





Abstract
Introduction There is no established clinical prediction model for in-hospital death among patients with pneumonic COPD exacerbation. We aimed to externally validate BAP-65 and CURB-65 and to develop a new model based on the eXtreme Gradient Boosting (XGBoost) algorithm.
Methods This multicentre cohort study included patients aged ≥40 years with pneumonic COPD exacerbation. The input data were age, sex, activities of daily living, mental status, systolic and diastolic blood pressure, respiratory rate, heart rate, peripheral blood eosinophil count and blood urea nitrogen. The primary outcome was in-hospital death. BAP-65 and CURB-65 underwent external validation using the area under the receiver operating characteristic curve (AUROC) in the whole dataset. We used XGBoost to develop a new prediction model. We compared the AUROCs of XGBoost with that of BAP-65 and CURB-65 in the test dataset using bootstrap sampling.
Results We included 1190 patients with pneumonic COPD exacerbation. The in-hospital mortality was 7% (88 out of 1190). In the external validation of BAP-65 and CURB-65, the AUROCs (95% confidence interval) of BAP-65 and CURB-65 were 0.69 (0.66–0.72) and 0.69 (0.66–0.72), respectively. XGBoost showed an AUROC of 0.71 (0.62–0.81) in the test dataset. There was no significant difference in the AUROCs of XGBoost versus BAP-65 (absolute difference 0.054; 95% CI −0.057–0.16) or versus CURB-65 (absolute difference 0.0021; 95% CI −0.091–0.088).
Conclusion BAP-65, CURB-65 and XGBoost showed low predictive performance for in-hospital death in pneumonic COPD exacerbation. Further large-scale studies including more variables are warranted.
Abstract
BAP-65, CURB-65 and the XGBoost model show low predictive performance for in-hospital death in pneumonic COPD exacerbation. Further large-scale studies with more variables are warranted to develop an ideal prognostic model. https://bit.ly/3m0ISLA
Introduction
COPD is a common respiratory disease that is characterised by airflow limitation due to chronic inflammation of the airways and lungs [1]. Patients with COPD often experience acute worsening of baseline symptoms, and with coexisting consolidation (pneumonic COPD exacerbation) on chest imaging, mortality is increased compared to non-pneumonic COPD exacerbation [2]. A previous study suggested that pneumonic COPD exacerbation might have a different inflammation profile from non-pneumonic COPD exacerbation [3, 4].
CURB-65 (confusion, blood urea nitrogen >19 mg·dL−1, respiratory rate ≥30 breaths·min−1, systolic blood pressure <90 mmHg or diastolic blood pressure ≤60 mmHg and age ≥65 years) is a simple prediction model in patients with community-acquired pneumonia and has been validated internally and externally [5, 6]. On the other hand, BAP-65 (blood urea nitrogen ≥25 mg·dL−1, altered mental status, heart rate ≥109 beats·min−1 and age ≥65 years) is an easily computable prediction model in patients with COPD exacerbation that has shown good performance in internal validation and external validation cohorts [7, 8]. However, we could not evaluate how many patients with pneumonic COPD exacerbation were included in those studies. Another study showed that CURB-65 had poor predictive ability for death in pneumonic COPD exacerbation [9].
To date, there is no established clinical prediction model specifically for the population with pneumonic COPD exacerbation. It is also unclear whether BAP-65 and CURB-65 can be applied to patients with pneumonic COPD exacerbation [10]. Our study had two purposes: 1) the external validation of BAP-65 and CURB-65 for predicting in-hospital death among patients with pneumonic COPD exacerbation; and 2) the development of a high-performance clinical prediction model using a modern machine learning algorithm that is gaining ground in the medical field [11].
Methods
Study design
Our study was a multicentre retrospective cohort study conducted across five acute care hospitals in Japan. To maximise patient capture, patient data were collected during different periods in each hospital between April 1, 2008, and July 31, 2020.
Pneumonic COPD exacerbation is diagnosed when the criteria for both pneumonia and COPD exacerbation are met [4, 12, 13]. To select patients with pneumonic COPD exacerbation, we used the validated algorithm based on the 10th revision of the International Classification of Diseases and Related Health Problems (supplementary eFigure S1) [4]. First, patients aged ≥40 years who had both pneumonia and COPD exacerbation were selected. Patients with other differential diagnoses mimicking pneumonic COPD exacerbation were excluded, including heart failure, pneumothorax, asthma exacerbation and obstructive pneumonia.
This study was approved by the institutional review board of each hospital (approval number 200811). This article was reported according to the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) statement (supplementary eTable S1) [14].
Input and output data
The following input data on the day of admission were collected from the data warehouse or electronic medical records in each hospital: age, sex, the activities of daily living status (full support or not), mental status (altered mental status or not), vital signs (systolic and diastolic blood pressure, respiratory rate and heart rate), laboratory results (peripheral blood eosinophil count and blood urea nitrogen) and presence of tracheal intubation. Activities of daily living were defined as full support when the Barthel index was zero, and altered mental status was defined as a Japan Coma Scale score ≥1. These two variables are used for administrative purposes in the Japanese original case-mix classification system or Diagnosis Procedure Combination [15, 16]. The Ministry of Health, Labour and Welfare regularly evaluates the trend, quality and cost of the healthcare system using Diagnosis Procedure Combination data. We extracted data from the database containing Diagnosis Procedure Combination data submitting the anonymised patient data to the Ministry of Health, Labour and Welfare. Our variable selection was based on existing clinical prediction models of pneumonia or COPD exacerbation [5, 7, 17]. We did not collect data on other comorbidities from the Diagnosis Procedure Combination database because these variable codes were not fully externally validated. The primary outcome was in-hospital death, which was derived from the electronic medical records in each hospital.
Statistical analysis
The study process is illustrated in figure 1. Patient characteristics were summarised as means for continuous variables and as percentages for categorical variables. All statistical analyses were performed using R software version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria). The scripts are available in the GitHub repository (https://github.com/AkihiroShiroshita/Prediction-model-for-Pnuemonic-COPD-exacerbation.git).

Patient selection flow and framework of the study process. XGBoost: eXtreme Gradient Boosting.
External validation of BAP-65 and CURB-65
We conducted the external validation of BAP-65 and CURB-65 with respect to the entire dataset to evaluate their performance in a large sample size. We calculated the sensitivity and specificity using each total score as the cut-off point. To assess the calibration ability, we summarised the mortality according to each total risk score. To assess the discriminatory ability of the two models, we calculated the area under the receiver operating characteristic curve (AUROC). We used multiple imputation to cope with missing data [18]. We created a total of 100 datasets using multiple imputation with chained equations and calculated the AUROC within each dataset. Thereafter, we combined the estimates of AUROC using Rubin's combining rule [19, 20].
Model development via machine learning
We used the eXtreme Gradient Boosting (XGBoost) algorithm to develop a clinical prediction model for in-hospital death among patients with pneumonic COPD exacerbation. The XGBoost algorithm is a powerful ensemble method of machine learning that combines a set of weak learners of the decision tree [21]. Its parallel computation enables the efficient and accurate development of a prediction model. Because it extracts variable importance, imputation of missing data, scaling or normalisation is not required. What is required in the algorithm is the proper tuning of the hyperparameters, which are parameters that control the behaviour of the model. In our study, the original data were first partitioned into training and test datasets. We used the stratified sampling method with a 7:3 ratio for data splitting, which allowed the two datasets to have similar in-hospital mortality. Second, we developed prediction models using a training dataset. We performed a grid search with four-fold cross-validation to obtain the optimal hyperparameters for maximising the mean AUROC (supplementary eFigure 2) [21]. In the grid search, the hyperparameter candidates for max_depth (maximum tree depth) was {2, 4, 6, 8, 10}, and min_child_weight (minimum degree of impurity needed in a node) was {1, 2, 3, 4, 5}. After fixing max_depth and min_child_weight, we searched the maximum number of trees based on the cross-validation. We set the remaining hyperparameters as default. Third, for external validation, we validated the trained model using the test dataset. We used the AUROC as an index to validate the model. Finally, the importance of the variables based on the impurity metric was plotted. Impurity is the degree of misclassification. It displays the degree to which each input dataset influences the output in our XGBoost model.

Important variables based on the impurity metric. Blood urea nitrogen was the most important feature. Activities of daily living and sex were of little importance.
Model comparison
We compared the model performances of the three prediction models using the test dataset to allow comparison on a one-to-one basis. To evaluate the discriminatory performance, we described the receiver operating characteristic (ROC) curves of the three prediction models. Thereafter, we estimated the differences in AUROCs using bootstrap sampling (BAP-65 versus XGBoost, and CURB-65 versus XGBoost) [22]. The XGBoost model can take into account missing data while BAP-65 and CURB-65 cannot. The XGBoost model used the whole test dataset while BAP-65 and CURB-65 only used the patient data without missing values.
Results
The patient selection flowchart is shown in figure 1. We initially selected 1431 patients. After excluding 241 patients with other diagnoses, 1190 patients with pneumonic COPD exacerbation were included in our analysis. Patient characteristics are summarised in table 1. The in-hospital mortality rate was 88 out of 1190 (7%). The number of intratracheal intubations was 16 out of 1190 (1%) and median length of hospital stay was 12 (interquartile range: 8–18) days.
Patient characteristics
External validation of BAP-65 and CURB-65
Table 2 presents a summary of the number of patients with each total score. The calibration performances of both prediction models were low. The AUROC of BAP-65 was 0.69 (95% CI 0.66–0.72) and that of CURB-65 was 0.69 (95% CI 0.66–0.72). The discriminatory performance of both prediction models was also low.
Risk scores and in-hospital mortality of BAP-65 and CURB-65
Model development via machine learning
Based on the results of the grid search, we set up the hyperparameters as follows: max_depth (maximum tree depth) = 4, min_child_weight (minimum degree of impurity needed in a node) = 2, eta (learning rate) = 0.1, subsample (the proportion of cases to be randomly sampled for each tree) = 0.8, colsample_bytree (the proportion of predictor variables sampled for each tree) = 0.8, gamma (minimal loss to expand on a leaf node) = 0, lambda (L2 regularisation term on weights) = 1, alpha (L1 regularisation term on weights) = 0, scale_pos_weight (balance of positive and negative weights) = 1 and maximum number of trees = 37. Cross-validation of the developed model revealed a mean AUROC of 0.76, and external validation in the test dataset revealed an AUROC of 0.72 (95% CI 0.62–0.82). Feature importance is illustrated in figure 2, which shows that blood urea nitrogen was the most important factor for predicting in-hospital death. Systolic blood pressure and altered mental status also had important roles in the XGBoost model. On the contrary, activities of daily living and sex showed little importance.
Model comparison
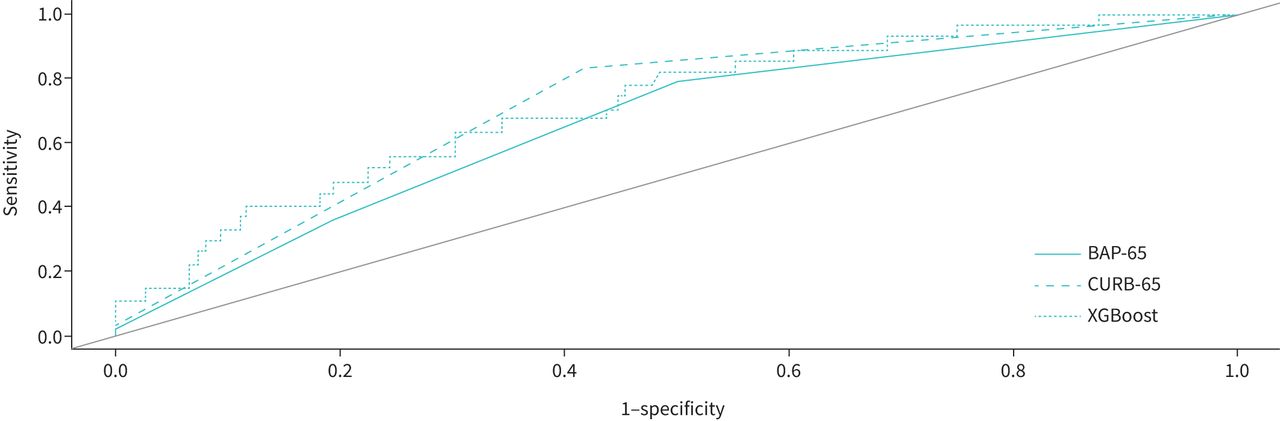
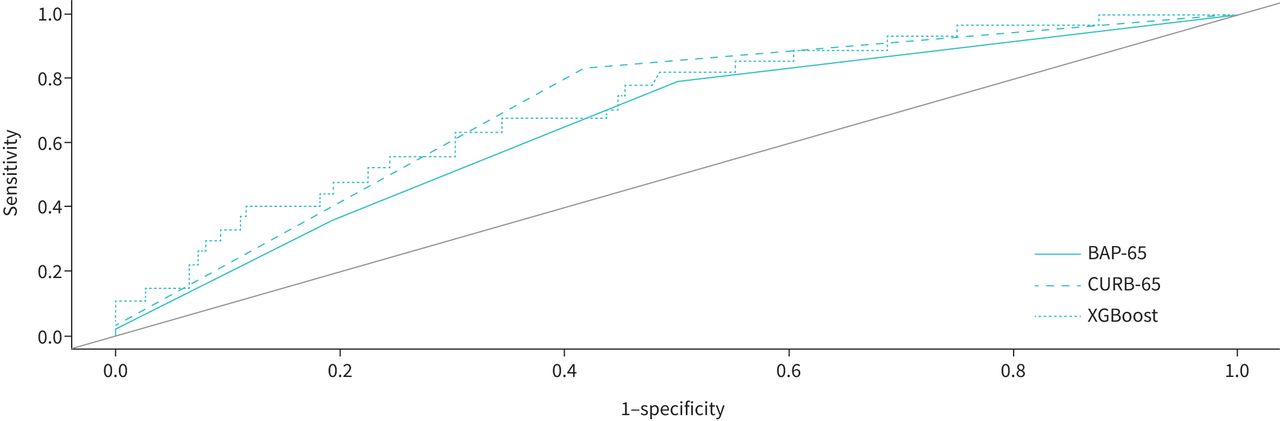
We performed model comparisons using the test data. The XGBoost model used the whole test dataset (n=357), while BAP-65 and CURB-65 used the data of 314 and 281 patients, respectively, because of missing values. Figure 3 shows the ROC curves of the BAP-65, CURB-65 and XGBoost models. There was no significant difference in AUROCs between the XGBoost model and BAP-65 (absolute difference 0.054; 95% CI −0.057–0.16) or between the XGBoost model and CURB-65 (absolute difference 0.0021; 95% CI −0.091–0.088).
{kind=link}
{kind=link}
{kind=link}
The receiver operating characteristic curves of BAP-65, CURB-65 and the eXtreme Gradient Boosting (XGBoost) model in the test dataset. The XGBoost model showed the best discriminatory performance.
Discussion
Our study revealed that contrary to the study results for either pneumonia or COPD exacerbation, all three models (BAP-65, CURB-65 and XGBoost model) had low discriminatory ability for predicting in-hospital death among patients with pneumonic COPD exacerbation. Further large-scale studies are needed to develop a specific clinical prediction model for pneumonic COPD exacerbation.
The two simple scoring systems, i.e. BAP-65 and CURB-65, showed low predictive performance in our dataset of patients with pneumonic COPD exacerbation. Although our study did not contrast their predictive abilities in either pneumonia or COPD exacerbation with pneumonic COPD exacerbation, CURB-65 was externally validated for the Japanese population and BAP-65 was validated for the Chinese population [23, 24]. Contrary to the results in either pneumonia or COPD exacerbation, CURB-65 or BAP-65 was not externally validated in our patient cohort. Our results were consistent with those of a previous retrospective cohort study that revealed CURB-65 had poor performance for predicting death in pneumonic COPD exacerbation, while it had high performance for non-pneumonic COPD exacerbation [9]. Our target population included patients with a specific category of pneumonic COPD exacerbation. The disease spectrum of pneumonic COPD exacerbation, which fulfils the diagnostic criteria for both pneumonia and COPD exacerbation, may differ from that of COPD exacerbation and pneumonia. A specific clinical prediction model for pneumonic COPD exacerbation is warranted.
A strength of our study was the use of a powerful machine learning technique that can overcome the drawbacks of the development processes of BAP-65 and CURB-65. However, the XGBoost model also had a low predictive performance for in-hospital deaths in pneumonic COPD exacerbation. Contrary to the recursive partition that was used in the development of BAP-65, the XGBoost model avoids model instability [5, 25]. In addition, unlike logistic regression, which was used in the development of CURB-65, the XGBoost model is not based on the assumption of linearity and does not require the categorisation of continuous variables [5]. It can also find the optimal interaction terms between variables. Despite its great ability, our XGBoost model did not show high performance.
However, our study had several weaknesses. First, our sample may have been too small to develop internally and externally validated prediction models. The number of events required for model development is at least 10 events per variable [26]. Our input data included 10 variables, and at least 100 events were required; however, there were only about 60 events in our training dataset. Although we used the XGBoost model, which may require a smaller sample size, we could not overcome the problem in our dataset [27]. Second, other missing variables should have been included in the model. For example, in a previous study, the DECAF score, a simple and validated scoring system for predicting outcomes in COPD exacerbation, tended to have a higher predictive performance than CURB-65 in pneumonic COPD exacerbation [9]. However, we could not collect the values for the Extended Medical Research Council Dyspnoea Scale, arterial blood gas analysis results or atrial fibrillation because they were not routinely collected in our clinical site, and they could be additional candidates for future prediction models. According to a systematic review of prediction models for COPD exacerbation, patients’ baseline characteristics such as body mass index, forced expiratory volume in 1 s, and previous COPD exacerbation were used in studies with a low risk of bias [28]. These could also be additional candidates for future models.
The feature importance plot in our study highlighted the importance of blood urea nitrogen, systolic blood pressure and altered mental status. These variables should be included in a new clinical prediction model for pneumonic COPD exacerbation. On the contrary, activities of daily living and sex were of little importance in the model. In our study, the activities of daily living were categorised as full support or not, and this might have led to the loss of notable information. ∼90% of the included patients were men, which may have led to the unimportance of sex as a variable. Our study revealed some candidates for the included variables in developing a new model.
In our study, we could not conclude which clinical model was superior. In our test dataset, the number of patients was ∼300, and the in-hospital mortality was 25, which was much smaller than the necessary sample size for precise external validation [29, 30]. The results of the external validation of BAP-65 and CURB-65 in the whole dataset showed that the predictive ability for in-hospital death appeared to be similar for CURB-65 and BAP-65. Physicians who use either BAP-65 or CURB-65 will not have to change their practice based on our study.
Our study had several limitations. First, as pointed out above, our sample size was small. Because we could not include additional patients after the patient enrolment period or incorporate another patient cohort, we could not address the problem. Second, only Japanese patients were included, suggesting a lack of generalisability. Third, the primary outcome in our study was in-hospital mortality, and long-term outcomes could not be evaluated. Fourth, we could not set aside an additional dataset for external validation before splitting the dataset. Because we performed external validation on the split dataset, the AUROC in the test dataset may have been overestimated. Fifth, altered mental status was evaluated based on the Japan Coma Scale. Although this scale has been widely used in Japan because of its simplicity, its accuracy has not been validated in patients with COPD. Sixth, we could not collect data on the patients’ code status (do-not-intubate or not). In our study, the rate of tracheal intubation was lower than mortality. This may have decreased the generalisability of our study results to intensive care units. To overcome these limitations, large-scale studies from different regions are needed.
Conclusion
BAP-65, CURB-65 and the XGBoost model showed poor performance in predicting in-hospital death among patients with pneumonic COPD exacerbation. Further large-scale studies with more variables are needed to develop a new prognostic model for pneumonic COPD exacerbation.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00452-2021.SUPPLEMENT
Footnotes
Provenance: Submitted article, peer reviewed.
Author contributions: A. Shiroshita, K. Yuya, H. Shiba, C. Shirakawa, K. Sato, S. Matsushita, K. Tomii and L. Yuki contributed to the conception and design of the work. A. Shiroshita, H. Shiba, C. Shirakawa, K. Sato, S. Matsushita and K. Tomii contributed to data acquisition. A. Shiroshita, K. Yuya and K. Yuki contributed to the data analysis and interpretation. A. Shiroshita, K. Yuya and K. Yuki drafted the manuscript. All authors revised the manuscript critically and approved the final version of the manuscript. A. Shiroshita, K. Yuya, H. Shiba, C. Shirakawa, K. Sato, S. Matsushita, K. Tomii and K. Yuki agreed to be accountable for all aspects of any part of the work.
This article has supplementary material available from openres.ersjournals.com
Data availability statement: The datasets generated and/or analysed during the current study are not publicly available due to the privacy issues but are available from the corresponding author on reasonable request.
Conflict of interest: A. Shiroshita has nothing to disclose.
Conflict of interest: Y. Kimura has nothing to disclose.
Conflict of interest: H. Shiba has nothing to disclose.
Conflict of interest: C. Shirakawa has nothing to disclose.
Conflict of interest: K. Sato has nothing to disclose.
Conflict of interest: S. Matsushita has nothing to disclose.
Conflict of interest: K. Tomii has nothing to disclose.
Conflict of interest: Y. Kataoka has nothing to disclose.
Support statement: Funding for English language editing was obtained from Ichinomiyanishi Hospital. The funder played no role in the study design, study execution, data analyses, data interpretation, or decision to submit the report. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received July 7, 2021.
- Accepted December 4, 2021.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










