





Abstract
Addition of intravenous amikacin and clofazimine to recommended rifamycin-ethambutol-macrolide regimens yields favourable outcomes in severe M. avium complex pulmonary disease (MAC-PD). This five-drug regimen should be considered in select MAC-PD patients. https://bit.ly/30dxdRj
To the Editor:
Mycobacterium avium complex (MAC) bacteria, i.e. Mycobacterium avium, Mycobacterium intracellulare, Mycobacterium chimaera and related species, can cause severe pulmonary disease (MAC-PD), especially in patients with chronic pulmonary diseases, like COPD and bronchiectasis [1, 2].
Treatment of MAC-PD is difficult due to its long duration, frequent adverse events and comorbidities of the host. Reported cure rates vary by disease manifestation, with poorest cure rates in fibrocavitary disease [3]. The currently recommended treatment for MAC-PD is a combination of a rifamycin (R), ethambutol (E) and a macrolide (M), preferably azithromycin [4]. In severe disease, amikacin (A) can be added to improve treatment outcome, but there is no direct evidence to support its role [4].
Clofazimine (C), an old anti-leprosy drug, may add efficacy to MAC-PD treatment regimens. In vitro, clofazimine shows synergy with amikacin and macrolides against MAC [5, 6]. In retrospective studies, the outcomes of treatment regimens in which clofazimine replaces rifamycin are similar to those of the recommended REM regimen [7–9].
In our nontuberculous mycobacterium (NTM) reference clinic, patients with severe MAC-PD have been receiving intensified treatment with the REMAC regimen since 2013. Here, we evaluate its outcome, as compared to a cohort that only received the REM regimen.
We conducted a retrospective cohort study of adults (>18 years) with macrolide-susceptible MAC-PD diagnosed according to current guidelines [4], treated from January 2007 until January 2017 in our reference clinic (last check: March 2021). A waiver from the local ethical board has been given for this retrospective study. Patients were classified into two groups: the REM group and the REMAC group. Amikacin was given intravenously at a 15-mg·kg−1 initial dose with therapeutic drug monitoring and clofazimine was dosed at 100 mg once daily. We collected demographic and treatment related data from the electronic medical records. Disease was classified as fibrocavitary or nodular–bronchiectatic and followed up on basis of chest computed tomography reports and a second assessment by two expert pulmonologists (C. Magis-Escurra and W. Hoefsloot). Disease severity and thus indication for REMAC treatment was assessed by the multidisciplinary team (all authors) on the basis of symptoms, immune status, frailty, extent of radiological abnormalities and microbiology (i.e. sputum smear status and quantitative culture).
Patients who received either amikacin or clofazimine, or who used amikacin for <2 weeks were excluded from the analysis.
Primary outcome measurements were time until sputum culture conversion and cure rates. Outcomes were defined using the NTM-NET definitions [10], except that microbiological cure and culture conversion were defined by two, rather than three, consecutive negative cultures.
Treatment duration was calculated continuously from the treatment start date.
Pearson's Chi-squared test or Fisher's exact test were performed for all outcome parameters. Time to sputum conversion was analysed with a log-rank test resulting in a survival analysis with a Kaplan–Meier curve. All analyses were performed using SPSS (version 25).
44 patients were included: 25 patients who received REM and 19 patients who received the REMAC regimen. Baseline characteristics were similar between both groups considering sex, age, underlying pulmonary diseases, history of smoking and causative MAC subspecies (table 1). Although not statistically significant, a trend towards more frequent fibrocavitary disease in the REMAC group was seen (79% versus 48% in the REM group, p=0.062).
Baseline characteristics, outcomes, radiological changes, side-effects and changes in therapy due to side-effects, stratified by treatment group
In the REMAC group, four patients received slightly different regimens; one was treated without a macrolide, two without a rifamycin and one without ethambutol, all because of toxicity or intolerance.
Median (range) treatment duration was 63 (35–90) weeks in the REM group versus 69 (36–103) weeks in the REMAC group. The mean±sd duration of amikacin use in the REMAC group was 11.1±5.9 weeks.
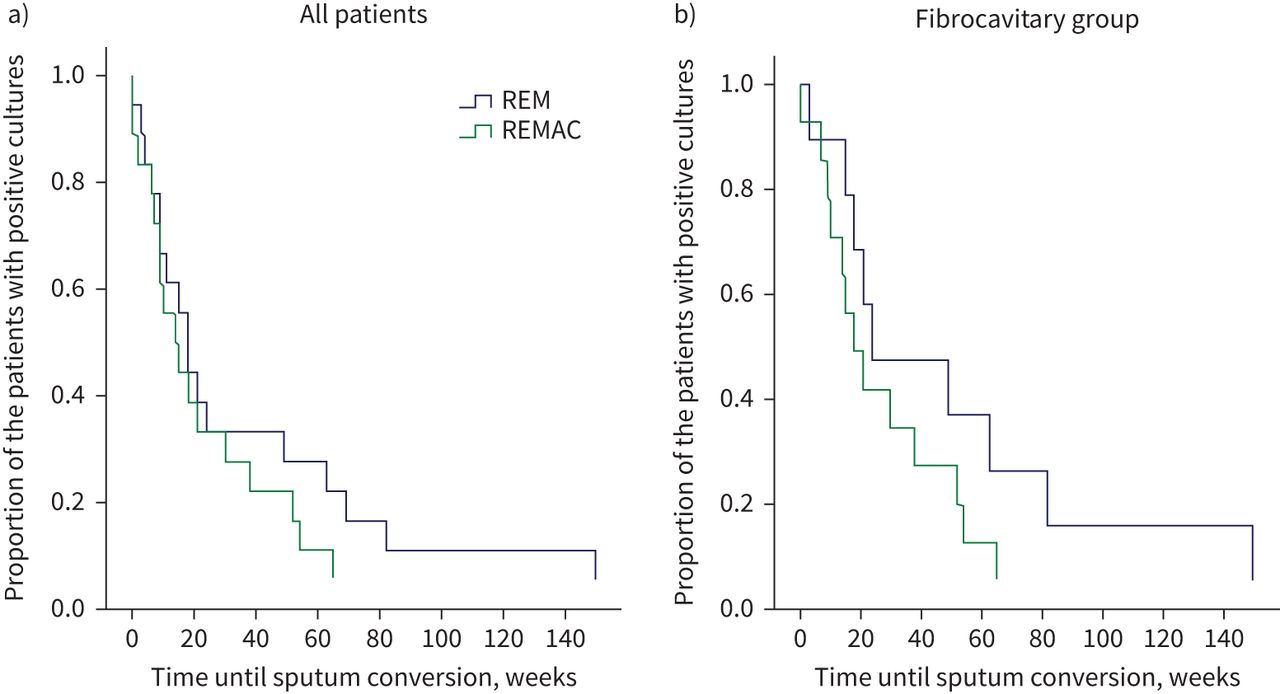
Sputum culture conversion was seen in 80.0% of the patients receiving REM, compared to 89.5% in the REMAC group (p=0.680). A trend towards longer median time to sputum culture conversion in the REM group (18 (9–27) weeks, p=0.247) than in the REMAC group (14 (6–22) weeks) (figure 1a) was observed. A subanalysis of patients with fibrocavitary disease showed a median time to sputum conversion of 24 (15–33) weeks for REM versus 18 (10–26) weeks for the REMAC regimen (p=0.154) (figure 1b).

{kind=link}
a) Time to sputum culture conversion of all patients, comparing rifamycin (R)–ethambutol (E)–macrolide (M) to REM–amikacin (A)–clofazimine (C) (p=0.247). b) Time to sputum culture conversion of patients with fibrocavitary pulmonary disease, comparing REM to REMAC (p=0.154).
In the REM group, 13 (52%) patients attained microbiological cure versus 14 (74%) patients in the REMAC group. Clinical cure was attained by a further seven (28%) patients in the REM group versus three (16%) patients in the REMAC group. In a subgroup analysis, excluding the four REMAC patients with alternative treatment regimens, microbiological cure rates did not differ between the groups (52% in the REM group versus 73% in the REMAC group, p=0.488). Treatment failure recurrence occurred in 20% (REM) and 11% (REMAC) of the patients. In both groups, two patients had recurrence after a mean follow-up of 31.8±34.1 months.
Adverse events were more frequent in the REMAC group in 84% of the patients, while it was reported in 56% in the REM group (p=0.046%). Perceptive hearing loss was reported in 37% and tinnitus in 42% of patients in the REMAC group, while it was never reported in the REM group. No renal toxicity was reported. Change of treatment regimen due to side-effects was more common in the REMAC group, occurring in 10 out of 19 patients in the REMAC group versus five out of 25 patients in the REM group (p=0.03). The main reason to stop amikacin was ototoxicity. In the REM group, clarithromycin was replaced by azithromycin in four cases and rifampicin was replaced by clofazimine in one case.
We observed a promising trend towards higher cure rates and faster culture conversion with the addition of clofazimine and amikacin to the standard REM regimen in the most severe MAC-PD group with fibrocavitary disease. Although this effect was not statistically significant, it might be clinically relevant, as severe fibrocavitary MAC-PD is associated with the poorest treatment outcomes [3, 4, 11]. Due to small numbers of patients, no statistical differences between these groups were seen and larger prospective studies need to be conducted to assess treatment outcomes with the five-drug REMAC regimen.
Our culture conversion rates are in line with those in the landmark clinical trial by Kobashi et al. [12], who found that addition of streptomycin to the RE–clarithromycin backbone yielded better short-term (71% versus 51% culture conversion) but equal long-term outcomes. This trial formed the basis of the current recommendation to add either streptomycin or amikacin to regimens of patients with severe MAC-PD [4]. The current cohort is the first to provide direct evidence for the role of amikacin in severe macrolide-susceptible MAC-PD, and supports and adds to the recent guidelines [4].
Microbiological cure rates in the REM group were similar to previously published cohorts with fibrocavitary disease and strikingly different from the 84–100% reported for nodular–bronchiectatic disease [3, 9, 13]. The microbiological cure rate observed in the REMAC group is more in line with results obtained in (milder) nodular–bronchiectatic disease, again emphasising its positive impact.
Even though cure rates are high for REMAC group, this coincides with more adverse events. Hearing loss and tinnitus were only recorded in the REMAC group. This is likely biased, as clinicians are probably more focused on detecting hearing loss in patients treated with amikacin and this group also is subjected to regular audiometry. In patients treated with macrolides, tinnitus and hearing loss has been reported in 10–13% of the patients [3]. In addition, changes to the treatment regimen were significantly more frequent in the REMAC group. The REMAC regimen is also more costly, in terms of a need for hospital admission and direct drug cost [14]. These and practical barriers to prolonged intravenous access might be partly overcome if amikacin liposome inhalation suspension, successful in treatment of refractory MAC-PD [15], proves to be as effective as intravenous amikacin therapy. The exact contributions of amikacin and clofazimine, or the synergy between them [5, 6], to the additive effect observed for the REMAC regimen remains unknown and a subject for further study.
In conclusion, the REMAC regimen leads to favourable treatment outcomes in a small cohort with severe MAC-PD and may be considered in selected severe or recurrent MAC-PD patients, yet the benefits should outweigh the economic and humanistic burden. Clinical trials are needed to evaluate the indication and performance of this regimen.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: S.M.H. Zweijpfenning has received a grant for unrelated research from Insmed.
Conflict of interest: S.E.P. Kops has nothing to disclose.
Conflict of interest: M.J. Boeree has nothing to disclose.
Conflict of interest: S. Kuipers has nothing to disclose.
Conflict of interest: J. van Ingen has nothing to disclose.
Conflict of interest: W. Hoefsloot has received a grant for unrelated research from Insmed.
Conflict of interest: C. Magis-Escurra has nothing to disclose.
Support statement: J. van Ingen was supported by a personal grant from the Netherlands Organization for Scientific Research (NWO/ZonMW grant Veni 016.176.024).
- Received July 15, 2021.
- Accepted October 7, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










