and the asthmatic population. Asthmatic individuals were at particular risk of respiratory tract infections and the use of antibiotics because of respiratory tract infections. Moreover, living in damp housing significantly increased the risk of respiratory tract infections and antibiotics compared to non-exposed in both the asthmatic and the general population. From a public health perspective, it might be important to consider strategies to reduce the rate of respiratory infections among asthmatic individuals and to pay specific attention to the overuse of antibiotics among asthma patients.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00429-2021.SUPPLEMENT
Footnotes
Provenance: Submitted article, peer reviewed.
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: M.A. Kisiel has nothing to disclose.
Conflict of interest: X. Zhou has nothing to disclose.
Conflict of interest: E. Björnsson has nothing to disclose.
Conflict of interest: M. Holm has nothing to disclose.
Conflict of interest: A. Dahlman-Höglund has nothing to disclose.
Conflict of interest: J. Wang has nothing to disclose.
Conflict of interest: C. Svanes has nothing to disclose.
Conflict of interest: D. Norbäck has nothing to disclose.
Conflict of interest: K.A. Franklin has nothing to disclose.
Conflict of interest: A. Malinovschi has nothing to disclose.
Conflict of interest: A. Johannessen has nothing to disclose.
Conflict of interest: V. Schlünssen has nothing to disclose.
Conflict of interest: C. Janson has nothing to disclose.
Support statement: The study was funded by the Swedish Heart and Lung Foundation; the Swedish Association Against Asthma and Allergy; the Swedish Association against Heart and Lung Disease; the Swedish Council for Working Life and Social Research; the Bror Hjerpstedt Foundation; the Faculty of Health, Aarhus University, Denmark (project number 240008); the Wood Dust Foundation (project number 444508795); the Danish Lung Association; the Norwegian Research Council project 135773/330; the Norwegian Asthma and Allergy Association; the Icelandic Research Council; and the Estonian Science Foundation (grant number 4350). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received June 28, 2021.
- Accepted September 9, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










