





Abstract
Despite the enormous impact on human health, acute respiratory distress syndrome (ARDS) is poorly defined, and its timely diagnosis is difficult, as is tracking the course of the syndrome. The objective of this pilot study was to explore the utility of breath collection and analysis methodologies to detect ARDS through changes in the volatile organic compound (VOC) profiles present in breath. Five male Yorkshire mix swine were studied and ARDS was induced using both direct and indirect lung injury. An automated portable gas chromatography device developed in-house was used for point of care breath analysis and to monitor swine breath hourly, starting from initiation of the experiment until the development of ARDS, which was adjudicated based on the Berlin criteria at the breath sampling points and confirmed by lung biopsy at the end of the experiment. A total of 67 breath samples (chromatograms) were collected and analysed. Through machine learning, principal component analysis and linear discrimination analysis, seven VOC biomarkers were identified that distinguished ARDS. These represent seven of the nine biomarkers found in our breath analysis study of human ARDS, corroborating our findings. We also demonstrated that breath analysis detects changes 1–6 h earlier than the clinical adjudication based on the Berlin criteria. The findings provide proof of concept that breath analysis can be used to identify early changes associated with ARDS pathogenesis in swine. Its clinical application could provide intensive care clinicians with a noninvasive diagnostic tool for early detection and continuous monitoring of ARDS.
Abstract
ARDS, confirmed by lung biopsy, was induced in swine, with breath monitored hourly. Seven VOC markers distinguish ARDS, which are the same as those in human ARDS and can predict ARDS onset ∼3 h earlier than clinical adjudication. https://bit.ly/3zIIIMQ
Introduction
For the past 50 years acute respiratory distress syndrome (ARDS) has continued to be a significant public health threat, with an annual incidence rate of >200 000 cases in the USA and an annual global rate of 13.5 cases per 100 000 population [1]. Early detection and trajectory monitoring of ARDS is critical to its treatment [2–5]. Despite the enormous impact on human health, ARDS remains poorly defined, and little progress has been made in advancing novel diagnostic and prognostic tools.
The most common ARDS risk model is the lung injury prediction score (LIPS), but it has a low ability to predict disease onset [6, 7]. The clinical diagnosis based on the Berlin criteria shows a moderate correlation with real-time and post mortem tissue pathological findings [8–10], but does not account for the critical, dynamic inflammatory processes that participate in ARDS. Furthermore, there are currently no predictive clinical biomarkers of ARDS pathogenesis. This hinders the ability of clinicians to detect the early or preclinical onset of ARDS.
Breath contains hundreds of volatile organic compounds (VOCs), some of which may provide information about the inflammatory state of the lungs as ARDS develops and progresses. Therefore, breath analysis can potentially be very useful for noninvasive ARDS detection and continuous monitoring [2, 3, 11–14]. In a previous study, we predicted ARDS in human subjects with high accuracy when compared to clinical adjudication based on Berlin criteria [13]. The study was limited by the absence of confirmatory, histopathologic evidence of ARDS (i.e. diffuse alveolar damage). Second, assessment of the rate of change in specific breath compounds (e.g. trajectory monitoring), which may be vital for timely clinical and therapeutic decision-making, was limited.
In our present work, we overcame the aforementioned limitations by using a newly developed and optimised swine model of ARDS that accurately replicates human conditions [15]. Animal models, particularly large animals such as swine, have been used in biomedical research for decades because of their anatomical and physiological similarities to humans [16–18]. They are also an ideal species for modelling the inflammatory response to ARDS [19, 20]. An automated portable gas chromatograph (GC) developed in-house was employed to study swine breath to better understand the pathophysiology and the utility of breath analytes as predictors of ARDS. Each swine was monitored hourly, starting from initiation of the experiment until the development of clinically defined ARDS. This approach provided us the opportunity to monitor VOCs during the development of ARDS, as well as dynamic changes that may be associated with it. Lung pathology was assessed at the end of the experiment to confirm the presence of diffuse alveolar damage.
Materials and methods
Animal preparation and induction of lung injury
We used a recently described swine model of ARDS that uses clinically relevant exposures (sepsis, hyperoxia, volutrauma and aspiration) and faithfully replicates the physiological, radiographical and histopathological features of ARDS [15]. As reported recently, this model fulfils both clinical criteria (Berlin definition) [9] and experimental criteria for animal models of ARDS [21].
Five male Yorkshire mix swine weighing 45 (±2) kg were used in the study. The Institutional Animal Care and Use Committee (IACUC) at the University of Michigan approved the study. All procedures were carried out in compliance with the university's institutional standards for care and use of laboratory animals in accordance with National Institutes of Health (NIH) guidelines [22]. Detailed physiological data regarding these animals have previously been published [15].
Animals were fasted overnight with libitum access to water and on the day of the experiment, anaesthesia was induced. Animals were intubated and mechanically ventilated to maintain a baseline end-tidal CO2 level between 35 and 45 mmHg (Biopac Systems Inc., Goleta, CA, USA). At the end of surgical instrumentation, animals were transitioned to total intravenous anaesthesia using a combination of propofol, fentanyl and midazolam. The anaesthesia level was monitored for the experiment's duration by assessing corneal reflex, jaw tension and haemodynamics, including blood pressure, heart rate and respiratory rate. More details on animal preparation can be found in the studies by Tiba and co-workers [15, 23].
Animals were subjected to systemic infection via an injection of Escherichia coli into the kidney parenchyma (3.5×1011 CFU Strain CFT073 E. coli in a total of approximately 5 mL at a rate of 0.333 mL·min−1), as previously described [15, 23]. Lung injury was induced using a combination of volume trauma (tidal volumes of 15 mL·kg−1), hyperoxia (100% inspiratory oxygen fraction (FIO2)) and the instillation of gastric particles (1–2 mL·kg−1) into the airways via bronchoscope [24]. Following the induction of lung injury, animals were continuously monitored for up to 16 h, at which point the experiment was terminated and the animal was euthanised.
The adjudication of the time points at which ARDS was present was done using the Berlin criteria [9, 10], which uses the ratio of partial pressure of arterial oxygen (PaO2) to FIO2 and the chest radiograph assessed at regular intervals during experiments. The final determination of ARDS was confirmed by lung pathology determined by a pathologist blinded to the specifics of the induced injury. Figure S1 shows the PaO2/FIO2 ratios for all five swine animals. Radiographs and pictures of the lungs taken at the end of the experiment are shown elsewhere [15].
Exhaled breath collection and analysis
We used an automated, portable GC device to sample and analyse the breath from each swine before the induction of lung injury and every hour thereafter for up to 16 h or until the animal expired, whichever occurred earlier. The GC device was connected to the expiratory port of the ventilator tubing via a T-piece and 1-m long polytetrafluoroethylene (PTFE) tubing (0.64 cm internal diameter), as shown in figure 1. The same GC device was used for breath sampling and analysis for all five animals. For each breath measurement, the breath sample was collected into a thermal desorption tube installed in the GC device at a rate of 70 mL·min−1, and then analysis was performed. Finally, device cleaning was performed to ensure that no residues were left from the previous run. Details of the breath sampling and analysis processes are given in the supplementary material, section S2. The total assay time was 30 min, including 5 min of sample collection at 70 mL·min−1, 5 min of desorption/transfer, 10 min of separation and 10 min of cleaning.

a) Schematic of a portable gas chromatograph (GC) attached to a mechanical ventilator for breath analysis. b) Picture taken during the breath measurement, showing the connection of the portable GC to a mechanical ventilator via a sampling tube to monitor exhaled breath of a swine.
The raw chromatograms were first pre-processed for noise reduction, curve smoothing, alignment with the reference chromatogram and peak assignment. After pre-processing, the area of each peak was calculated and normalised by the entire area under the chromatogram curve [13, 25]. Through machine learning, principal component analysis (PCA) and linear discriminant analysis (LDA) [13, 17, 18], a subset of chromatographic peaks were selected as the biomarkers for the discrimination of ARDS. Details about the GC system and the algorithm used in data analysis can be found elsewhere [13, 25–27].
Traditional mass spectrometry was performed to identify the VOCs present in swine breath. The swine's breath at the experiment termination or animal death, whichever occurred first, was collected into a 3 L Tedlar bag. It was then assayed by our GC coupled to a Thermo Scientific Single Quadrupole Mass Spectrometer (ISQTM Series) and the results analysed using Chromeleon™ 7 software.
Results
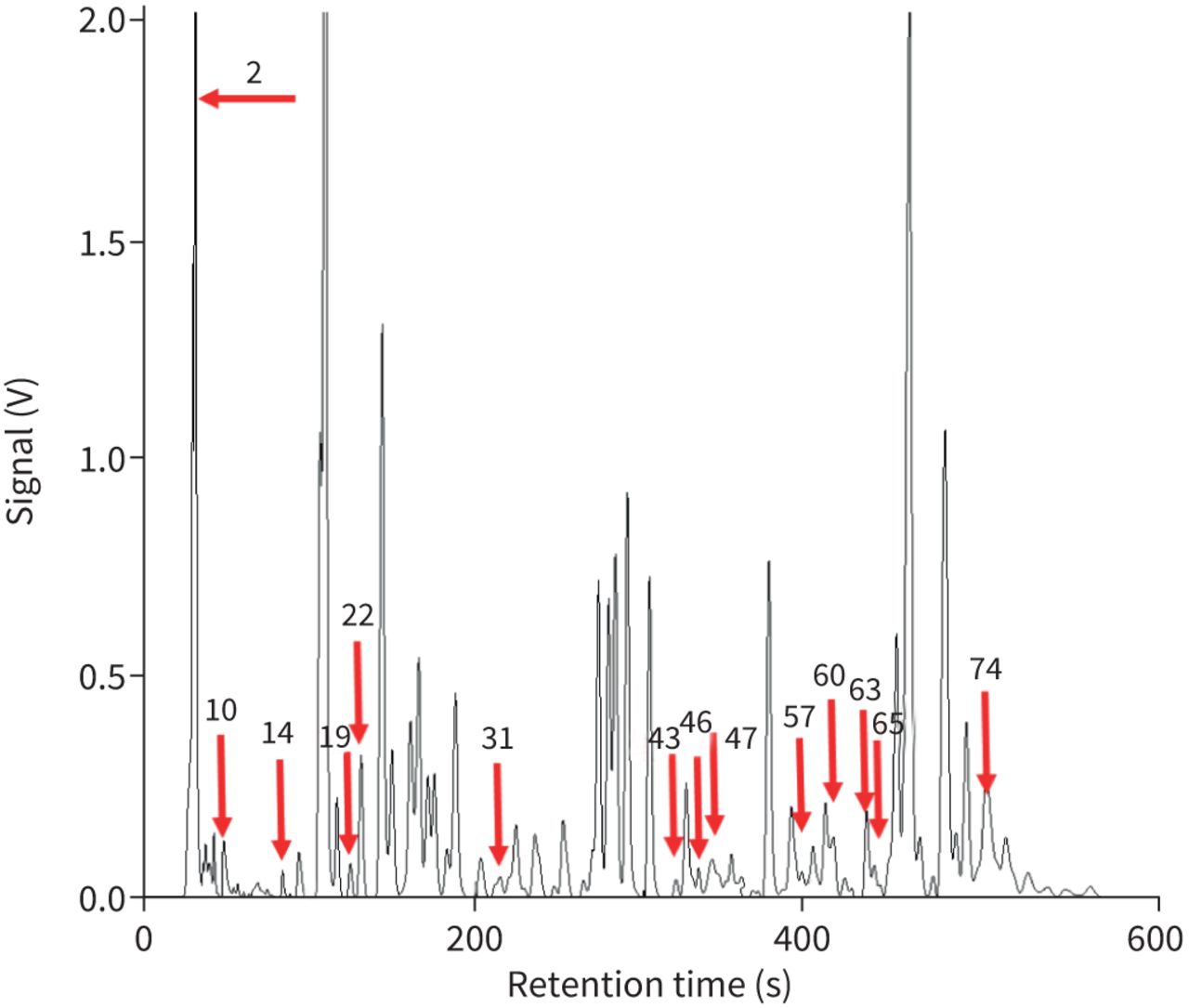
Figure 2 shows a representative chromatogram of swine breath. A total of 67 breath chromatograms from the five swine were collected and analysed, including 34 pre-ARDS chromatograms and 33 chromatograms after development of ARDS (as adjudicated by the Berlin criteria during the experiment and confirmed by lung biopsies at the end of the experiment). There were approximately 60–70 peaks in each individual chromatogram. Collectively, there were a total of 78 different peaks.
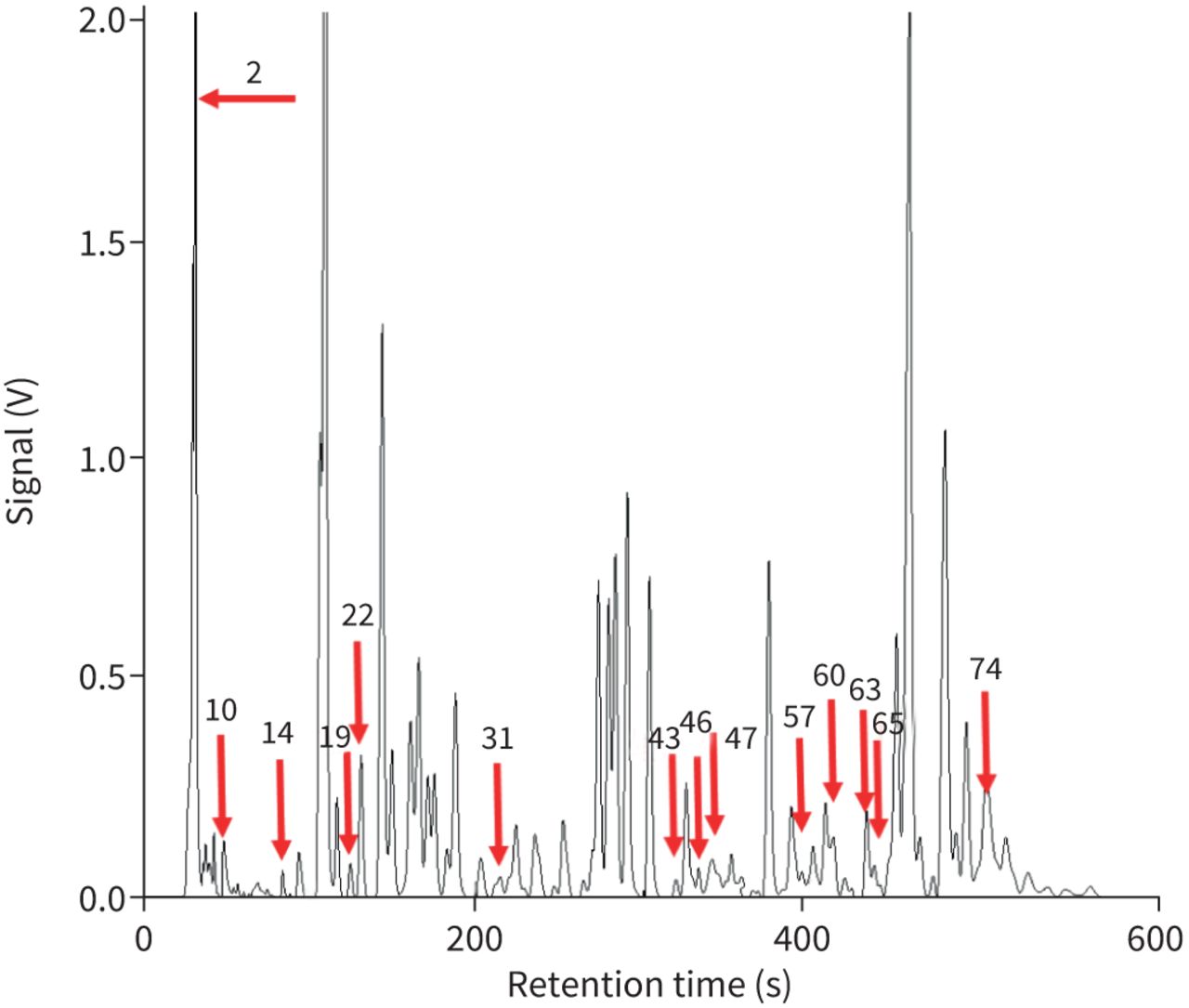
Representative gas chromatogram of exhaled breath from a swine animal via a ventilator. The red arrows show the locations of all peaks used in biomarker search (see details in table S1).
Candidate biomarkers of ARDS
For biomarker discovery, we used 40 out of 67 breath chromatograms as the training set, among which 20 were pre-ARDS and 20 were ARDS. The 20 pre-ARDS data were from the breath samples taken at the 0th hour (before lung injury was induced), and the 1st, 2nd and 3rd hour after the induction of lung injury, up until the PaO2/FIO2 ratio fell below 300. By doing this, we ensured that the swine had not developed ARDS, which was confirmed by clinical adjudication based on the Berlin criteria. The 20 ARDS chromatograms were from the breath samples taken in the last 4 h of the experiment for Swine #2, #4 and #5. Swine #1 died within 8 h and we had only the last two data points adjudicated as ARDS, which are included in the training set. For Swine #3, which died after 16 h, we used the samples taken in the last 6 h in the training set. The reason for using the samples taken 4–6 h prior to the animal's death is two-fold. First, it is highly likely that the swine had developed ARDS at this stage (4–6 h prior to death), as confirmed by clinical adjudication. Second, it was necessary to make the total number of ARDS in the training set to be 20 (i.e. equal to the number of pre-ARDS controls). The remaining 27 chromatograms (14 pre-ARDS and 13 ARDS, as adjudicated by the Berlin criteria) were used as the testing set. They were obtained between the 3rd hour after the lung injury and 4–6 h prior to death.
Through machine learning, PCA and LDA, seven VOCs (see table 1) were identified as the candidate biomarker set, which yielded a classification accuracy of 92.5% (table 2) for the training set and the largest boundary distance in the PCA plot. Interestingly, these seven analytes are the same as seven of the nine biomarkers found in our previous breath analysis, which predicted human ARDS [13]. The similarities in the biomarker set further validate our findings in humans and underscore the clinical relevancy of the swine model to simulate human conditions. We also examined the other two VOCs, 2,4-dimethylpentane and methylcyclohexane (see table 1), which differentiated human ARDS, to see whether they could be added to the current seven-analyte biomarker set. The results were neutral, i.e. adding one of them or the combination of both does not change classification accuracy. This may be due to the limited number of swine and the breath samples used in this study. In contrast, the addition of other peak(s) to the current biomarker set resulted in decreased accuracy (table S1).
Breath biomarkers that distinguish swine pre-ARDS and ARDS and/or human non-ARDS and ARDS
Corresponding statistics based on the principal component analysis scores of breath analysis for training, test and overall sets
In figure 3, we plotted the normalised peak area for each identified analyte versus time after the induction of lung injury of all five swine to assess the trend in analyte signal during the pathogenesis of ARDS. Of these, 2-methylpentane and 3-methylheptane increased over time, while the other five compounds decreased.
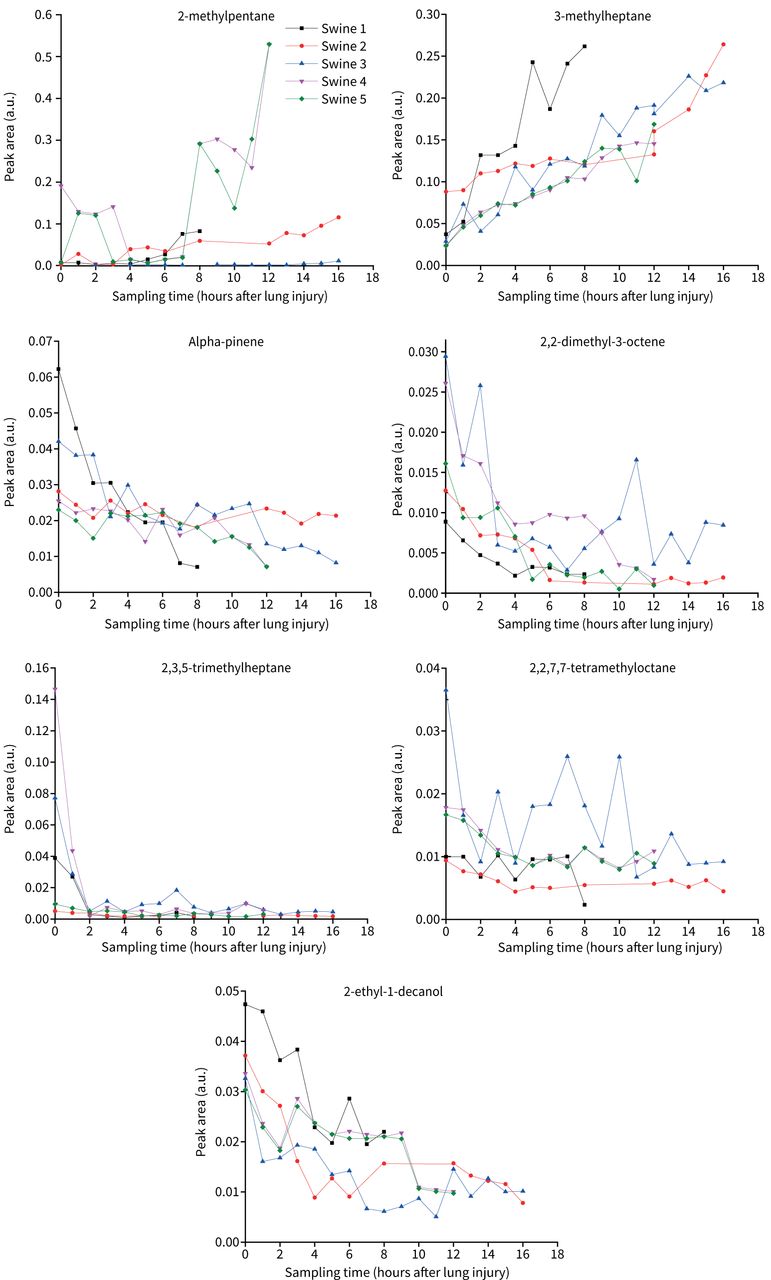
Normalised peak area versus time of seven biomarkers after the induction of lung injury. Each peak area is normalised to the total area under the chromatogram curve. The 0th hour refers to the time just before the induction of lung injury.
Figure 4 shows the PCA scores for the 40 data points in the training set using the seven discriminating analytes, giving an accuracy of 92.5%. The corresponding statistics are summarised in table 2. The data demonstrate that pre-ARDS and ARDS are well separated and that the distribution of the pre-ARDS data points is much more clustered than that for the non-ARDS human subjects in our previous study [13], perhaps indicative of the homogeneity of the swine model in comparison with the human subjects. Figures S2 and S3 show the PCA scores for the testing set and for all the datasets, respectively. The corresponding accuracy decreases significantly compared to the training set (see table 2). However, this does not necessarily indicate that breath analysis fails. Instead, it suggests the limitation of the Berlin criteria, because breath analysis can detect changes consistent with the development of ARDS approximately 3 h earlier than the clinical adjudication and all of the 27 chromatograms in the testing set were intermediate points obtained during the development of ARDS (see detailed explanation later).

Principal component analysis (PCA) plot for the training set (40 data points in total). Red circles and black crosses denote respectively acute respiratory distress syndrome (ARDS) and pre-ARDS, adjudicated using the Berlin criteria. The region below and above the boundary line represents the baseline and ARDS region, respectively, as determined by breath analysis using the seven biomarkers in table 1. The numbers shown in the PCA plot denote “swine number.sampling time”. For example: “1.2” refers to Swine #1 sampled 2 h after the induction of lung injury; “4.0” refers to Swine #4 sampled before the induction of lung injury; “4.11” refers to Swine #4 sampled 11 h after the induction of lung injury.
Cross-validation was also performed, where the original training datasets were divided into five cross-validation models. The five models yielded an overall classification accuracy of 92.5±1.5% (and 90.5±16.2% for the testing set), which indicates the robustness of the model. The statistics of the five models are presented in table S3.
Dynamic response of swine breath
The time trajectory monitoring of disease is critical for guided therapy of ARDS. In our previous study with human subjects, we did not continuously monitor subjects through their entire course so development of an ARDS trajectory was not possible. In contrast, in the current swine experiment we were able to perform a sequential hourly monitoring of the dynamic change of swine ARDS from the very beginning (prior to the induction of lung injury) to the end of the experiment (death from ARDS), as shown in figure 5 where each swine moved from pre-ARDS to ARDS. The first data point (the 0th hour, before the induction of lung injury) and the last data point (just before the death from ARDS) are well separated and far from the boundary line. For all five swine, as the experiment progresses, the PCA trajectory moves from the 0th hour (i.e. the pre-ARDS region) towards the boundary line, then reaches the ARDS region, and eventually moves farther away from the boundary line as the severity of ARDS increases. The only exception is “3.10” (Swine #3 at the 10th hour), which shows movement to a decreased state of severity. This could, however, be caused by errors in breath measurement.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Principal component analysis (PCA) plots showing hourly trajectories of individual swine starting from the 0th hour (healthy and just prior to the induction of lung injury) to the end of the experiment or until the animal died (last data point, acute respiratory distress syndrome (ARDS) confirmed by biopsy). This figure shows the dynamic change in a swine's breath when the animal status changes from healthy pre-ARDS to ARDS. Red circles and black crosses denote respectively ARDS and pre-ARDS, adjudicated based on the Berlin criteria.
Discussion
To better understand the physiology, pathophysiology and therapy for ARDS, we used a large animal model that replicates human conditions [15]. The animal model helps overcome some of the current clinical limitations and lends insight into the underlying physiology that leads to ARDS because it uses clinically relevant results leading to diffuse alveolar damage, the histopathological hallmark of ARDS. To date, most exhaled breath studies of ARDS have been limited in their scope, and most have used a single time point [4]. To our knowledge, we are the first group to use a portable GC to study a high-fidelity large animal model allowing for continuous point of care monitoring of VOCs. The presented results support our previous study based on human subjects for delineation between non-ARDS controls and ARDS patients in whom histopathological examination of lungs is not possible. We found that the seven biomarkers (from swine's breath) as shown in table 1 are shared with the nine biomarkers (from the human subjects) that could distinguish non-ARDS and ARDS. This underscores the clinical relevancy of the swine model to simulate human conditions.
The longitudinal analysis revealed that volatile metabolic changes in exhaled breath might be used to map the pathological trajectory of ARDS. In this animal model we provide evidence that it was possible to detect changes consistent with the development of ARDS 1–6 h (3 h on average) earlier than the clinical adjudication based on the Berlin criteria (table S2). This may be why accuracy in the testing set was much lower than the training set, because most of the data points in the testing set were obtained when the animals were in the transition from pre-ARDS to ARDS using the Berlin criteria as the gold standard. Also, as expected, animals have different trajectories of ARDS development. For example, it took less than 1 h for Swine #2 to develop ARDS after the induction of lung injury, whereas it took 3 h or longer for the other four animals to develop ARDS (they died in 11–16 h). It should be noted that the ability of breath analysis to provide early detection and trajectory monitoring of ARDS pathogenesis has also been demonstrated in a limited number of human subjects in our previous study (24–48 h earlier than the ARDS adjudication using the Berlin criteria) [13].
Compared to our previous work on human subjects, the present study has some strengths. 1) We were able to control many endogenous and exogenous factors in study subjects that might affect breath VOC profiles. The animals were all male of the same approximate age under the same controlled environmental and dietary conditions. The multiple clinically relevant insults used to produce ARDS were uniform and tightly controlled. The sample collection and analysis were the same for all animals. 2) Lung tissue biopsies were collected at the end of the experiment to examine histopathological changes that are consistent with diffuse alveolar damage to diagnose ARDS, which is not feasible in standard clinical care and clinical research studies. The adjudication of animals’ last breath samples compared to the presence of histopathological adjudicated diffuse alveolar damage provided increased accuracy and confidence in the training set. 3) We were able to perform detailed longitudinal studies (from the healthy pre-ARDS state to the final death due to ARDS), which helps better delineate the trajectory of ARDS. This could be vital for guided therapy and decision-making. Finally, we identified a physiologically relevant VOC profile similar to that which we previously found in humans with ARDS [13] (see detailed discussion in the supplementary material, section S3). As a class of compounds, VOCs are highly relevant to the detection of ARDS because many are alkanes (e.g. pentane, heptane) and alkenes (e.g. α-pinene), which are by-products of inflammatory processes [3, 28–35]. The VOC pattern found in both our human and swine studies is consistent with what has been previously reported in the literature [3, 4] and is most often attributable to fatty acid peroxidation [36]. Lipid peroxidation (the oxidative degradation of lipid membranes that leads to cell damage and dysfunction) is mediated by reactive oxygen species, most likely generated by leukocytes [37, 38], which is consistent with what is known about ARDS pathogenesis [39].
The current study has several limitations. First, we used only five animals with limited data points. Consequently, we were unable to separate the training and testing sets by animal identifiers. As such the training and testing sets have observations from the same animal at different time points. Although we conducted cross-validation, we expect improvement in mean accuracy and standard deviation with increased datasets. Second, classification of the severity of ARDS (i.e. mild, moderate and severe) was not attempted due to lack of transition data points. In future, this work may be possible with increased numbers of swine and transition data points. Third, we identified seven biomarkers using the swine model, compared to nine in the human study. This may be due to the limited number of swine and the breath samples used in this study. Additional swine experiments will be needed to determine the validity of identified compounds for ARDS detection. Therapies that change the trajectory of ARDS by treating underlying causes such as sepsis could be instituted in the future to allow further dynamic perturbation of VOCs to understand whether the technology can track changes prior to standard clinical metrics. Finally, by design our swine model of ARDS is multifactorial in aetiology, and our study design does not enable us to determine which exhaled breath signals are attributable to ARDS itself or the constituent exposures of our model (e.g. sepsis, aspiration). Further work will determine the generalisability of our findings.
Conclusion
In conclusion, breath analysis using a portable GC has been presented as an alternative for rapid diagnostic and trajectory monitoring of ARDS. The performance of this methodology in delineating ARDS from pre-ARDS is excellent and provides encouraging conceptual evidence at the experimental level. Continuous monitoring of VOCs produced by ARDS opens up the potential for trajectory monitoring, which will have implications for earlier interventions. Using a high-fidelity swine model to study exhaled breath significantly enhances the ability to study ARDS and to test new technologies aimed at improving its diagnosis, monitoring and treatment.
Footnotes
Provenance: Submitted article, peer reviewed.
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: R. Sharma has nothing to disclose.
Conflict of interest: M. Zhou has nothing to disclose.
Conflict of interest: M.H. Tiba reports grants from the Michigan Institute for Clinical and Health Research during the conduct of the study.
Conflict of interest: B.M. McCracken has nothing to disclose.
Conflict of interest: R.P. Dickson has nothing to disclose.
Conflict of interest: C.E. Gillies has nothing to disclose.
Conflict of interest: M.W. Sjoding has nothing to disclose.
Conflict of interest: J.A. Nemzek has nothing to disclose.
Conflict of interest: K.R. Ward has equity in Blue Biotech LLC, a new company that has optioned technology from the University of Michigan.
Conflict of interest: K.A. Stringer has nothing to disclose.
Conflict of interest: X. Fan reports grants from Blue Biotech LLC, which has an option agreement with the University of Michigan to license the breath analysis technology invented by X. Fan. It also sponsors X. Fan's laboratory at the University of Michigan to develop micro-gas chromatography devices for potential breath analysis use. In addition, X. Fan has a patent (10,705,061) for a microfluidic photoionisation detector issued to Nanova Environmental. In the article, a gas chromatography device was used to analyse breath. The gas chromatography device used this detector. However, the results presented in this article should be valid regardless of the device and detector.
Support statement: The authors are grateful for support from the National Institutes of Health (NIH) (1R21HL139156), the Flux HPC Cluster provided by the University of Michigan Office of Research and Advanced Research Computing–Technology Services, and the Analytical Chemistry Lab at the UM Biological Station at Pellston. The development of the swine model of ARDS was supported by the Michigan Center for Integrative Research in Critical Care and the Michigan Institute for Clinical and Health Research (MICHR) Accelerating Synergy Award. MICHR is supported by a National Center for Advancing Translational Sciences award (UL1TR002240) from the NIH. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received March 7, 2021.
- Accepted September 19, 2021.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










