





Abstract
Background This nationwide study aimed to elucidate the incidence and clinical characteristics of tissue-verified sarcoidosis in Iceland. A secondary aim was to analyse sex differences and identify possible environmental factors contributing to the pathological process.
Materials and methods This is a descriptive study covering 36 years (January 1, 1981 through December 31, 2016). Histopathological reports and electronic hospital discharge registries were reviewed in context for granulomas and/or sarcoidosis. National data were used for comparison regarding smoking habits and occupation, adjusted for age, sex and year of diagnosis. The data were stored in FileMaker and calculations were made by extracting data from this database to the statistical software package R.
Results A total of 418 patients (54% females) were diagnosed with tissue-verified sarcoidosis. The incidence rate was 4.15/100 000/year, similar among females and males. The mean age at diagnosis was higher among females (53.0±14.2 years) than males (48.2±13.8 years). Fatigue was the most frequent single symptom (49.7%), but when all respiratory symptoms were grouped, they were the most frequent symptoms (60%). No significant difference was found between smoking status and sarcoidosis. Possible hazardous exposure in the workplace was reported by 19.4% of the cases.
Conclusion The incidence of sarcoidosis in Iceland was higher than in an Asian population where the same inclusion criteria were applied. The clinical picture diverges partly from that in the Asian population but resembles that among other Caucasians. Fatigue and respiratory symptoms were predominant. The biphasic pattern of age at disease debut seen elsewhere among females was not evident in Iceland.
Abstract
This paper describes a nationwide study on the incidence of tissue-verified sarcoidosis in Iceland, focusing on clinical symptoms, smoking and occupation. The incidence is low, and main symptoms are fatigue and symptoms of the respiratory tract. https://bit.ly/3ur6jk8
Introduction
Sarcoidosis is a multisystem, inflammatory disease in which non-caseating granulomas can invade almost any human body organ [1]. The diagnosis is established when clinical and radiological findings are supported by histological evidence of non-caseating, epithelial cell granulomas [2]. It is assumed that some microbial or non-organic antigens trigger an immune response in genetically susceptible individuals that leads to granuloma formation [3, 4].
The reported incidence of sarcoidosis varies widely among populations. In Japan the incidence is 0.8/100 000/year [5] and in Sweden 11.5–24/100 000/year [6, 7], and it is even higher amongst black females in the USA—107/100 000 in the 30- to 39-year age group [8]. Histological confirmation of sarcoidosis through tissue biopsy is the gold standard for diagnosis of sarcoidosis. However, most studies in this field include tissue and clinically verified cases [6–13]. To the best of our knowledge, very few studies are based solely on tissue-verified cases of sarcoidosis [9, 14–16]. Age at diagnosis has been widely studied and has often been described as biphasic, with a peak at young adult age (25–34 years) and a second peak later in life (50–65 years) [7, 13, 15, 17–19]. Clinical symptoms vary widely among different populations, ethnic groups, individuals and sexes [20]. In particular, in the USA, different phenotypic expressions are found between subjects of different origins, likely resulting from genetics, environment, socioeconomics, implicit or racial biases, or a combination thereof [21]. Persistent cough and fatigue are predominant symptoms, followed by skin, eye, neurological and joint manifestations [19, 20, 22, 23].
Imaging by chest radiograph [22, 24–26] and thoracic computer tomography and pulmonary function tests [25, 27] are used to stage disease activity. Scadding staging is historically the conventional method of staging sarcoidosis, using chest radiographs as a parameter. Pulmonary function tests are impaired in 20% of patients with Scadding Stage I but up to 40–80% in the stages with a higher Scadding score [28].
Many studies have shown clustering of sarcoidosis in certain occupations, such as nursing, teaching and firefighting [2, 29–32]. Clusters in families and even spouses have also been reported [2, 33–37]. A linkage between sarcoidosis and industrial organic dust [38] and silica has been suggested [39, 40], whereas smoking has been inversely linked to sarcoidosis [41, 42]. Seasonal variation in incidence has been reported, with peaks in late winter, early spring and summer compared to autumn [43, 44].
Iceland is an island in the North Atlantic; until recently, it had a homogenous Caucasian population. In 2019, the population of Iceland was 356 991, 77.6% of whom had no foreign background. In a study published in 1978, an analysis of all sarcoidosis cases known in Iceland (only 39 cases) showed that half of the patients had symptoms in the respiratory tract, while half complained of constitutional symptoms [45]. Another study of sarcoidosis in a silica plant in Iceland showed a higher incidence among silica workers than among a group living in the same area [40]. Iceland has extended registries and healthcare records that can be linked together through individual explicit security numbers. Based on this, we performed a nationwide study of all tissue-verified cases of sarcoidosis in Iceland, focusing on incidence, clinical characteristics, sex differences and environmental factors.
Materials and methods
Study subjects
All known histologically verified cases of sarcoidosis diagnosed over 36 years, from January 1, 1981 through December 31, 2016, were included in the study. The data were obtained by searching the word granuloma from databases of pathological laboratories during the study period (January 1, 1981 to December 31, 2016). The main author reviewed these and extracted those diagnosed with tissue-verified sarcoidosis. Also, an electronic search was done to find all those discharged with International Classification of Diseases (ICD)-9 and ICD-10 codes for sarcoidosis from Landspitali University Hospital in the study period. The main author read all the case's hospital charts and registered information on clinical symptoms, environmental factors, smoking habits, occupation, spirometry, laboratory data, Scadding Stage at diagnosis, the method used for tissue biopsy, treatment received at the time of diagnosis (and in some cases at a different timeframe after diagnosis) and the month of diagnosis (for seasonal variation). The Icelandic Bioethics Committee (VSN 99-069-V1-V2-S1) and the Icelandic Data Protection Authority (99080306) approved the study.
Study design
This is a descriptive study of sarcoidosis in Iceland. The main aim of this study was to elucidate the incidence and clinical characteristics of sarcoidosis in Iceland. A secondary aim was to analyse sex differences and identify possible environmental factors contributing to the underlying pathological process. The study group's smoking habits and occupations were compared to those in the general population for each year of the study period. Clinical data were collected from the patients’ clinical charts at the time of diagnosis.
Methods
In Iceland, three histopathology laboratories analyse all (except one dermatologist's laboratory) tissue biopsies taken in Iceland: The Department of Pathology, Landspitali University Hospital of Iceland (UHI), the Department of Pathology, Akureyri Hospital (AkH) and a private laboratory, The Histopathology Laboratory in Reykjavik (HLR). The study subjects were found by digitally reviewing all histopathology results involving the words granuloma and sarcoidosis, from January 1, 1981 to December 31, 2016, from the first three laboratories (UIH, AkH and HLR), seeking out those having tissue-verified sarcoidosis. Another source was an electronic registry of discharge diagnosis of sarcoidosis from the major hospitals in Iceland: UHI and AkH where those with tissue proven sarcoidosis were sought out.
In addition, we searched all outpatient and inpatient diagnoses of sarcoidosis from our hospital and found those who had been given the diagnosis at least two times. Our patient ICD-coded registry goes in part back to January 1, 1983 and in part from January 1, 1987. This was linked to our dataset, and those that were not accounted for were registered, aiming to find those with clinically diagnosed sarcoidosis. The search was based on the ICD 9th and 10th diagnostic registry using the following diagnostic codes: D135 and D86 with subclasses D86.0, D86.1, D86.2, D86.3, D86.8 and D86.9 [46, 47].
Clinical symptoms
Symptoms were classified into the following categories: I) respiratory symptoms (cough, expectoration, dyspnoea, chest pain), II) fatigue, III) fever, IV) arthritis, V) weight loss, VI) rash, VII) excessive sweating and night sweats, VIII) eye symptoms, IX) erythema nodosum, X) heart symptoms and finally XI) symptoms attributed to the nervous system (including, e.g., palpitations, headaches, cranial nerve affections and paraesthesia).
Environmental factors
Self-reported possible exposure to hazardous substances in the workplace or elsewhere, such as mould, fumes and hay dust, was registered. Connections with animals, either as pets in the home or as livestock, were also registered. Living in an urban or rural area at the time of diagnosis was noted. In evaluating seasonal variation, we registered in which month each case was diagnosed according to the date of the positive tissue biopsy, registered on the pathological report.
Smoking habits and occupation
Smoking history was classified as 1) nonsmoker, 2) previous smoker or 3) current smoker. The study group's smoking habits were compared to those of the Icelandic population, adjusted for the year of diagnosis, age and sex. The data for smoking in Iceland go as far back as 1989 and are stratified into age groups of 10 years and sex [48]. The relationship between smoking and sarcoidosis is presented as a boxplot. Information on occupations was obtained from hospital charts and classified using ISTARF-95, a modified version of The International Standard Classification of Occupations, ISCO-88 used by Statistics Iceland [49, 50]. The incidence rate of sarcoidosis was calculated from the number of workers in each work sector, stratified by age, sex and the year of diagnosis [50]. The results are shown as incidence in a bar chart.
Spirometry and blood tests
Spirometry values (forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and diffusion capacity of the lungs for carbon monoxide (DLCO)) were registered as normal if >80% of the predicted value using the standard international reference values used by the laboratories at the time of diagnosis. If an ECG was taken at the time of diagnosis, the outcome was noted. Values for standard blood tests taken in the timeframe of a week before or after biopsy-taking that confirmed the diagnosis of sarcoidosis were included, as were results for angiotensin-converting enzyme (ACE), according to international reference ranges used by the hospital laboratory.
Imaging and Scadding stages
In the case of classification into one of the five Scadding stages, the first author (SOH) reviewed all chest radiographs and/or reports on the first radiograph taken at the time of diagnosis and categorised those into appropriate Scadding stages if they were not registered as such in the hospital charts.
Diagnosis and treatment
The method for obtaining tissue biopsy that confirmed a histological diagnosis of sarcoidosis was registered. Information on treatment for sarcoidosis was obtained from hospital charts at the time of diagnosis and, for some cases, also at follow-up visits at our clinic.
Statistical analysis
All data were stored in FileMaker 4/8. Statistical analysis was performed using the statistical software package R. Welch's two-sample t-test and Fisher's exact tests were used for comparisons. A p-value <0.05 was considered statistically significant. The study data were stripped of information, allowing individual identification before the analysis of data began. Smoking in the study group was compared to that in the general population, taking year, age and sex into account. The same method was applied for occupation. For smoking habits, the distribution of incidence rates between groups was observed in a boxplot. For occupation, the incidence of each occupational sector in the study group was compared to the incidence in the nation for the same year as the diagnosis was confirmed for the individual case. Regarding seasonal variation, a Poisson regression model was used to see if the difference in the number of cases for each month was significant, observing both by months and by clustering into the four seasons, winter (December, January, February), spring (March, April, May), summer (June, July, August) and autumn (September, October, November).
Results
Annual incidence
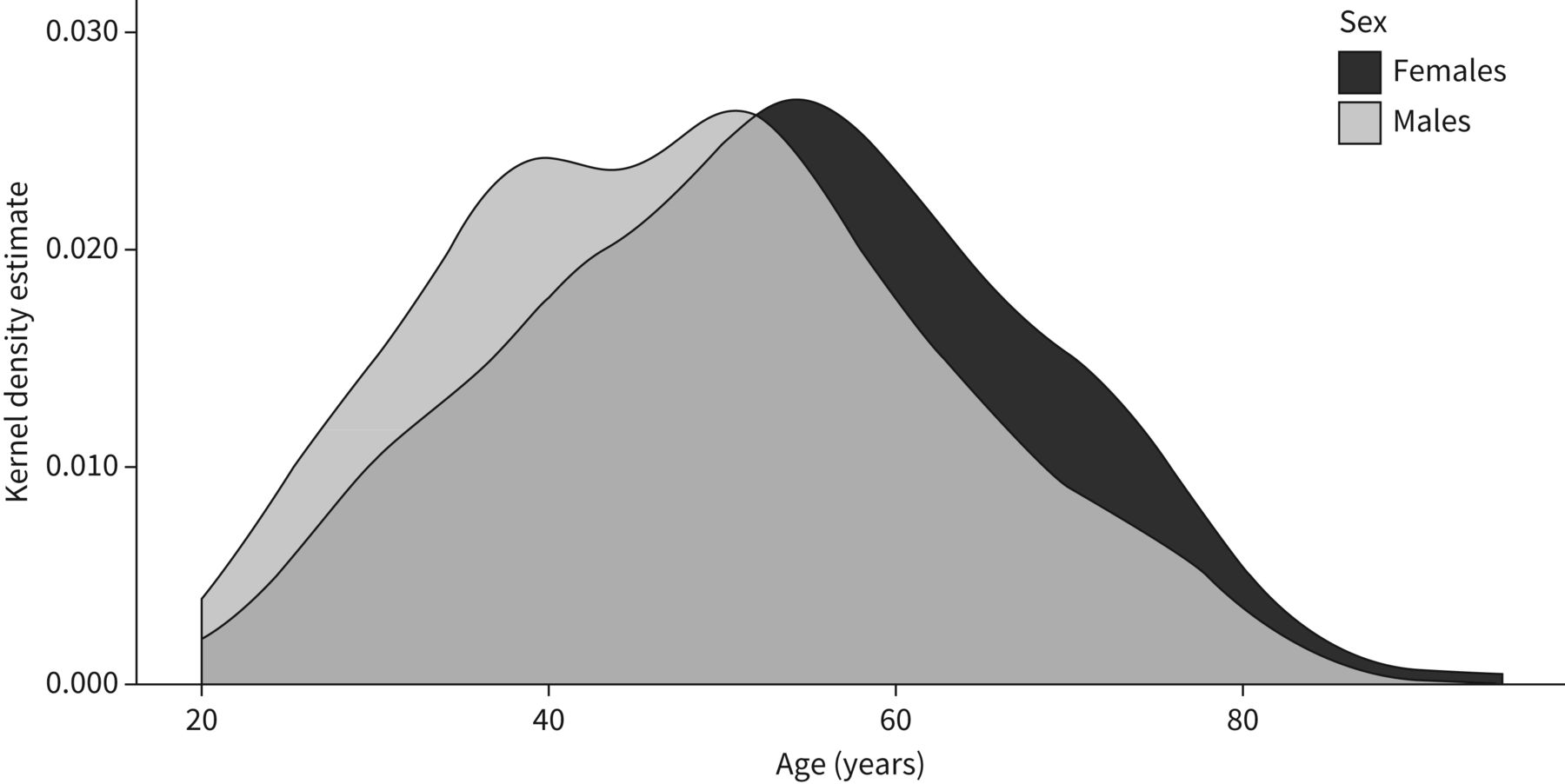
We identified 418 histologically verified cases of sarcoidosis (54% female). The mean±sd age at diagnosis was 50.8±14 years. Females were diagnosed at an older age (53.0±14.2 years versus 48.2±13.8 years; p<0.0001) (figure 1). Smoking history, self-reported pollution at work, household animals marital status, and living area are presented in table 1.

The density distribution for age at diagnosis for females and males. The total area under the curve is normalised to 1.0.
Demographic data on the study population
The annual incidence rate was 4.15/100 000/year (4.44/100 000 among females and 3.78/100 000 among males) (figure 2). A peak in diagnosis among females was seen during late winter and early spring (figure 3), although the difference between seasons was nonsignificant. When all cases of sarcoidosis, tissue proven or not, were considered, the total number of cases of sarcoidosis rose from 418 to 466. Thus, only 48 cases were found to have been diagnosed with sarcoidosis without a tissue biopsy for the main part of the study period.

Incidence of sarcoidosis per 100 000 Icelanders for each 5-year period from 1981 to 2016.

The number of sarcoidosis cases diagnosed for each month showing the seasonal variation.
Clinical manifestations
Information on subjective symptoms was obtained in 348 of the cases (83.2%). Respiratory symptoms (grouped) were present in most cases: 63.6% in females and 60.8% in males. Fatigue was the most common single symptom reported by both sexes, present in 49.1% of females and 50.3% of males. Subjective symptoms by sex are shown in figure 4. When examining fatigue for those diagnosed less than a year from the beginning of symptoms compared to those diagnosed over a year after first symptoms, there was no significant difference for fatigue between the groups (p=0.238).

Frequency of symptoms for females and males. Respiratory symptoms include cough, expectoration, dyspnoea and chest pain.
Smoking and other environmental factors
Smoking history was obtained from 322 individuals (77.0%). There was no significant difference between smoking habits and being diagnosed with sarcoidosis (figure 5). Suspected hazardous exposure in the workplace was reported by 19.4% of the cases, more often by males than females (69.5% versus 36.4%, p<0.0001), and was of various types: hay, mould, silica, asbestos and epoxy from painting/varnish. Only two cases reported exposure to insecticides.

Boxplot of observed incidence rates for smoking habits according to sex. Incidence was found by comparing the study group with national data. Age groups, sex and years were adjusted for.
Occupation
Occupational history was registered in 282 (67.5%) cases. For females, the highest incidence of sarcoidosis was found among plant and machine operators and assemblers. For males, the same applied for office workers. Occupation by sex is shown in figure 6 in relation to national data.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidence for each employment sector, where the dotted line shows the mean incidence rate for sarcoidosis in Iceland.
Spirometry and laboratory findings
Pulmonary function data were available for 241 (57.7%) of the study group. DLCO was under the normal range in 54.0% of the females and 32.1% of the males (p<0.05). FEV1 was under the normal range in 27.8% of the females and 25.0% of the males. FVC values were more often under the normal range in females than males—24.8% compared to 22.4%. ECG was described as abnormal in 19 males and 17 females but was only obtained in 39% of cases. The abnormalities described were extra-systoles, left anterior bundle branch block, bradycardia and other nonspecific abnormalities. Only one case in this dataset was suspected of cardiac sarcoidosis. Hypercalcaemia was present in 23.9% of the female cases and 20.0% of the males who had their calcium measured, which was only done in 29% of the whole group. ACE was measured in 36 cases, five of whom had elevated ACE levels.
Scadding stages
About one third or 32.2% of the chest radiographs were interpreted as indicating Scadding Stage I. Only two cases, both females (0.7%), were staged as Scadding Stage IV. The results of the Scadding stages, according to sex, are shown in table 2. No differences were observed in the spreading of the Scadding stages between sexes (p=0.3386).
Staging of sarcoidosis according to chest radiograph abnormalities (Scadding staging)
Tissue samples and treatment
Lung and/or transbronchial biopsies obtained tissue samples in 184 cases (98 females and 86 males, 44% in total), mediastinoscopy in 103 cases (51 females, 52 males, 24.6% of total cases) and surgical biopsy in 49 cases (24 females and 25 males, 11.7%). Among other biopsies were fine needle biopsies from the skin, peripheral lymph nodes or other organs. One case was diagnosed post mortem by autopsy. Information on treatment was obtained for 347 individuals or 83% of the cases. Most often (72.6% of cases) oral corticosteroids were used, followed by methotrexate (24.8%). Only eight patients (2.8%) received treatment with infliximab in the observed period.
Discussion
The present study shows a lower incidence of sarcoidosis in Iceland than in other Western countries. Those studies used different inclusion criteria [1, 7, 13]. On the other hand, the incidence of sarcoidosis in our study is higher than in a Japanese study where the same inclusion criteria were used [15]. Incidence was stable until the mid-1990s; then it increased but has been declining since 2010. Part of the explanation for this could be that after 1995 a better knowledge of the disease and the diagnostic approach reduces the need for tissue samples for confirming the diagnosis of sarcoidosis. However, the decline in annual incidence in recent years could also be caused by increased awareness of possible hazardous environmental factors. A few cases were identified without a positive tissue biopsy. The data on this were not available for the whole study period, but all the same, show that this disease is mainly diagnosed with a pathological verification in Iceland.
To our knowledge, only two epidemiological studies included exclusively tissue-verified cases of sarcoidosis [15, 16] aside from a large international multicentre study on phenotypes in sarcoidosis, where 90% of the cases were tissue-verified [20]. In most other studies, inclusion was based on clinical and chest radiograph findings [6]. This must be kept in mind when our results are compared to other studies.
Females did not show the biphasic age distribution at diagnosis seen elsewhere and were older than males at the time of diagnosis [7, 15]. However, our male patients did show this biphasic age pattern, which is in concordance with other studies [20, 36]. We also observed a trend to seasonal clustering of incidences in late winter and early spring, also seen in other studies, although not significant [43, 44].
Fatigue was the single most frequent symptom: it was reported by half of our patients and by both sexes. This is in accordance with studies from Estonia and the Netherlands [19, 36], whereas fatigue was rarely reported in Japan [15]. In our study, the prevalence of fatigue was independent of the diagnosis delay. However, when grouped, respiratory symptoms were the most common manifestation of sarcoidosis in Iceland, which is consonant with other studies among Caucasians [20, 36]. In our study, uveitis or iritis were the most common eye manifestations, as reported by others [2]. Skin lesions (other than erythema nodosum) were more frequently reported in our study than in Japan and Europe, however, consistent with many other studies [15, 20, 22, 51]. Arthritis and/or arthralgia were common complaints, as we have reported earlier [52]. Our finding is also in accordance with other studies regarding the rare involvement of the central nervous system and heart [15, 22, 51]. The difference in the clinical picture shown in Iceland and Japan is interesting and indicates an ethnic variability in sarcoidosis; there is also a difference in non-Caucasians and the Icelandic sarcoidosis population.
In the present study, nonsmokers or previous smokers outnumbered current smokers even though the difference was nonsignificant. This is not in concordance with most previous studies, which show a negative correlation between smoking and sarcoidosis [2, 4, 20, 41, 42, 53]. Our findings of the high incidence of sarcoidosis among male office workers (relative risk 18.9 for males and 8.4 for females) and female machine operators and assemblers (relative risk 9.7 for females and 6.8 for males) must be taken with caution, because hospital charts do not use ISTARF95 classification for registration of work, so the subjects were classified afterwards according to the available data in the hospital charts. This might skew the results when compared to national data. Therefore, it would not be advisable to link the causality of male office workers or a female machine operator with a higher risk of sarcoidosis, although there is an indication of that.
Spirometry results indicate that more females than males have a defect in diffusion capacity, as represented by a DLCO <80% predicted. Females may develop pulmonary hypertension more often due to parenchymal disease in sarcoidosis, but we do not have any data supporting this in our study. Interestingly, pulmonary hypertension has been reported in up to 47% of sarcoidosis patients with exertional dyspnoea, which is disproportionate to pulmonary function tests [54]. Another explanation could be that females are more prone to developing interstitial changes than males, as a recent study showed a significant increase in DLCO after 1 month of steroid treatment for sarcoidosis [55]. The distribution of Scadding staging was as seen in other studies, with stages I and II being most frequent [14, 15, 20, 36], and it may represent a relatively mild disease.
The main strength of this study is that it is nationwide in an ethnically homogenous population; diagnoses were according to the gold standard (i.e., tissue-verified) and based on reliable registers. Landspitali, University Hospital of Iceland, is a tertiary hospital serving the whole country with pulmonary services, and most cases were referred there for diagnosis and treatment.
It could be argued that our choice only to include in our study individuals with tissue-verified sarcoidosis, not clinically and/or radiograph diagnosed, is a limitation. We found a part of those described before in this paper, and they constituted an 11.4% increase in the total number of cases over these 36 years. This small number has, in our opinion, little effect on the main results. It is true that by excluding those without tissue biopsy, we most likely missed those with Lofgren's syndrome. The cases diagnosed by a skin biopsy by one dermatologist in Iceland are believed to be very few, and we assume that those cases had few or no systemic manifestations. Therefore, we conclude that those missed, clinically diagnosed or diagnosed with a skin biopsy by this one dermatologist would have had a minimal effect on the outcome of our study.
We are aware that a weakness of this retrospective study is that it was based on hospital charts, so the information is limited to what was registered in each chart. Sometimes this results in a lack of information on topics important for the clinical picture of sarcoidosis.
In conclusion, the incidence of sarcoidosis in Iceland is low compared to other western countries but higher than in a Japanese population. Fatigue is a predominant clinical symptom. Critical illnesses caused by sarcoidosis with end-stage organ involvement or the requirement for intensive treatment, such as with biologics, appear to be rare in Iceland. The incidence of sarcoidosis continued to rise at the beginning of the study period but has declined in recent years. The decline in recent years could reflect better awareness of occupational safety and less exposure to possible environmental factors.
Acknowledgements
The authors would like to thank Kristjan A. Kristjansson for creating the database for the study group. The authors also thank Kari Eiriksson at Intellecon for his work on statistical analyses. We would also like to acknowledge Lovisa Gudmundsdottir for her help with collecting data.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: S.Ó. Haraldsdóttir reports support for the present manuscript from The Science Fund of Landspitali, University Hospital of Iceland, and The Icelandic Respiratory Society.
Conflict of interest: J.G. Jonasson has nothing to disclose.
Conflict of interest: K.B. Jorundsdottir has nothing to disclose.
Conflict of interest: H.J. Hannesson reports support for the present manuscript from The Science Fund of Landspitali, University Hospital of Iceland.
Conflict of interest: T. Gislason has nothing to disclose.
Conflict of interest: B. Gudbjornsson reports consulting fees from Novartis, and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Amgen and Novartis, outside the submitted work.
Support statement: The Icelandic Bioethics Committee (VSN 99-069-V1-V2-S1) and the Icelandic Data Protection Authority (99080306) approved the study protocol. It was supported by grants from The Science Fund of Landspitali, University Hospital of Iceland, and from the Association of Icelandic Pulmonologists.
- Received June 16, 2021.
- Accepted September 22, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










