





Figures
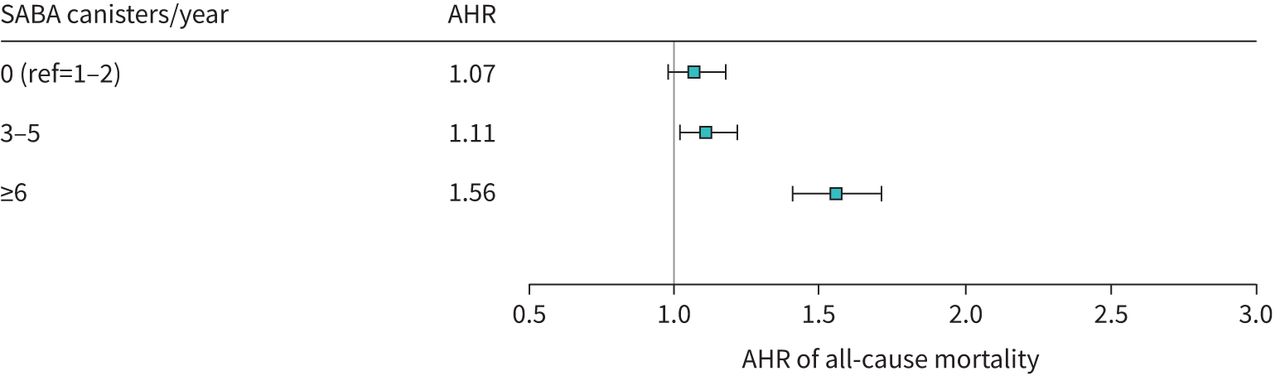
- FIGURE 1
Forest plot comparing adjusted hazard ratios (AHRs) for all-cause mortality from Cox proportional hazards regression. The Cox proportional hazards regression models were adjusted for the following: age, sex, prevalence of comorbidities, prevalence of asthma exacerbation at baseline as an indicator of severity of asthma, Ontario Marginalization Index (deprivation and dependency), rurality and asthma medication use at baseline. SABA: short-acting β2-agonist; ref: reference.
- FIGURE 2
Forest plot comparing adjusted hazard ratios (AHRs) for severe asthma exacerbations from Cox proportional hazards regression. The Cox proportional hazards regression models were adjusted for the following: age, sex, prevalence of comorbidities, prevalence of asthma exacerbation at baseline as an indicator of severity of asthma, Ontario Marginalization Index (deprivation and dependency), rurality and asthma medication use at baseline. SABA: short-acting β2-agonist; ref: reference.

{kind=link}
{kind=link}
Tables
- TABLE 1
Characteristics of the study population and baseline medication use by number of short-acting β2-agonist (SABA) canisters (n=59 533)
Covariates Number of SABA canisters Total p-value# 0 1–2 3–5 ≥6 Subjects n 33 332 17 736 5332 3133 59 533 Participant factors Sex n (%) Female 21 898 (65.7) 12 561 (70.8) 3645 (68.4) 1982 (63.3) 40 086 (67.3) <0.001 Male 11 434 (34.3) 5175 (29.2) 1687 (31.6) 1151 (36.7) 19 447 (32.7) Age at index date years Mean±sd 69.80±6.12 69.55±5.82 69.38±6.08 69.35±6.26 69.67±6.04 <0.001 Median (IQR) 67.00 (65.00–73.00) 67.00 (65.00–72.00) 66.00 (65.00–72.00) 66.00 (65.00–72.00) 67.00 (65.00–72.00) <0.001 Age group at index
date years, n (%)65–69 21 254 (63.8) 11 551 (65.1) 3536 (66.3) 2080 (66.4) 38 421 (64.5) <0.001 70–74 5533 (16.6) 3044 (17.2) 841 (15.8) 476 (15.2) 9894 (16.6) 75–79 3415 (10.2) 1727 (9.7) 498 (9.3) 300 (9.6) 5940 (10.0) 80–89 3130 (9.4) 1414 (8.0) 457 (8.6) 277 (8.8) 5278 (8.9) Age at asthma
prevalence
yearsMean±sd 59.73±9.74 59.40±9.59 59.98±10.47 59.62±10.85 59.64±9.83 <0.001 Median (IQR) 59.00 (52.00–66.00) 59.00 (52.00–66.00) 60.00 (51.00–67.00) 59.00 (50.00–67.00) 59.00 (52.00–66.00) 0.004 Years of asthma at index
dateMean±sd 10.03±6.61 10.12±6.85 9.32±7.07 9.60±7.09 9.97±6.76 <0.001 Median (IQR) 10.63 (4.14–15.16) 10.68 (3.65–15.53) 9.78 (1.72–14.99) 10.19 (2.25–14.95) 10.57 (3.68–15.23) <0.001 Baseline asthma medication use, n (%) No asthma medication 20 672 (62.0) 0 (0.0) 0 (0.0) 0 (0.0) 20 672 (34.7) <0.001 ICS only or ICS-LABA 11 653 (35.0) 3988 (22.5) 1742 (32.7) 1134 (36.2) 18 517 (31.1) SABA only 0 (0.0) 6292 (35.5) 1100 (20.6) 491 (15.7) 7883 (13.2) Other asthma
medication1007 (3.0) 7456 (42.0) 2490 (46.7) 1508 (48.1) 12 461 (20.9) Socio-demographic factors Neighbourhood income
quintile, n (%)1 (lowest) 5639 (16.9) 2972 (16.8) 1051 (19.7) 704 (22.5) 10 366 (17.4) <0.001 2 6648 (19.9) 3562 (20.1) 1133 (21.2) 726 (23.2) 12 069 (20.3) 3 6445 (19.3) 3563 (20.1) 1073 (20.1) 642 (20.5) 11 723 (19.7) 4 6911 (20.7) 3763 (21.2) 1048 (19.7) 522 (16.7) 12 244 (20.6) 5 (highest) 7604 (22.8) 3843 (21.7) 1010 (18.9) 527 (16.8) 12 984 (21.8) Missing 85 (0.3) 33 (0.2) 17 (0.3) 12 (0.4) 147 (0.2) Ontario Marginalization Indices (lowest quintile is the least marginalised) Deprivation quintile,
n (%)1 (least) 6953 (20.9) 3735 (21.1) 1000 (18.8) 516 (16.5) 12 204 (20.5) <0.001 2 6752 (20.3) 3517 (19.8) 978 (18.3) 505 (16.1) 11 752 (19.7) 3 6606 (19.8) 3506 (19.8) 989 (18.5) 616 (19.7) 11 717 (19.7) 4 6652 (20.0) 3532 (19.9) 1190 (22.3) 710 (22.7) 12 084 (20.3) 5 (most) 6185 (18.6) 3354 (18.9) 1135 (21.3) 766 (24.4) 11 440 (19.2) Missing 184 (0.6) 92 (0.5) 40 (0.8) 20 (0.6) 336 (0.6) Dependency quintile,
n (%)1 (least) 5449 (16.3) 3186 (18.0) 1044 (19.6) 678 (21.6) 10 357 (17.4) <0.001 2 5981 (17.9) 3322 (18.7) 1040 (19.5) 620 (19.8) 10 963 (18.4) 3 6142 (18.4) 3236 (18.2) 971 (18.2) 611 (19.5) 10 960 (18.4) 4 6528 (19.6) 3326 (18.8) 937 (17.6) 512 (16.3) 11 303 (19.0) 5 (most) 9048 (27.1) 4574 (25.8) 1300 (24.4) 692 (22.1) 15 614 (26.2) Missing 184 (0.6) 92 (0.5) 40 (0.8) 20 (0.6) 336 (0.6) Ethnic concentration
quintile, n (%)1 (least) 5161 (15.5) 2846 (16.0) 830 (15.6) 461 (14.7) 9298 (15.6) <0.001 2 5325 (16.0) 2928 (16.5) 856 (16.1) 418 (13.3) 9527 (16.0) 3 6005 (18.0) 3135 (17.7) 848 (15.9) 455 (14.5) 10 443 (17.5) 4 7207 (21.6) 3567 (20.1) 960 (18.0) 560 (17.9) 12 294 (20.7) 5 (most) 9450 (28.4) 5168 (29.1) 1798 (33.7) 1219 (38.9) 17 635 (29.6) Missing 184 (0.6) 92 (0.5) 40 (0.8) 20 (0.6) 336 (0.6) Instability quintile, n (%) 1 (least) 6470 (19.4) 3689 (20.8) 1129 (21.2) 712 (22.7) 12 000 (20.2) <0.001 2 6539 (19.6) 3512 (19.8) 949 (17.8) 516 (16.5) 11 516 (19.3) 3 6224 (18.7) 3264 (18.4) 975 (18.3) 560 (17.9) 11 023 (18.5) 4 6045 (18.1) 3188 (18.0) 1017 (19.1) 535 (17.1) 10 785 (18.1) 5 (most) 7870 (23.6) 3991 (22.5) 1222 (22.9) 790 (25.2) 13 873 (23.3) Missing 184 (0.6) 92 (0.5) 40 (0.8) 20 (0.6) 336 (0.6) Rural residence, n (%) 3046 (9.1) 1738 (9.8) 545 (10.2) 307 (9.8) 5636 (9.5) 0.015 Follow-up years Mean±sd 8.82±3.25 8.82±3.17 9.07±3.35 9.01±3.58 8.85±3.25 <0.001 Median (IQR) 8.50 (6.41–11.59) 8.47 (6.41–11.55) 8.75 (6.65–12.17) 8.81 (6.56–12.34) 8.53 (6.43–11.66) <0.001 Number of comorbidities,
n (%)0 7732 (23.2) 4029 (22.7) 1206 (22.6) 626 (20.0) 13 593 (22.8) 0.001 1 12 762 (38.3) 6940 (39.1) 2053 (38.5) 1240 (39.6) 22 995 (38.6) 2 8260 (24.8) 4407 (24.8) 1396 (26.2) 831 (26.5) 14 894 (25.0) ≥3 4578 (13.7) 2360 (13.3) 677 (12.7) 436 (13.9) 8051 (13.5) Outcomes Deaths, n (%) 4487 (13.5) 1942 (10.9) 703 (13.2) 552 (17.6) 7684 (12.9) <0.001 Severe asthma
exacerbation, n (%)446 (1.3) 642 (3.6) 343 (6.4) 295 (9.4) 1726 (2.9) <0.001 SABA: short-acting β2-agonist; IQR: interquartile range; ICS: inhaled corticosteroid; ICS-LABA: ICS long-acting β2-agonist. #: p-values were calculated using Chi-squared statistics for categorical variables and ANOVA for numerical variables.
- TABLE 2
All-cause mortality hazard ratios (HRs) from Cox proportional hazard regressions (n=59 533)
Unadjusted HR
(95% CI)p-value AHR
(95% CI)p-value Exposure SABA canisters per year 0 1.23 (1.16–1.29) <0.0001 1.07 (0.98–1.17) 0.15 1–2 1.00 (Reference) 1.00 (Reference) 3–5 1.14 (1.05–1.25) 0.00 1.11 (1.02–1.22) 0.02 ≥6 1.52 (1.38–1.67) <0.0001 1.56 (1.41–1.71) <0.0001 Covariate Deprivation quintile 1 (least) 1.00 (Reference) 1.00 (Reference) 2 1.09 (1.01–1.17) 0.02 1.03 (0.95–1.11) 0.47 3 1.12 (1.04–1.21) 0.00 1.00 (0.93–1.08) 0.97 4 1.21 (1.13–1.3) <0.0001 1.03 (0.96–1.11) 0.44 5 (most) 1.33 (1.23–1.42) <0.0001 1.11 (1.04–1.19) 0.00 Dependency quintile 1 (least) 1.00 (Reference) 1.00 (Reference) 2 1.10 (1.01–1.20) 0.02 1.03 (0.95–1.12) 0.52 3 1.15 (1.06–1.25) 0.00 1.08 (0.99–1.17) 0.07 4 1.30 (1.20–1.41) <0.0001 1.16 (1.07–1.26) 0.00 5 (most) 1.67 (1.56–1.8) <0.0001 1.25 (1.16–1.34) <0.0001 Age group at index date 1.17 (1.16–1.17) <0.0001 1.16 (1.16–1.17) <0.0001 Male sex (reference=female) 1.09 (1.04–1.14) 0.00 1.30 (1.24–1.36) <0.0001 Rural residence
(reference=urban)1.05 (0.97–1.13) 0.24 1.19 (1.10–1.28) <0.0001 ICS only or ICS-LABA 1.00 (Reference) 1.00 (Reference) No asthma medication 1.43 (1.35–1.51) <0.0001 1.26 (1.18–1.34) <0.0001 SABA only 1.29 (1.20–1.39) <0.0001 1.19 (1.08–1.31) 0.00 Other asthma medication 1.26 (1.19–1.35) <0.0001 1.16 (1.07–1.26) 0.00 Asthma exacerbation in
baseline period0.90 (0.69–1.16) 0.40 1.08 (0.83–1.39) 0.58 Number of comorbidities 0 1.00 (Reference) 1.00 (Reference) 1 1.63 (1.51–1.76) <0.0001 1.25 (1.15–1.34) <0.0001 2 2.54 (2.36–2.75) <0.0001 1.66 (1.54–1.79) <0.0001 ≥3 3.75 (3.46–4.06) <0.0001 2.13 (1.96–2.31) <0.0001 AHR: adjusted hazard ratio; SABA: short-acting β2-agonist; ICS: inhaled corticosteroid; ICS-LABA: ICS long-acting β2-agonist.
- TABLE 3
Severe asthma exacerbation hazard ratios (HRs) from Cox proportional hazard regressions (n=59 533)
Unadjusted HR
(95% CI)p-value AHR
(95% CI)p-value Exposure SABA canisters per year 0 0.38 (0.34–0.43) <0.0001 0.64 (0.56–0.75) <0.0001 1–2 1.00 (Reference) 1.00 (Reference) 3–5 1.73 (1.52–1.97) <0.0001 1.59 (1.4–1.82) <0.0001 ≥6 2.50 (2.17–2.87) <0.0001 2.26 (1.96–2.60) <0.0001 Covariate Deprivation quintile 1 (least) 1.00 (Reference) 1.00 (Reference) 2 1.07 (0.91–1.25) 0.4335 1.05 (0.89–1.23) 0.5702 3 1.21 (1.03–1.41) 0.0185 1.14 (0.97–1.33) 0.1055 4 1.32 (1.14–1.54) 0.0003 1.23 (1.05–1.43) 0.0089 5 (most) 1.51 (1.30–1.76) <0.0001 1.42 (1.22–1.65) <0.0001 Dependency quintile 1 (least) 1.00 (Reference) 1.00 (Reference) 2 0.82 (0.70–0.96) 0.0135 0.84 (0.71–0.98) 0.0305 3 0.99 (0.85–1.15) 0.8407 1.01 (0.87–1.18) 0.911 4 0.93 (0.8–1.09) 0.3596 0.95 (0.82–1.12) 0.558 5 (most) 0.89 (0.77–1.02) 0.0958 0.90 (0.78–1.05) 0.179 Age group at index date 0.98 (0.97–0.99) <0.0001 0.98 (0.97–0.99) <0.0001 Male sex (reference=female) 0.67 (0.60–0.75) <0.0001 0.69 (0.62–0.77) <0.0001 Rural residence
(reference=urban)1.67 (1.47–1.91) <0.0001 1.73 (1.51–1.98) <0.0001 Number of comorbidities 0 1.00 (Reference) 1.00 (Reference) 1 1.01 (0.89–1.14) 0.8902 0.98 (0.86–1.11) 0.7211 2 1.05 (0.91–1.20) 0.5219 1.03 (0.90–1.19) 0.637 ≥3 0.91 (0.77–1.07) 0.2566 0.97 (0.82–1.15) 0.7115 AHR: adjusted hazard ratio; SABA: short-acting β2-agonist.
- TABLE 4
Summary of findings from other published studies
Country Authors [ref.] Published year Journal Year of data Study population Study size Findings SABA overuse prevalence (%) All-cause mortality# Asthma exacerbation# France Raherison-Semjen et al. [21] 2018 Eur Respir J 2018 Aged ≥18 years with an asthma diagnosis n=15 587 28.30 Not reported Not reported Poland Kupczyk et al. [22] 2019 Eur Respir J 2018 Aged 18–64 years with an asthma diagnosis n=91 673 29–37 Not reported Not reported Germany Worth et al. [19] 2021 Respir Res 2017–2018 Aged ≥12 years with an asthma diagnosis in the Disease Analyser database (IQVIA) n=15 640 36 Not reported Not reported UK Bloom et al. [9] 2020 Adv Ther 2007–2017 Aged ≥12 years with an asthma diagnosis n=574 913 38 Not available (due to small numbers) 1–2 canisters: 1.20 (1.16–1.24)
3–5 canisters:
1.24 (1.20–1.28)Italy Di Marco et al. [8] 2021 Adv Ther 2015–2018 Aged ≥12 years with an asthma diagnosis n=22 102 9 Not reported Compared to <3 canisters/year:
≥3 canisters:
1.27 (1.21–1.33)Sweden Nwaru et al. [7] 2020 Eur Respir J 2006–2016 Aged 12–45 years in the nationwide longitudinal cohort, those who collected medication for COPD n=365 324 30 Compared to <3 canisters/year:
3–5 canisters:
1.26 (1.14–1.39)
6–10 canisters
1.67 (1.49–1.87)
≥11 canisters:
2.35 (2.02–2.72)Compared to <3 canisters/year:
3–5 canisters:
1.26 (1.24–1.28)
6–10 canisters:
1.44 (1.41–1.46)
≥11 canisters:
1.77 (1.72–1.83)Taiwan Wang et al. [23] 2021 NPJ Prim Care Resp Med 2001–2015 Aged 12–100 years with asthma who enrolled in the Taiwanese pay-for-performance asthma programme n=218 039 16 Compared to no ICS and <3 canisters/year:
3–6 canisters:
1.17 (1.09–1.25)
≥7 canisters:
2.01 (1.89–2.13)Compared to no ICS and <3 canisters/year:
3–6 canisters:
2.43 (2.36–2.50)
≥7 canisters:
4.94 (4.79–5.09)Canada To et al.
(current study)2022 ERJ Open Res 2006–2020 Aged 65–99 years with prevalent asthma in the OASIS n=59 533 14 Compared to 1–2 canisters/year:
3–5 canisters:
1.11 (1.02–1.22)
≥6 canisters:
1.56 (1.41–1.71)Compared to 1–2 canisters/year:
3–5 canisters:
1.59 (1.40–1.82)
≥6 canisters:
2.26 (1.96–2.60)SABA: short-term β2-agonist; ICS: inhaled corticosteroid; OASIS: Ontario Asthma Surveillance System. #: all-cause mortality and asthma exacerbation data presented as hazard ratio (95% CI).
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00032-2022.SUPPLEMENT










