





Abstract
Continuous positive airway pressure is an efficacious and cost-effective modality of treatment for #COVID19 ARDS, particularly in resource-poor settings with late referrals to overwhelmed intensive care units https://bit.ly/3dKwXwP
To the Editor:
Management of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-associated acute respiratory distress syndrome (coronavirus disease 2019 (COVID-19) ARDS or CARDS) has challenged the health systems of developed countries, and even more so the health systems of resource-poor settings [1]. Within this context, continuous positive airway pressure (CPAP) has been trialled as an alternative, less resource-intensive respiratory support to early invasive mechanical ventilation (IMV) [2] with promising results, and now features in some major guidelines [3]. However, there are limited studies from resource-poor settings that have been impacted massively by COVID-19. We retrospectively analysed the completed survival outcomes and characteristics for the exclusive use of CPAP for moderate-to-severe CARDS as defined by the Kigali criteria [4] in a cohort of patients admitted to Bach Christian Hospital (BCH; Abbottabad, Pakistan) between April and August 2021.
BCH is a small 60-bed secondary level hospital in rural Northern Pakistan (Khyber Pakhtunkhwa Province). A COVID-19 unit was opened at BCH in December 2020 to respond to the surge of severely unwell COVID-19 patients in Pakistan's “second wave”. This contained nine high-dependency unit beds with appropriate step-down patients transferred to another ward. Nursing staff with limited previous critical care experience were trained in the management of critically unwell patients, the use of CPAP and arterial blood gas (ABG) sampling. The unit was staffed by a single nurse and nurse aide.
Patients were admitted to the COVID-19 unit at BCH based on respiratory failure (peripheral oxygen saturation (SpO2) <90% or respiratory rate >30 breaths·min−1) in the presence of a clinical history and examination suggestive of COVID-19 pneumonia with appropriate radiological and laboratory findings. SARS-CoV-2 PCR was performed on patients who could afford it, but was limited due to cost and availability [5]. However, all patients tested had positive results, and COVID-19 antigen testing was implemented from August 2021.
Ethical approval was obtained from the hospital committee for this observational study.
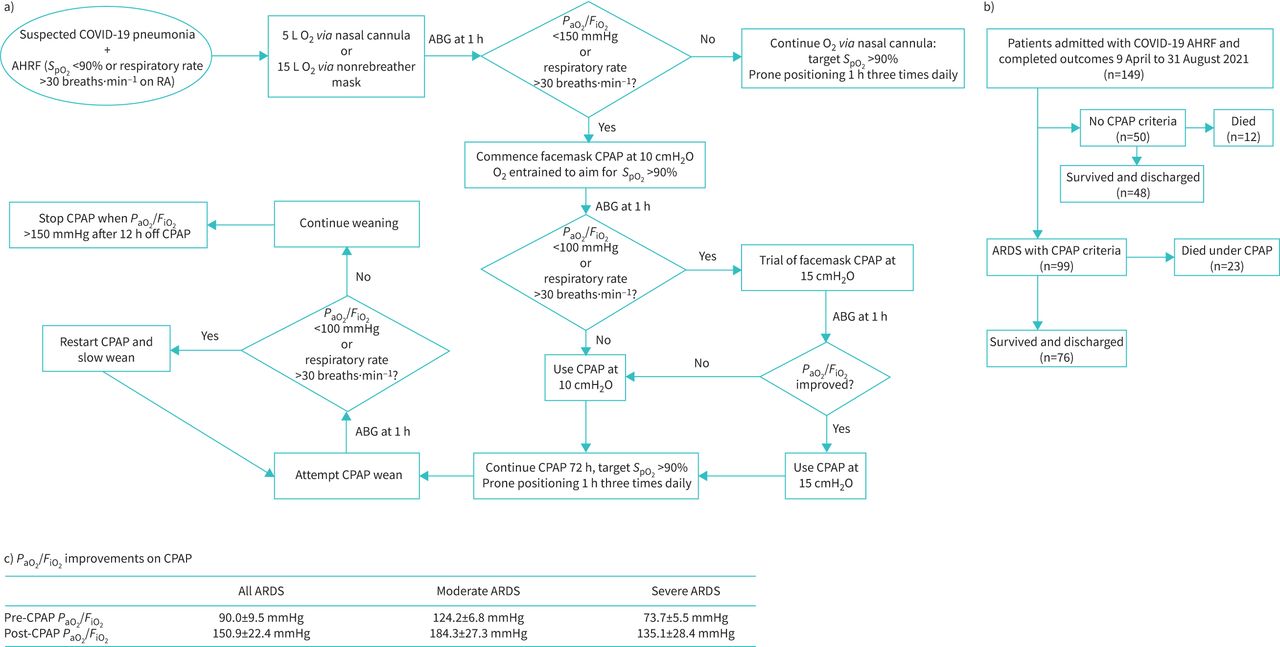
Patients were initially resuscitated with 5 L oxygen (O2) via nasal cannula or 15 L O2 via nonrebreather mask, depending on severity, with a target SpO2 of 95% (figure 1a). After 1 h clinical assessment was performed using ABG, and those with persistent tachypnoea or arterial oxygen tension (PaO2)/inspiratory oxygen fraction (FiO2) ratio <150 mmHg (corresponding to requiring more than >5 L O2 via nasal cannula to maintain SpO2 >90%) were commenced on CPAP at 10 cmH2O, as recommended by United Kingdom guidelines [6] and the initial study from Genoa [2].
{kind=link}
a) Respiratory support algorithm for coronavirus disease 2019 (COVID-19) acute respiratory distress syndrome (CARDS); b) completed outcomes for patients admitted with acute hypoxaemic respiratory failure (AHRF) April to August 2021; c) improvement in oxygenation with continuous positive airway pressure (CPAP) for moderate and severe CARDS (results for initial cohort April to May 2021 with complete data; n=31). Data are presented as mean±95% CI. SpO2: peripheral oxygen saturation; RA: room air; O2: oxygen; ABG: arterial blood gases; PaO2: arterial oxygen tension; FiO2: inspiratory oxygen fraction.
Philips Respironics CPAP machines originally intended for home use for obstructive sleep apnoea were used with their default Amara full-face masks, with the addition of antibacterial/antiviral heat and moisture exchange filters. Philips advise a separate inflow attachment for O2 entrainment [7], but in the absence of these pieces, O2 was entrained via a T-tube to the machine end of the CPAP tubing. O2 was supplied from a wall flow meter with a capacity of up to 15 L·min−1.
Clinical status was reassessed by ABG after 1 h on CPAP. Those who had improved on CPAP 10 cmH2O were placed on continuous CPAP for 72 h, as recommended by an Italian protocol [8], with breaks for eating and drinking. Those who failed to improve sufficiently on 10 cmH2O CPAP were given a trial of 15 cmH2O CPAP, which has been described in Italian and Scottish guidelines [9, 10]. If patients improved significantly at 15 cmH2O, that pressure was continued. Otherwise, 10 cmH2O was used for all patients, given the risks of barotrauma at pressures >10 cmH2O. All patients on oxygen, including those on CPAP, were encouraged to undergo prone positioning for ⩾1 h three times daily [11]. Those unable to tolerate complete proning were encouraged to undergo semi-prone positioning.
CPAP weaning was attempted after 72 h of continuous CPAP. CPAP was stopped when PaO2/FiO2 off CPAP was >150 mmHg, or SpO2 >90% was maintained on 5 L O2 via nasal cannula. Patients who failed to wean off CPAP at all were given another 72 h of continuous CPAP and weaning was reattempted afterwards.
Steroids (dexamethasone) with appropriate thromboprophylaxis (rivaroxaban, due to lack of availability of low molecular weight heparin) formed the mainstay of medical management. Remdesivir was not used, due to lack of evidence of efficacy in severe disease, and tocilizumab was used in select patients from July, as per the updated World Health Organization guidelines [12].
149 patients were admitted with suspected COVID-19 acute hypoxaemic respiratory failure at BCH from 9 April to 31 August 2021. 99 patients met criteria for moderate-to-severe ARDS and were commenced on CPAP regardless of age or underlying comorbidities. 76 patients survived on CPAP (figure 1b).
The duration of successful CPAP ranged from 5 to 21 days. Complications on CPAP included barotrauma, particularly with higher pressures. Four patients on 15 cmH2O developed these complications (n=2 pneumothorax, n=2 pneumomediastinum), while only one patient on 10cm H2O had this complication (n=1 pneumomediastinum). The patients with pneumothorax had chest tube insertion, but even so, all five of these patients died. However, this rate of barotrauma (five (5%) out of 99 patients) is similar to that reported elsewhere for noninvasive ventilation (NIV) in CARDS, which is lower than rates observed for IMV [13].
Patients with CARDS demonstrated improvement in oxygenation with CPAP (figure 1c). FiO2 on simple oxygen including nasal cannula was approximated using the Shapiro formula [14], and a white paper from Philips was used to estimated FiO2 on CPAP [7].
No healthcare-associated infections were reported among staff.
Our survival rate on CPAP (76.8% total) is slightly lower than the 83% reported in the original study on CPAP in CARDS from Genoa [2]. However, the original study excluded a significant number of patients who were not considered fit for resuscitation, while all patients received CPAP as per protocol in this study, regardless of pre-morbid state. Our survival rate is significantly higher than the 29% reported in patients treated exclusively with CPAP in another Italian series [15]; however, it is likely that these patients had a greater frequency of underlying comorbidities, as they were classed ineligible for intubation. The CARDS survival rate for CPAP at our centre is not too dissimilar to reported rates (∼80%) from intensive care units (ICUs) employing NIV and IMV in resource-rich settings [16], suggesting that CPAP is feasible as a ceiling of care treatment modality in pandemic circumstances. Even more significantly, the survival rate is higher than the dire outcomes in ICUs employing IMV in resource-poor settings inundated by late referrals [1]. CPAP is less resource-intensive in terms of equipment and staffing, and healthcare workers can be easily trained in its operation. Early implementation of CPAP for CARDS in a non-ICU setting as opposed to late referral to an already overwhelmed ICU for IMV is likely to save many lives.
Significant limitations of this study include its observational nature, retrospective single-centre design and small sample size.
CPAP is an efficacious and cost-effective modality of treatment for CARDS, particularly in resource-poor settings, which now bear most of the pandemic burden.
Acknowledgements
Many thanks to our dedicated nursing staff (Bach Christian Hospital, Abbottabad, Pakistan) for their work with COVID-19 patients and help with data collection, particularly Rizwan Hameed and Shahzad Gill. We are thankful to Luke Cutherell, Musheer Shaukat, Zubaid Inayat and Nabila Michael for their support and encouragement with the work of our COVID-19 unit.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: The authors have nothing to disclose.
- Received August 25, 2021.
- Accepted December 4, 2021.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org










