





Figures
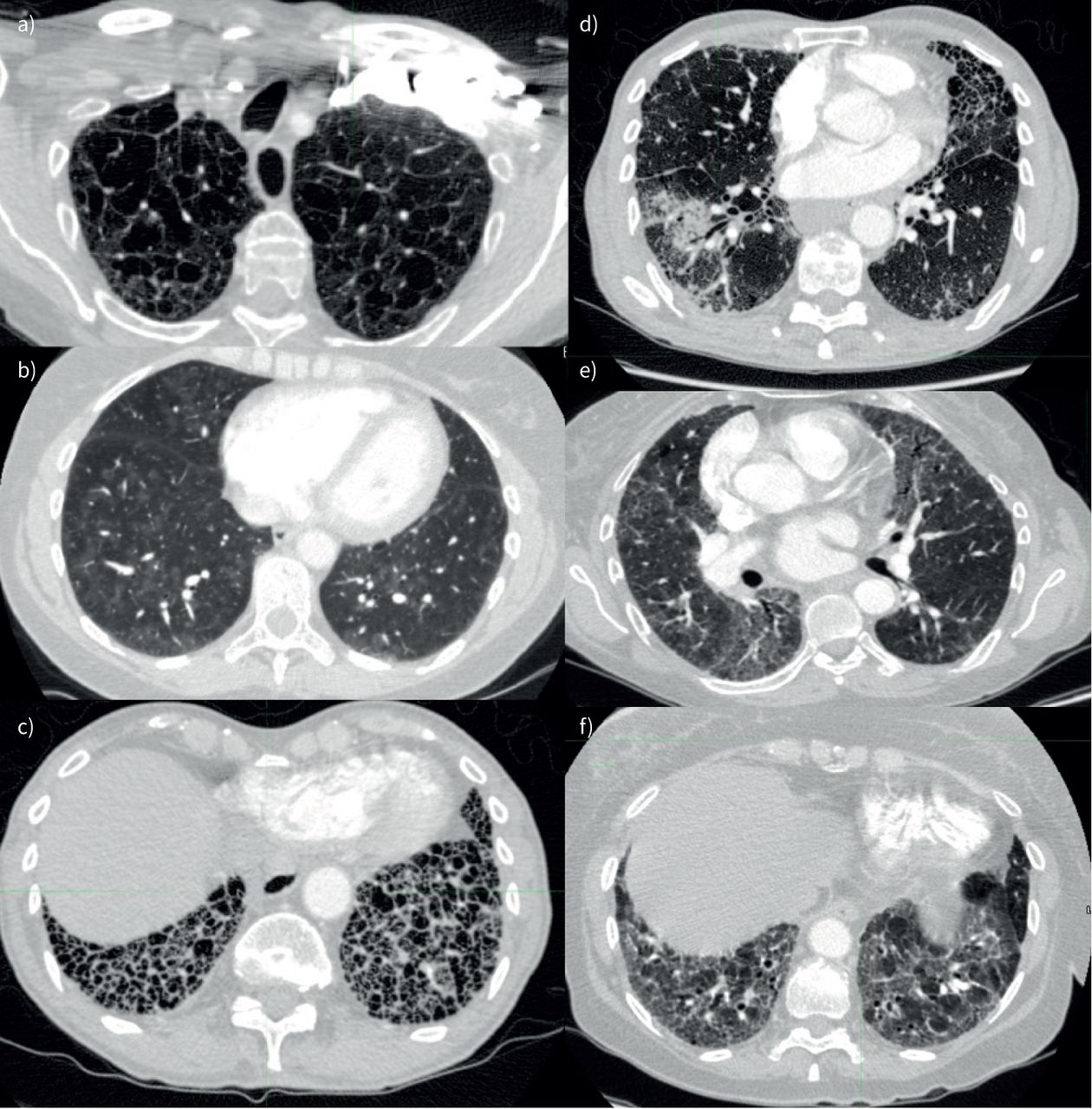
- FIGURE 1
Computed tomography lung parenchymal patterns assessed. a) Emphysema, b) centrilobular ground glass change (windowed to emphasise subtle pattern), c) honeycombing, d) consolidation (with surrounding ground glass change), e) ground glass change and f) fibrosis.
- FIGURE 2
CONSORT (Consolidated Standards of Reporting Trials) flow diagram showing selection of study cohort. CTEPH: chronic thromboembolic pulmonary hypertension; LHD-PH: pulmonary hypertension with left heart disease; PH-CLD: PH due to chronic lung disease and/or hypoxia; OHS: obesity hypoventilation syndrome; OSA: obstructive sleep apnoea; RHC: right heart catheterisation; PAH: pulmonary arterial hypertension; IPAH: idiopathic pulmonary arterial hypertension; FPAH: familial pulmonary arterial hypertension; CT: computed tomography; IPAH-noLD: idiopathic pulmonary arterial hypertension with no lung disease; IPAH-LD: idiopathic pulmonary arterial hypertension with lung disease; CGG: centriobular ground glass.
- FIGURE 3
Kaplan–Meier survival curves stratified by computed tomography features of CGG, emphysema and fibrosis for: a) all patients, b) patients initially diagnosed with IPAH and c) patients initially diagnosed with PH-CLD. IPAH: idiopathic pulmonary arterial hypertension; PH-CLD: PH due to chronic lung disease and/or hypoxia; CGG: centrilobular ground-glass; CPFE: combined pulmonary fibrosis and emphysema.
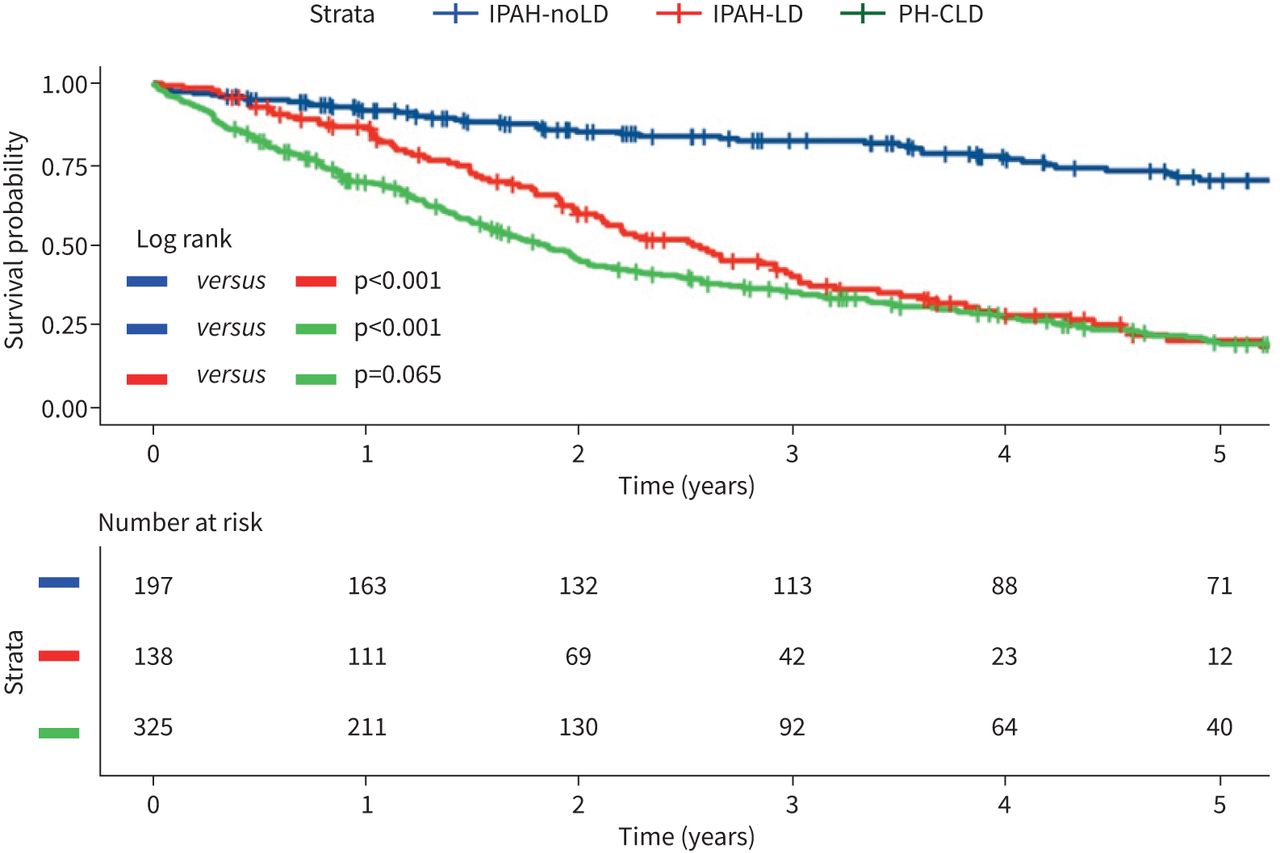
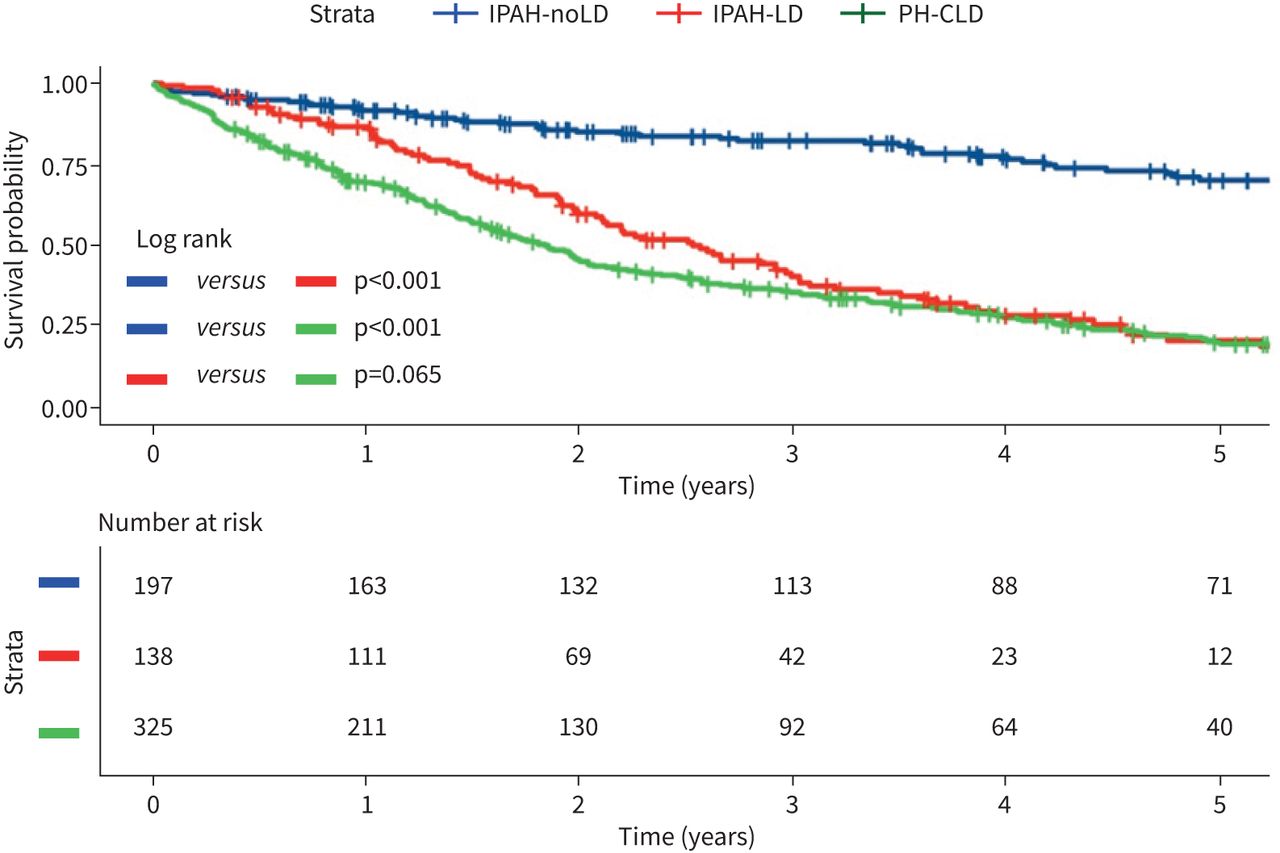
- FIGURE 4
Kaplan–Meier survival curves for patients classified as IPAH-LD, IPAH-noLD and PH-CLD. IPAH-noLD: idiopathic pulmonary arterial hypertension with no CT features of lung disease; IPAH-LD: idiopathic pulmonary arterial hypertension with CT features of lung disease; PH-CLD: pulmonary hypertension associated with chronic lung disease.
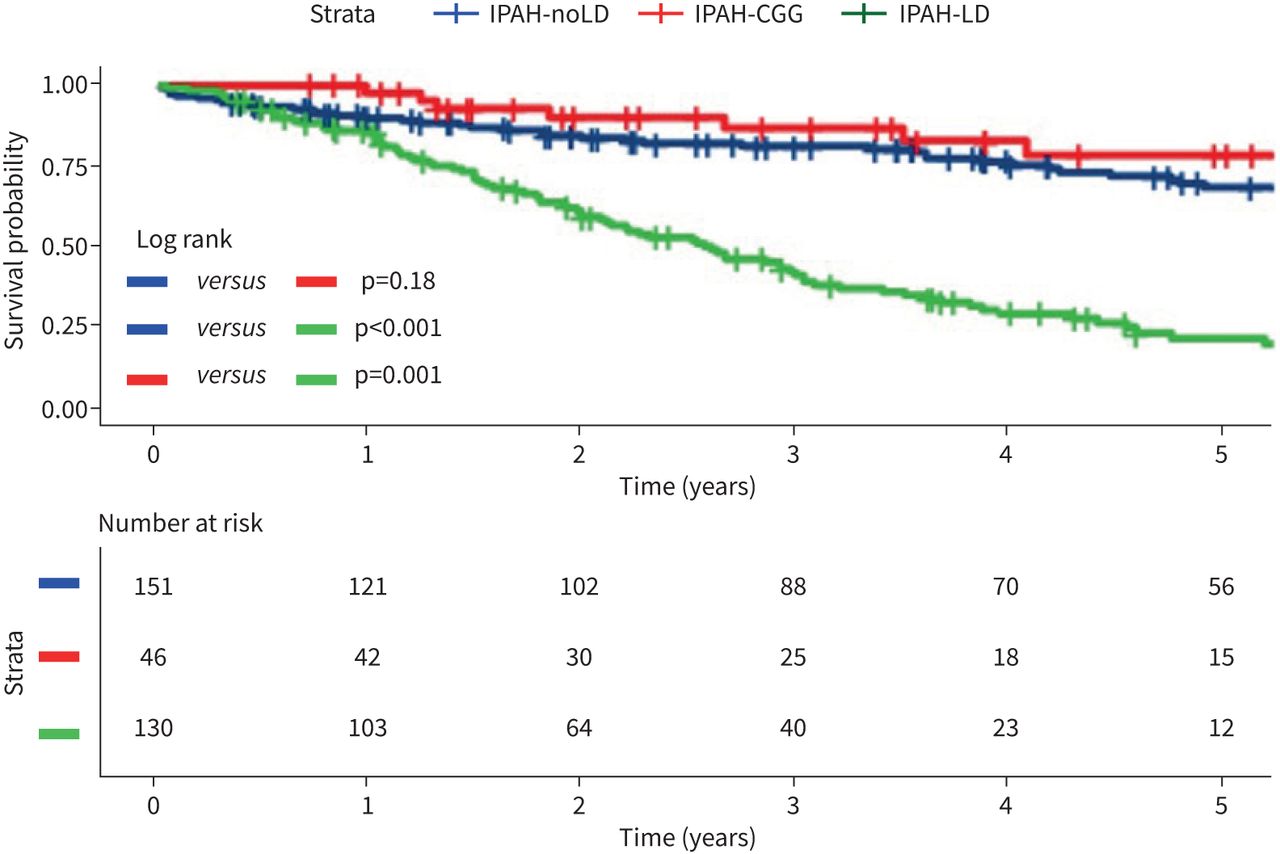
- FIGURE 5
Kaplan–Meier curve comparing survival in IPAH-noLD, IPAH-LD and IPAH-CGG. IPAH-noLD: idiopathic pulmonary arterial hypertension with no computed tomography (CT) features of lung disease; IPAH-LD: idiopathic pulmonary arterial hypertension with CT features of lung disease; IPAH-CGG: idiopathic pulmonary arterial hypertension with centrilobular ground-glass changes.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Baseline characteristics
Characteristic Full cohort Subgroups p-value IPAH PH-CLD Subjects n 660 335 325 Age at diagnosis years 64±15 60±17 67±11 <0.001 Male sex 318 (48) 131 (39) 187 (58) <0.001 WHO functional class 0.020 II 78 (12) 44 (13) 34 (10) III 398 (61) 213 (64) 185 (57) IV 181 (28) 76 (23) 105 (32) CT – centrilobular ground-glass (CGG) 54 (8.2) 54 (16) 0 (0) <0.001 CT – ground-glass opacification (GGO) 93 (14) 62 (19) 31 (9.5) <0.001 CT – honeycombing 15 (2.3) 5 (1.5) 10 (3.1) 0.2 CT – consolidation 31 (4.7) 9 (2.7) 22 (6.8) 0.013 CT – fibrosis 213 (32) 72 (21) 141 (43) <0.001 CT – fibrosis (by severity) <0.001 None 447 (68) 263 (79) 184 (57) Mild 82 (12) 54 (16) 28 (8.6) Moderate 53 (8.0) 9 (2.7) 44 (14) Severe 48 (7.3) 0 (0) 48 (15) Unknown 30 (4.5) 9 (2.7) 21 (6.5) CT – emphysema 302 (46) 98 (29) 204 (63) <0.001 CT – emphysema (by severity) <0.001 None 358 (54) 237 (71) 121 (37) Mild 77 (12) 48 (14) 29 (8.9) Moderate 129 (20) 38 (11) 91 (28) Severe 69 (10) 5 (1.5) 64 (20) Unknown 27 (4.1) 7 (2.1) 20 (6.2) CT – CPFE 101 (15) 32 (9.6) 69 (21) <0.001 mPAP mmHg 47±13 53±12 42±10 <0.001 mRAP mmHg 10.2±5.6 11.4±5.8 9.0±5.1 <0.001 PAWP mmHg 11.3±3.8 10.8±3.3 11.8±4.2 0.002 Cardiac output L·min−1 4.65±1.66 4.31±1.62 5.00±1.64 <0.001 Cardiac index L·min−1·m−2 2.53±0.87 2.32±0.81 2.73±0.87 <0.001 PVR Wood Units 9.0±5.1 11.0±5.2 7.0±4.1 <0.001 SvO2% 63±9 61±9 65±8 <0.001 FEV1 % predicted 72±25 83±18 60±25 <0.001 FEV1 severity <0.001 Normal (>80% predicted) 259 (41) 187 (58) 72 (24) Mild (70–80% predicted) 87 (14) 53 (17) 34 (11) Moderate (50–70% predicted) 139 (22) 70 (22) 69 (23) Severe (<50% predicted) 140 (22) 11 (3.4) 129 (42) FEV1/FVC % 66±15 71±10 61±18 <0.001 DLCO % predicted 37±19 44±20 28±14 <0.001 Data are presented as n (%) or mean±sd unless otherwise stated. IPAH: idiopathic pulmonary arterial hypertension; PH-CLD: PH due to chronic lung disease and/or hypoxia; CT: computed tomography; WHO: World Health Organisation; CPFE: combined pulmonary fibrosis and emphysema; mPAP: mean pulmonary arterial pressure; mRAP: mean right atrial pressure; PAWP: pulmonary arterial wedge pressure; PVR: pulmonary vascular resistance; SvO2: mixed venous oxygen saturation; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; DLCO: diffusing capacity of the lung for carbon monoxide.
- TABLE 2
Univariate analysis of the overall study cohort
Full cohort# IPAH¶ PH-CLD+ Characteristic HR 95% CI p-value HR 95% CI p-value HR 95% CI p-value CT – centrilobular ground-glass (CGG) 0.29 0.17–0.50 <0.001 0.44 0.25–0.78 0.005 CT – ground-glass opacification (GGO) 0.53 0.38–0.74 <0.001 0.52 0.32–0.86 0.010 0.72 0.46–1.14 0.2 CT – honeycombing 2.79 1.57–4.99 <0.001 3.72 1.37–10.1 0.010 2.11 1.04–4.30 0.039 CT – consolidation 0.84 0.50–1.40 0.5 1.10 0.45–2.68 0.8 0.60 0.32–1.13 0.11 CT – fibrosis 2.38 1.94–2.91 <0.001 2.48 1.76–3.50 <0.001 1.83 1.42–2.35 <0.001 CT – fibrosis (any present, ref: none) None — — — — — — Mild 1.94 1.46–2.58 <0.001 2.51 1.72–3.66 <0.001 1.73 1.11–2.71 0.016 Moderate 2.77 1.99–3.85 <0.001 4.53 2.07–9.92 <0.001 1.71 1.18–2.48 0.005 Severe 3.19 2.30–4.43 <0.001 1.98 1.40–2.80 <0.001 CT – emphysema 2.09 1.71–2.56 <0.001 2.74 1.96–3.81 <0.001 1.13 0.87–1.47 0.4 CT – emphysema (any present, ref: none) None — — — — — — Mild 1.78 1.30–2.43 <0.001 2.90 1.89–4.46 <0.001 0.89 0.56–1.42 0.6 Moderate 2.18 1.69–2.81 <0.001 3.16 2.01–4.97 <0.001 1.13 0.82–1.55 0.5 Severe 2.92 2.15–3.97 <0.001 11.1 3.92–31.6 <0.001 1.37 0.97–1.93 0.075 CT – CPFE 2.20 1.72–2.80 <0.001 2.09 1.33–3.29 0.001 1.82 1.36–2.44 <0.001 Age at diagnosis years 1.05 1.04–1.05 <0.001 1.06 1.05–1.08 <0.001 1.02 1.01–1.04 <0.001 Male sex 1.66 1.36–2.03 <0.001 1.59 1.16–2.18 0.004 1.42 1.10–1.83 0.007 WHO functional class III and IV (ref: I and II) 1.78 1.45–2.18 <0.001 1.88 1.34–2.64 <0.001 1.74 1.35–2.25 <0.001 WHO functional class II — — — — — — III 2.57 1.70–3.89 <0.001 3.00 1.51–5.96 0.002 2.45 1.46–4.13 <0.001 IV 5.08 3.31–7.79 <0.001 5.49 2.69–11.2 <0.001 4.80 2.81–8.21 <0.001 mPAP mmHg 0.99 0.98–1.00 0.028 0.98 0.97–0.99 0.006 1.04 1.03–1.05 <0.001 mRAP mmHg 1.01 0.99–1.03 0.4 1.03 1.00–1.06 0.023 1.03 1.00–1.05 0.057 PAWP mmHg 1.02 0.99–1.04 0.3 1.03 0.98–1.09 0.2 0.98 0.95–1.01 0.2 Cardiac output L·min−1 0.92 0.86–0.98 0.009 0.88 0.78–0.99 0.035 0.79 0.72–0.86 <0.001 Cardiac index L·min−1·m−2 0.87 0.76–0.98 0.028 0.80 0.63–1.01 0.063 0.61 0.51–0.74 <0.001 PVR (Wood Units) 1.04 1.00–1.08 0.036 0.98 0.91–1.05 0.5 1.10 1.05–1.16 <0.001 SvO2% 0.98 0.97–0.99 0.001 0.97 0.95–0.98 <0.001 0.96 0.94–0.97 <0.001 FEV1 % predicted 1.00 0.99–1.00 0.032 0.99 0.98–1.00 0.11 1.01 1.01–1.02 <0.001 FVC % predicted 1.00 0.99–1.00 0.028 1.00 0.99–1.01 0.9 1.00 1.00–1.01 0.4 FEV1/FVC ratio 0.99 0.99–1.00 0.038 0.97 0.95–0.98 <0.001 1.02 1.01–1.03 <0.001 DLCO % predicted 0.95 0.95–0.96 <0.001 0.95 0.94–0.96 <0.001 0.96 0.95–0.97 <0.001 Bold text: meets statistical significance. IPAH: idiopathic pulmonary arterial hypertension; PH-CLD: PH due to chronic lung disease and/or hypoxia; HR: hazard ratio; CI: confidence interval; CT: computed tomography; WHO: World Health Organisation; CPFE: combined pulmonary fibrosis and emphysema; mPAP: mean pulmonary arterial pressure; mRAP: mean right atrial pressure; PAWP: pulmonary arterial wedge pressure; PVR: pulmonary vascular resistance; SvO2: mixed venous oxygen saturation; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; DLCO: diffusing capacity of the lung for carbon monoxide. #: n=660; ¶: n=335; +: n=325.
- TABLE 3
Multivariate analysis
Characteristic Univariate Multivariate 1 (adjusted for demographics – age, sex, WHO FC) Multivariate 2 (adjusted for demographics and mPAP) Multivariate 3 (adjusted for demographics, mPAP and DLCO) HR 95% CI p-value HR 95% CI p-value HR 95% CI p-value HR 95% CI p-value Full cohort (n=660) CT – centrilobular ground-glass (CGG) 0.29 0.17–0.50 <0.001 0.50 0.28–0.89 0.010 0.48 0.26–0.86 0.007 0.76 0.39–1.47 0.4 CT – ground-glass opacification (GGO) 0.53 0.38–0.74 <0.001 0.82 0.58–1.16 0.2 0.84 0.60–1.19 0.3 0.80 0.54–1.18 0.2 CT – honeycombing 2.79 1.57–4.99 <0.001 1.73 0.97–3.11 0.087 1.74 0.97–3.12 0.086 1.10 0.54–2.24 0.8 CT – emphysema 2.09 1.71–2.56 <0.001 1.48 1.21–1.83 <0.001 1.52 1.23–1.88 <0.001 1.13 0.89–1.44 0.3 CT – fibrosis 2.38 1.94–2.91 <0.001 1.75 1.42–2.15 <0.001 1.77 1.43–2.18 <0.001 1.37 1.09–1.73 0.008 IPAH (n=335) CT – centrilobular ground-glass (CGG) 0.44 0.25–0.78 0.005 0.79 0.43–1.45 0.4 0.80 0.43–1.48 0.5 0.92 0.47–1.82 0.8 CT – ground-glass opacification (GGO) 0.52 0.32–0.86 0.010 0.88 0.52–1.47 0.6 0.91 0.54–1.52 0.7 0.96 0.55–1.69 0.9 CT – honeycombing 3.72 1.37–10.1 0.010 1.69 0.61–4.65 0.3 1.68 0.61–4.62 0.4 1.35 0.49–3.74 0.6 CT – emphysema 2.74 1.96–3.81 <0.001 1.72 1.22–2.42 0.002 1.76 1.24–2.49 0.002 1.26 0.85–1.86 0.2 CT – fibrosis 2.48 1.76–3.50 <0.001 1.42 0.99–2.02 0.060 1.44 1.00–2.07 0.056 1.23 0.84–1.81 0.3 PH-CLD (n= 325) CT – honeycombing 2.11 1.04–4.30 0.039 1.80 0.88–3.67 0.14 2.02 0.99–4.14 0.081 1.06 0.39–2.91 >0.9 CT – fibrosis 1.83 1.42–2.35 <0.001 1.73 1.34–2.24 <0.001 1.63 1.26–2.10 <0.001 1.46 1.09–1.96 0.011 Bold text: meets statistical significance. WHO FC: World Health Organization functional class; mPAP: mean pulmonary arterial pressure; DLCO: diffusing capacity of the lung for carbon monoxide; HR: hazard ratio; CI: confidence interval; CT: computed tomography; IPAH: idiopathic pulmonary arterial hypertension; PH-CLD: pulmonary hypertension associated with chronic lung disease.
- TABLE 4
Baseline characteristics of patients with initial diagnosis of IPAH
Characteristic IPAH-noLD IPAH-CGG IPAH-LD p-value Subjects n 151 46 130 Age at diagnosis 56±18# 48±19# 70±9¶,+ <0.001 Male sex 48 (32)# 11 (24)# 69 (53)¶,+ <0.001 WHO functional class # # ¶,+ 0.011 II 25 (17) 9 (20) 9 (6.9) III 98 (65) 29 (64) 81 (62) IV 27 (18) 7 (16) 40 (31) Smoker, ever 66 (49)# 19 (42)# 81 (86)¶,+ <0.001 CT – centrilobular ground-glass 0 (0)+ 46 (100)¶,# 0 (0)+ <0.001 CT – ground-glass opacification 9 (6.0)+ 39 (85)¶,# 8 (6.2)+ <0.001 CT – honeycombing 0 (0)# 0 (0)¶,# 5 (3.8)¶ 0.021 CT – consolidation 5 (3.3) 2 (4.3) 2 (1.5) 0.4 CT – fibrosis 0 (0)# 0 (0)# 68 (52)¶,+ <0.001 CT – fibrosis (by severity) # # ¶,+ <0.001 None 151 (100) 46 (100) 62 (48) Mild 0 (0) 0 (0) 52 (40) Moderate 0 (0) 0 (0) 9 (6.9) Unknown 0 (0) 0 (0) 7 (5.4) CT – emphysema 0 (0)# 0 (0)# 94 (72)¶,+ <0.001 CT – emphysema (by severity) # # ¶,+ None 151 (100) 46 (100) 36 (28) Mild 0 (0) 0 (0) 44 (34) Moderate 0 (0) 0 (0) 38 (29) Severe 0 (0) 0 (0) 5 (3.8) Unknown 0 (0) 0 (0) 7 (5.4) CT – CPFE 0 (0)# 0 (0)# 32 (25)¶,+ <0.001 mPAP mmHg 54±12+,# 62±13¶,# 49±8¶,+ <0.001 mRAP mmHg 12±6 10±5 11±5 0.3 PAWP mmHg 10.91±3.10 9.72±2.77 11.03±3.21 0.055 Cardiac output L·min−1 4.64±1.87+,# 3.85±0.98¶ 4.08±1.44¶ 0.014 Cardiac index L·min−1·m−2 2.47±0.95# 2.13±0.52 2.23±0.73¶ 0.031 PVR Wood Units 10.7±5.2+ 14.6±6.2¶,# 10.3±4.4+ <0.001 SvO2% 61±10 62±7 59±8 0.030 FEV1 % predicted 82±17 88±15 83±20 0.124 FEV1 severity 0.056 Normal (>80% predicted) 83 (58) 31 (70) 67 (53) Mild (70–80% predicted) 21 (15) 8 (18) 24 (19) Moderate (50–70% predicted) 34 (24) 5 (11) 29 (23) Severe (<50% predicted) 5 (3.5) 0 (0) 6 (4.8) FVC % predicted 93±20 101±18 99±21 0.016 FEV1/FVC % 74±10# 74±8# 67±10¶,+ <0.001 DLCO % predicted 52±20# 56±17# 31±14¶,+ <0.001 Data are presented as n (%) or mean±sd unless otherwise stated. Between-group comparisons performed using one-way ANOVA with Bonferroni post hoc correction. Eight patients with both CGG and LD not included. IPAH: idiopathic pulmonary arterial hypertension; IPAH-noLD: idiopathic pulmonary arterial hypertension with no computed tomography features of lung disease; IPAH-CGG: idiopathic pulmonary arterial hypertension with centrilobular ground-glass changes; IPAH-LD: idiopathic pulmonary arterial hypertension with CT features of lung disease; CT: computed tomography; WHO: World Health Organisation; CPFE: combined pulmonary fibrosis and emphysema; mPAP: mean pulmonary arterial pressure; mRAP: mean right atrial pressure; PAWP: pulmonary arterial wedge pressure; PVR: pulmonary vascular resistance; SvO2: mixed venous oxygen saturation; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; DLCO: diffusing capacity of the lung for carbon monoxide; CGG: centrilobular ground-glass; LD: lung disease. Difference between groups noted – #: significant difference to IPAH-LD; ¶: significant difference to IPAH-noLD; +: significant difference to IPAH-CGG.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00549-2021.SUPPLEMENT










