





Abstract
Rationale Chronic obstructive pulmonary disease (COPD) patients often report aggravated symptoms due to heat and cold, but few studies have formally evaluated this.
Methodology We followed 30 Boston-based former smokers with COPD for four non-consecutive 30-day periods over 12 months. Personal and outdoor temperature exposure were measured using portable and Boston-area outdoor stationary monitors. Participants recorded daily morning lung function measurements as well as any worsening breathing (breathlessness, chest tightness, wheeze) and bronchitis symptoms (cough, sputum colour and amount) compared to baseline. Using linear and generalised linear mixed-effects models, we assessed associations between personal and outdoor temperature exposure (1–3-day moving averages) and lung function and symptoms, adjusting for humidity, smoking pack-years and demographics. We also stratified by warm and cold season.
Results Participants were on average 71.1±8.4 years old, with 54.4±30.7 pack-years of smoking. Each 5°C increase in personal temperature exposure was associated with 1.85 (95% CI 0.99–3.48) higher odds of worsening breathing symptoms. In the warm season, each 5°C increase in personal and outdoor temperature exposure was associated with 3.20 (95% CI 1.05–9.72) and 2.22 (95% CI 1.41–3.48) higher odds of worsening breathing symptoms, respectively. Each 5°C decrease in outdoor temperature was associated with 1.25 (95% CI 1.04–1.51) higher odds of worsening bronchitis symptoms. There were no associations between temperature and lung function.
Conclusions Our findings suggest that higher temperature, including outdoor exposure during the warm season and personal temperature exposure year-round, may worsen dyspnoea, while colder outdoor temperature may trigger cough and phlegm symptoms among COPD patients.
Abstract
Higher temperature, including outdoor exposure during the warm season and personal exposure year-round, may worsen dyspnoea while colder outdoor temperature may trigger cough and phlegm symptoms in COPD patients https://bit.ly/3G0bL2c
Background
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death in the world, with global burden and mortality expected to continue rising in the coming decades [1]. Symptoms of COPD include chronic cough, production of phlegm (mucus) and dyspnoea [2]. The disease course often involves a progressive, inexorable functional decline with acute episodes of exacerbation [3].
Increasing attention is being given to the effects of weather exposure in the context of climate change [4]. Extremes of temperature such as heat waves, hot weather and extended periods of cold may negatively affect lung function and symptom burden in COPD. In fact, COPD patients often report susceptibility to temperature and weather changes [5–8]. Both summer heat [5, 6, 8] and winter cold [7, 9, 10] have been associated with increased COPD hospitalisations and symptom burden. For example, McCormack et al. [6] found that higher maximal indoor temperature during the warm season in Baltimore was associated with worsened breathlessness, cough and sputum, and increased rescue inhaler use among COPD patients. Similarly, McCormack et al. [7] found that colder temperatures in the cold season were associated with respiratory symptoms and lower lung function.
Few studies have evaluated whether temperature affects individual-level COPD morbidity indictors, including daily changes in respiratory symptoms and lung function, that may precede healthcare utilisation for COPD [6, 7]. Most studies have relied on community-level monitors or brief sampling periods to estimate exposure to temperature, which may not capture personal exposure to temperature, especially among COPD patients who spend most of their time at home. New methods, using portable monitors that patients bring along during their indoor and outdoor activities, allow for daily evaluation of personal exposure to temperature [11]. This study examines how daily personal and outdoor temperature exposure in the warm (May–September) and cold (October–April) seasons affect daily lung function, breathing and bronchitis symptoms among community-dwelling COPD patients, using both portable and stationary monitors in the greater Boston area.
Materials and methods
Study population
The study population included 30 former smokers with COPD who were recruited as part of the Study of Air Pollution and COPD Exacerbation (SPACE) at the Beth Israel Deaconess Medical Center (Boston, MA, USA). This study was conducted in accordance with the Declaration of Helsinki and was approved by the Committee on Clinical Investigations at Beth Israel Deaconess Medical Center (IRB protocol number: 2015P000336/06). To be eligible, study participants were required to 1) have a home address within 50 km of the Harvard Supersite air pollution and temperature monitor at Harvard Medical School in Boston and 2) have a clinical diagnosis of COPD with at least moderate (Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage 2) airflow obstruction, defined as forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio of <0.70 and FEV1<80% predicted, using the Third National Health and Nutrition Examination Survey (NHANES III) prediction formulas [12]. Participants with a history of lung cancer, interstitial lung disease or bronchiectasis were ineligible to participate.
Data collection
Participants entered the study between February 24, 2017, and January 17, 2019. At study entry, demographic information, height, weight, past medical history, medication history and baseline measures of lung function were obtained, and participants were instructed on how to use a portable spirometer and personal air quality monitor (PAM). Participants were then observed for up to four non-consecutive 30-day periods in four different seasons over 12 months. Participants measured their lung function daily in the morning before taking any medications, using a portable EasyOne Plus Diagnostic Spirometer (NDD Medical Technologies, Zurich). This device meets American Thoracic Society guidelines and has built-in quality assurance and incentive software. At the end of follow-up, the 30 participants had contributed a total of 3314 observation-days.
Exposure assessment
We measured personal daily exposure to temperature and relative humidity using the portable PAMs, and outdoor exposure using the temperature and relative humidity monitor on the rooftop of Countway Library, Harvard Medical School (Boston, MA, USA). The PAMs were developed by Atmospheric Sensors Ltd (model 520) and were equipped with sensors for temperature and relative humidity. All exposure measures from the PAMs were calibrated to stationary monitors in the Boston area. During repeated calibration periods in different seasons, 24-h averages of temperature and relative humidity from a reference PAM were compared to a state-owned stationary monitor in Boston using linear regression models. Mean adjusted R [2] was 0.8 for temperature and 0.9 for relative humidity. Daily personal exposure to air pollutants, including fine particulate matter (particles with a 50% cut-off aerodynamic diameter of 2.5 µm (PM2.5)), nitrogen dioxide (NO2) and ozone (O3), was also measured by the PAMs, as previously described [13]. Additional information about the PAM technology, reproducibility of pollutant measurements and agreement with stationary monitors in diverse settings has been published by other investigators [14, 15]. Outdoor exposure to pollutants was measured using state-owned stationary monitors in Boston, as previously described [13]. Finally, we evaluated if associations between temperature and COPD-related symptoms departed from linearity.
Statistical analysis
We calculated mean previous-day 24-h exposure to temperature from the PAMs (personal exposure) and outdoor state-owned stationary monitors in the Boston area (outdoor exposure).
We constructed multilevel linear mixed-effects models to assess associations between 1-, 2- and 3-day 24-hour exposure to personal and outdoor temperature and lung function (FEV1 and FVC) as follows: where Yimt is any continuous indicator of lung function for participant i at observation month m on day t; tempimt indicates personal or outdoor temperature exposure average and cimt represents a vector of potential confounders (personal or outdoor exposure to relative humidity, age, sex, race, height, weight, total pack-year smoking history, education and season). Season was categorised as winter, spring, summer or autumn based on the calendar start dates of each observation month. The term wi denotes a participant-specific random effect and was used to account for intra-individual correlations between repeated measurements from the same person, vim denotes a participant observation month-specific random effect that allows daily observations from a single observation month within the same person to be more highly correlated than observations from a different observation month on the same person. The residuals eimt are normally distributed errors, assumed to follow an autoregressive (AR(1)) process, modelling the serial correlation among the daily time series within the same person's observation month.
where Yimt is any continuous indicator of lung function for participant i at observation month m on day t; tempimt indicates personal or outdoor temperature exposure average and cimt represents a vector of potential confounders (personal or outdoor exposure to relative humidity, age, sex, race, height, weight, total pack-year smoking history, education and season). Season was categorised as winter, spring, summer or autumn based on the calendar start dates of each observation month. The term wi denotes a participant-specific random effect and was used to account for intra-individual correlations between repeated measurements from the same person, vim denotes a participant observation month-specific random effect that allows daily observations from a single observation month within the same person to be more highly correlated than observations from a different observation month on the same person. The residuals eimt are normally distributed errors, assumed to follow an autoregressive (AR(1)) process, modelling the serial correlation among the daily time series within the same person's observation month.
For binary symptom outcomes, we constructed similar generalised logistic mixed-effects models using the PROC GLIMMIX function in SAS (SAS Institute, Cary, NC, USA) with a participant observation month-specific random effect to assess for associations between exposure to personal and outdoor temperature and odds of worsening breathing symptoms (breathlessness, chest tightness, wheeze) [16] and bronchitis symptoms (cough, sputum colour and sputum amount) [17].
To evaluate differential effects of heat and cold, we ran all models using stratum-specific associations for warm (May–September) and cold (October–April) seasons. This distinction is relevant for the Boston area and aligns with cold and warm seasons defined in previous research [18]. When assessing the association between exposure to temperature (personal or outdoor) and morning lung function and symptom outcomes, in separate models we examined temperature based on previous 1-, 2- and 3-day moving averages of temperature.
To test if any associations were explained by differences in exposure to pollutants, we performed sensitivity analyses additionally adjusting all previous-day (1-day moving average) temperature models for previous-day PM2.5, NO2 and O3 in separate models. For this analysis, we adjusted for individual personal pollutant exposure when examining personal temperature exposure, and outdoor pollutant exposure when examining outdoor temperature exposure and associations with lung function and symptoms.
Using generalised additive mixed models with a binomial distribution, we plotted penalised splines to evaluate the shape of the associations of personal and outdoor temperature exposure with COPD-related symptoms, including data for all seasons.
All statistical analyses were performed using SAS 9.4 (SAS Institute), and spline plots were produced using R v3.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of study participants
We collected 3314 observations from 30 participants. Baseline participant characteristics are summarised in table 1. Participants had an average age of 71.1±8.4 years, were predominantly white (80.0%) and there were slightly more female participants (53.3%). Most had some level of college education or associate degree or higher (73.3%) and had on average 54.4±30.7 pack-years of smoking. There was also a near even distribution of participants across the income categories.
Baseline characteristics of study participants (n=30)
The mean±sd personal temperature exposure was 21.5±2.2°C for all seasons, 20.8±2.1°C for the cold season (October–April) and 22.3±2.0°C for the warm season (May–September). The mean±sd outdoor temperature was 12.0±9.6°C for all seasons, 5.6±7.1°C for the cold season and 20.3±5.2°C for the warm season. Figure 1 shows the mean daily temperature per month as measured by personal and outdoor community-level monitors.

Distribution of daily personal and outdoor temperature exposure per month.
Temperature exposure and lung function
Using linear mixed-effects models, we found no associations between 1-, 2- and 3-day moving average personal and outdoor temperature exposure and morning lung function (FEV1 and FVC) across all seasons, nor for the cold or warm seasons (supplementary table S1).
Temperature exposure and breathing symptoms
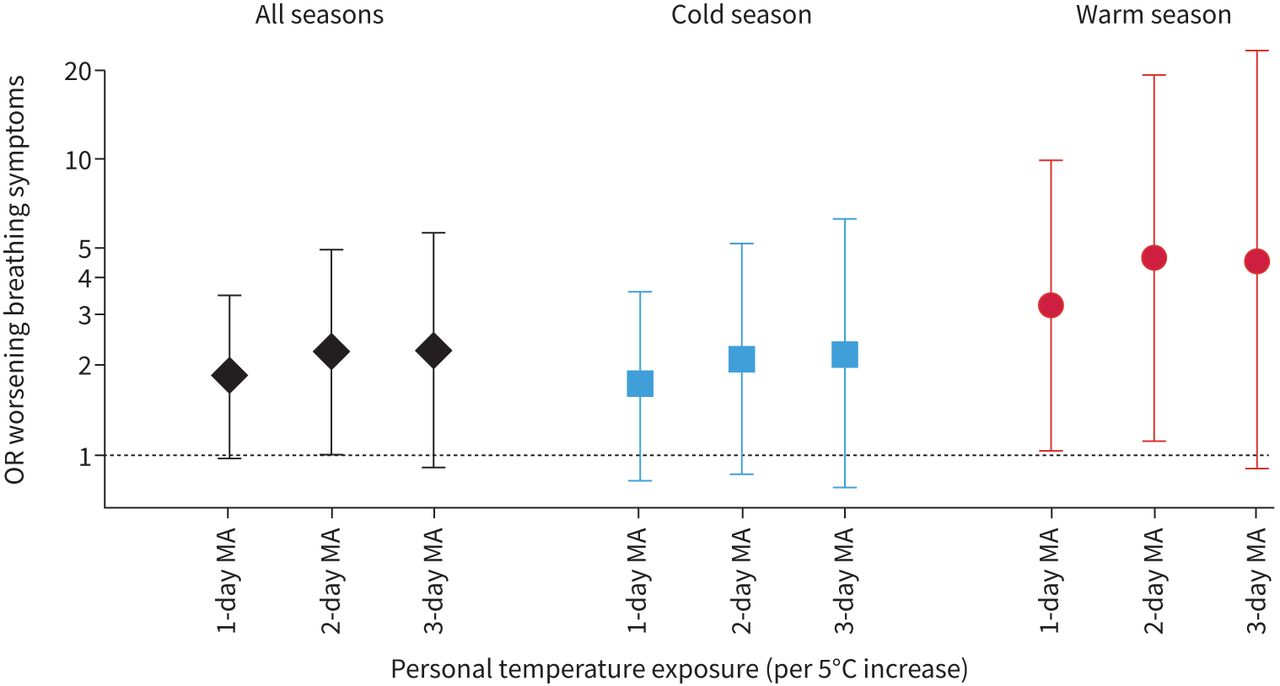
Higher temperature exposure measured by the personal monitor was associated with higher odds of worsened breathing symptoms (figure 2). For example, in fully adjusted mixed-effects models, each 5°C higher previous-day personal exposure to temperature was associated with a 1.85 (95% CI 0.99–3.48, p=0.055) higher odds of worsening breathing symptoms overall. These results were similar for 2-day (OR 2.23, 95% CI 1.01–4.89, p=0.046) and 3-day (OR 2.26, 95% CI 0.91–5.58, p=0.078) moving averages of temperature. We also found positive associations between each 5°C higher 1-day moving average personal temperature exposure and odds of worsening breathing symptoms in the warm season (OR 3.20, 95% CI 1.05–9.72, p=0.040), with similar results for 2-day (OR 4.61, 95% CI 1.12–18.94, p=0.034) and 3-day (OR 4.56, 95% CI 0.91–22.81, p=0.065) moving averages of temperature. We found no associations between personal exposure to temperature and breathing symptoms within the cold season.

Association between personal temperature exposure and breathing symptoms (per 5°C temperature increase). Mixed-model analysis showing odds ratios (ORs) for worsening breathing symptoms per 5°C higher personal temperature exposure, adjusted for previous-day humidity, age, sex, height, weight, total pack-years of smoking and education. Cold season: October–April; warm season: May–September. MA: moving average.
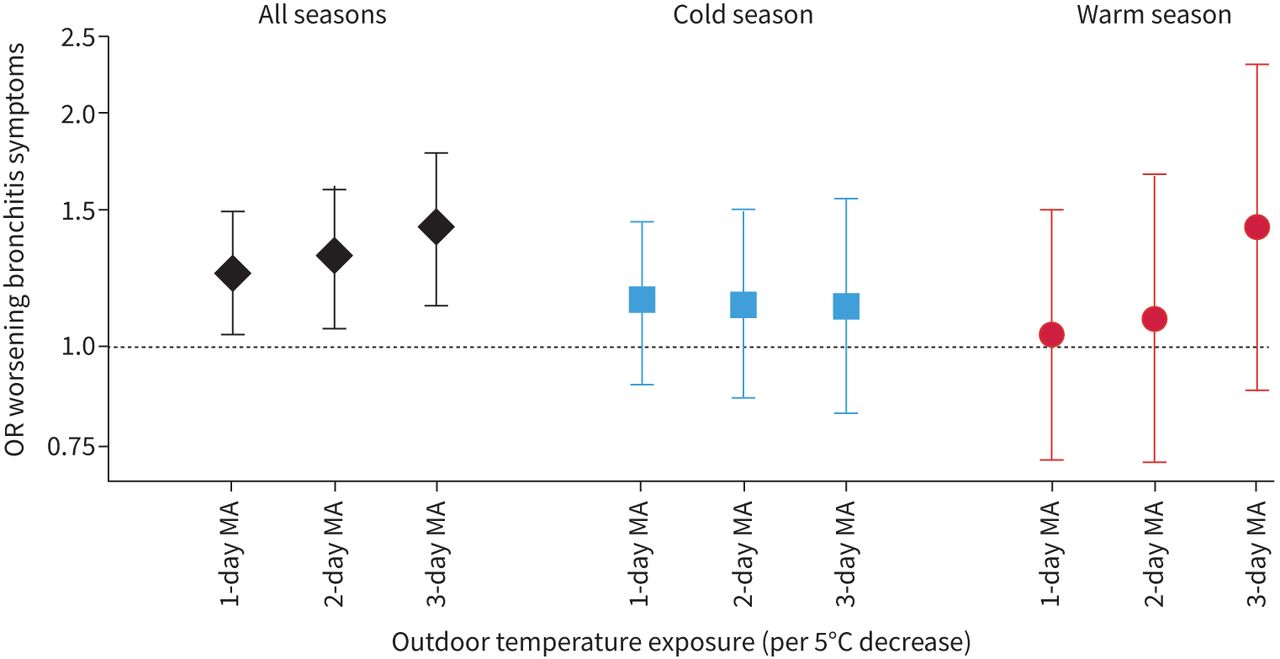
Higher outdoor temperature exposure was associated with worsened breathing symptoms in the warm season (figure 3). Each 5°C higher previous-day outdoor temperature was associated with a 2.22 (95% CI 1.41–3.48, p=0.001) higher odds of worsening breathing symptoms in the warm season. These results were similar for 2-day (OR 2.50, 95% CI 1.47–4.24, p=0.001) and 3-day (OR 2.53, 95% CI 1.40–4.55, p=0.002) moving averages of outdoor temperature exposure in the warm season. Outdoor temperature exposure was not associated with worsening breathing symptoms overall, or in the cold season specifically.

Association between outdoor temperature exposure and breathing symptoms (per 5°C higher temperature). Mixed-model analysis showing odds ratios (ORs) for worsening breathing symptoms per 5°C higher outdoor temperature exposure, adjusted for previous-day humidity, age, sex, height, weight, total pack-years of smoking and education. Cold season: October–April; warm season: May–September. MA: moving average.
Temperature exposure and bronchitis symptoms
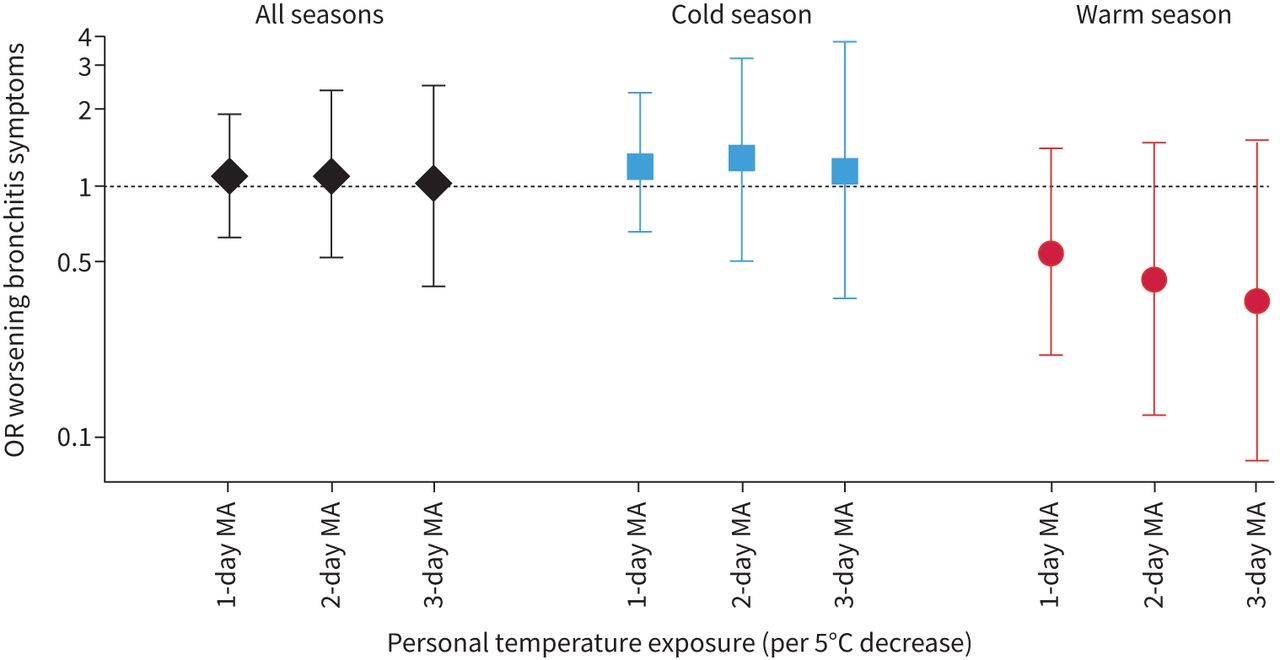
Personal exposure to temperature was not associated with worsening bronchitis symptoms overall, nor for season-stratified models (figure 4).

Association between personal temperature exposure and bronchitis symptoms (per 5°C lower temperature). Mixed-model analysis showing odds ratios (ORs) for worsening bronchitis symptoms per 5°C lower personal temperature exposure, adjusted for previous-day humidity, age, sex, height, weight, total pack-years of smoking and education. Cold season: October–April; warm season: May–September. MA: moving average.
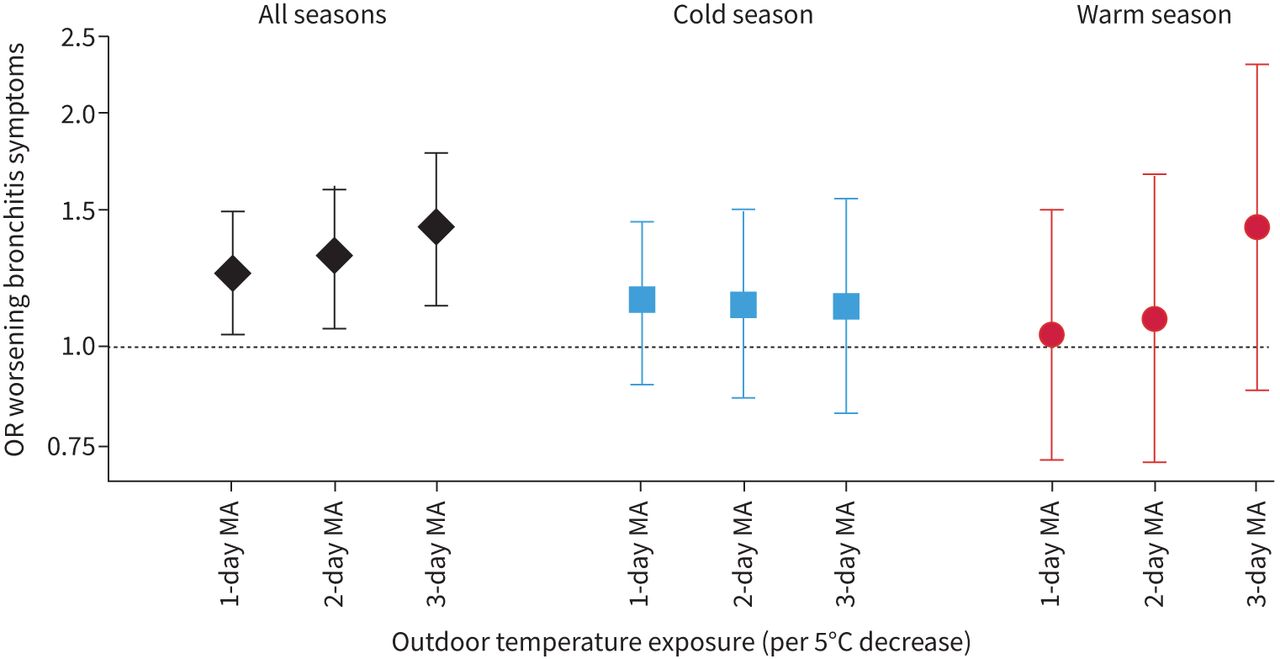
Lower outdoor temperature exposure was associated with worsening bronchitis symptoms. In fully adjusted models, each 5°C lower previous-day outdoor temperature exposure was associated with a 1.25 (95% CI 1.04–1.51, p=0.016) higher odds of worsening bronchitis symptoms, with similar associations for 2-day (OR 1.30, 95% CI 1.06–1.60, p=0.014) and 3-day (OR 1.42, 95% CI 1.13–1.78, p=0.003) moving averages. We found no associations between outdoor temperature exposure and bronchitis symptoms in season-stratified models (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between outdoor temperature exposure and bronchitis symptoms (per 5°C lower temperature). Mixed-model analysis showing odds ratios (ORs) for worsening bronchitis symptoms per 5°C lower outdoor temperature exposure, adjusted for previous-day humidity, age, sex, height, weight, total pack-years of smoking and education. Cold season: October–April; warm season: May–September. MA: moving average.
Secondary analyses
In secondary analyses, we did not find that any associations between temperature exposure and symptoms were explained or confounded by personal or outdoor pollutant exposures. In models examining associations between previous-day personal and outdoor temperature exposure and lung function, breathing and bronchitis symptoms, additional adjustment for personal or outdoor PM2.5, NO2 or O3 exposure did not change any of the associations between temperature exposure and these outcomes (supplementary tables S2–S5).
Penalised spline plots demonstrated linear-shaped associations between previous-day personal temperature exposure and breathing symptoms, and between previous-day personal and outdoor temperature exposure and bronchitis symptoms. However, the association between outdoor temperature exposure and breathing symptoms showed a non-linear, U-shaped relationship, in which extremes of both warmer and colder outdoor temperature exposure were associated with higher odds of breathing symptoms (supplementary figure S1). Splines for cold and warm season followed similar patterns as those for all seasons (data not shown).
Discussion
In this prospective study of people with moderate-to-severe COPD residing in the Boston area, higher personal and outdoor temperature exposure was associated with worsened breathing symptoms (i.e. breathlessness, wheeze and tightness of the chest), especially in the warm (May–September) season. By contrast, lower outdoor temperature exposure was associated with worsening bronchitis symptoms (cough, sputum colour and sputum amount), regardless of season. We found no associations between temperature exposure and morning lung function. Associations with temperature were not explained by differences in exposure to air pollutants.
Our findings are consistent with a growing number of studies reporting adverse health effects of indoor and outdoor heat in the warm season in older patients with COPD [6, 19]. For example, longitudinal individual-level exposure and symptom assessment data in a Baltimore-based cohort of COPD patients demonstrated that a 10°F (5.5°C) increase in daily maximum indoor home temperature was associated with a worsening of symptoms based on average Breathlessness, Cough and Sputum Scale score as well as increased inhaler use in the warmer months [6]. A New York City-based study [20] on COPD morbidity using hospitalisation data found that the same-day risk of COPD hospitalisation increased by 7.6% for every 1°C increase above a threshold temperature of 29.8°C, and that there was a detectable but smaller association between temperature and respiratory hospitalisation when applying a 1-day lag.
We found that higher personal heat exposure was associated with breathlessness, but not lung function, regardless of season. This may indicate that worsened breathing symptoms are not a result of a bronchoconstrictive effect of heat but, rather, a thermoregulatory response in which the metabolic demands of cooling the body in the setting of fixed airflow limitation results in exertional dyspnoea [8]. Our findings suggest that heat can result in a greater burden of breathing symptoms in COPD patients, whether it is due to hot weather or other sources of (indoor) heat. In the cold season, we found associations for breathlessness with personal heat exposure but not with outdoor temperature exposure, suggesting that higher temperatures from indoor heating sources during the cold season have an adverse effect on breathing symptoms. Our findings suggest an opportunity for clinical, housing and policy measures to prevent exposure to high temperatures among patients with COPD, both during warm and cold seasons.
Although the results of our primary (linear) models demonstrated that higher outdoor temperature exposure was associated with worsened breathing symptoms in the warm season only, in secondary analyses we evaluated non-linear relationships and found that both extremes of outdoor temperature (not only very warm but also very cold) were associated with a higher odds of worsening breathing symptoms [7]. Interestingly, for personal temperature exposure, we found that only higher temperatures were associated with greater odds of breathing symptoms in a linear fashion across the range of exposures. A potential explanation could be that during periods of extremely cold weather, our participants spent most of their time indoors (reflected in the much narrower range of recorded personal temperatures throughout the year, averaged over 24-h periods, compared to outdoor temperatures). These results may suggest that even brief exposure to outdoor cold temperatures may cause dyspnoea in the COPD population who spend most of their time indoors in a temperature-controlled environment [7]. Our finding that colder outdoor temperature was associated with bronchitis symptoms is consistent with epidemiological studies finding adverse health effects of cold weather, such as risk of acute bronchitis and exacerbations of asthma and COPD [7, 21]. One of the few studies to evaluate associations of colder temperature with daily subclinical measures reported that during the winter season colder outdoor temperatures were associated with increased respiratory symptoms (measured by the Breathlessness, Sputum and Cough scale), increased rescue inhaler use and decreased lung function in former smokers with COPD [7]. We found an effect of colder temperature on bronchitis symptoms (cough, sputum colour and sputum amount), while we found the opposite for breathing symptoms. This may indicate mucous hypersecretion as a potential mediator of the response to cold temperature in COPD [22]. Despite evidence that colder temperatures can trigger bronchoconstriction in COPD [23, 24], we did not find any associations between personal or outdoor cold temperature exposure and lung function in this study, even within the cold season. The reasons for the lack of association are unclear. Our findings suggest that COPD patients experience changes in bronchitis symptoms in association with temperature in the absence of lung function change [16, 25].
Our study has several limitations. Because our study population consists of former smokers with COPD living in an urban environment, our findings may not be generalisable to current smokers or those living in other settings. While we collected a large number of repeated measures (up to 120 observation-days per participant and 3314 observation-days in total), our study only included 30 unique individuals in the Boston area, which limits the generalisability of our findings to other populations with COPD, such as those with milder disease or those living in other climates. We also did not account for characteristics of participant's homes and behaviours, such as types of insulation used in the home, heating sources or window-opening behaviour of people living in the home, which may influence participant's personal exposure to temperature. Future research may assess how such factors influence personal temperature exposure, and whether there are health benefits of interventions to reduce exposure to heat and cold in this population.
Our study also has several strengths. Our unique longitudinal study design with daily exposure and health measures allowed us to evaluate how day-to-day variability in personal and outdoor temperature exposure relate to daily lung function, breathing symptoms and bronchitis symptoms in an older population with COPD, while accounting for within-person correlation of measurements, and adjusting for a robust list of potential individual-level and seasonal confounders. We used lightweight portable exposure monitors, calibrated to gold standard stationary monitors, to measure exposure at the individual level for a prolonged period (a total of 4 months) across different seasons. Our findings suggest the value of measuring personal temperature exposure in this population, because we found that personal temperature exposure was associated with both breathing and bronchitis symptoms.
Conclusion
Our findings suggest that exposure to higher temperature year-round may worsen breathing symptoms, especially in the warm season, and exposure to colder temperatures independent of season may trigger cough and phlegm symptoms among COPD patients, without affecting lung function. These findings suggest an opportunity to address personal exposure to warmer temperature as a risk factor for aggravated dyspnoea in the warmer months, and outdoor colder temperatures as a risk factor for increased bronchitis symptoms in COPD throughout the year.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00574-2021.supplement
Footnotes
Provenance: Submitted article, peer reviewed.
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: C. Scheerens declares a stipend from the Belgian American Educational Foundation and a project grant from the Strategic International Partnership Ghent University–Harvard University, in the 36 months prior to manuscript submission. L. Nurhussien reports that the current work was supported by the National Institutes of Environmental Health Sciences (NIEHS) (K23ES026204, R01ES031252 and P30ES000002) and by the US Environmental Protection Agency (grant RD-835872). B.A. Coull declares National Institutes of Health grant funding to their institution for the present work. M.B. Rice reports grants from the NIEHS (K23 ES026204 and P30 ES000002) in support of the present work; grants U01 HL 146408 and R01 ES 031252 in the 36 months prior to manuscript submission, unconnected to the present work; a personal honorarium from USC for serving as visiting professor for their NIEHS Center; and payment to them from the Conservation Law Foundation for providing an expert opinion, also within the 36 months prior to manuscript submission. She also reports that she was Leader of the American Thoracic Society (ATS) Environmental Health Policy Committee until May 2020 and is Program Committee chair-elect for the EOPH assembly of ATS. The other authors have nothing to disclose.
Support statement: This work was supported by the National Institutes of Environmental Health Sciences (K23ES026204, R01ES031252 and P30ES000002), the National Heart, Lung, and Blood Institute (F32 HL143819), the US Environmental Protection Agency (USEPA) (grant RD-835872), the Belgian American Educational Foundation and Ghent University. Its contents are solely the responsibility of the grantee and do not necessarily represent the official views of the USEPA. Further, USEPA does not endorse the purchase of any commercial products or services mentioned in the publication. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received October 4, 2021.
- Accepted December 28, 2021.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










