





Abstract
Background Cough symptom severity represents an important subjective end-point to assess the impact of therapies for patients with refractory or unexplained chronic cough (RCC/UCC). As existing instruments assessing the severity of cough are neither widely available nor tested for measurement properties, we aim to develop a new patient-reported outcome measure addressing cough severity.
Objective The aim of this study was to establish items and domains that would inform development of a new cough severity instrument.
Methods Three focus groups involving 16 adult patients with RCC/UCC provided data that we analysed using directed content analysis. Discussions led to consensus among an international panel of 15 experts on candidate items and domains to assess cough severity.
Results The patient focus group provided 48 unique items arranged under broad domains of urge-to-cough sensations and cough symptom. Feedback from expert panel members confirmed the appropriateness of items and domains, and provided an additional subdomain related to cough triggers. The final conceptual framework comprised 51 items in the following domains: urge-to-cough sensations (subdomains: frequency and intensity) and cough symptom (subdomains: triggers, control, frequency, fit/bout duration, intensity, quality and associated features/sequelae).
Conclusions Consensus findings from patients and international experts established domains of urge-to-cough and cough symptom with associated subdomains and relevant items. The results support item generation and content validity for a novel patient-reported outcome measure for use in health research and clinical practice.
Abstract
The urge-to-cough (subdomains: frequency and intensity) and cough symptom (subdomains: triggers, control, frequency, fit/bout duration, intensity, quality, and associated features/sequelae) represent domains to assess cough severity in RCC/UCC https://bit.ly/3fI6qkC
Introduction
Chronic cough lasting >8 weeks is a common health problem that affects 2–18% of adults worldwide [1]. Although clinicians can often identify and effectively treat known causes of cough—including asthma, COPD, bronchiectasis, gastro-oesophageal reflux disease and upper airway cough syndromes—many patients, despite treatment targeting these underlying conditions, experience refractory chronic cough (RCC) [2, 3]. In others, clinical assessment fails to identify a cause, and patients are classified with unexplained chronic cough (UCC) [2, 3]. Patients with RCC/UCC often exhibit cough hypersensitivity syndrome, defined as a troublesome cough triggered by low levels of thermal, mechanical or chemical irritants [4].
RCC/UCC can lead to significant impairment in quality of life (QoL); thus, QoL serves as an important end-point in establishing treatment impact. Cough-specific QoL measures, including the Leicester Cough Questionnaire [5], Cough Quality of Life Questionnaire [6] and Chronic Cough Impact Questionnaire [7], address the impact of cough symptoms on patients’ physical, social and psychological health. Such assessments, although crucial in addressing treatment impact, are limited in that they capture domains influenced by factors aside from cough symptom severity (i.e. psychosocial context). The same degree of cough in two patients can thus lead to substantially different responses regarding cough QoL. Neuromodulatory agents, such as pregabalin [8] and experimental neurokinin receptor antagonists [9], can improve cough QoL independent of cough suppression. Thus, full insight into therapeutic efficacy must, alongside cough QoL, include assessment of cough symptom severity.
Objective cough frequency using the VitaloJAK monitor represents the most common primary end-point in antitussive clinical trials [10]. Cough monitors provide direct insight into whether treatment improves cough frequency by quantifying spontaneous coughs over a defined period. Existing monitors are limited, however, in that they are typically only used over a 24-h period, they can pose a burden for patients to wear repeatedly and they are expensive to administer [11]. Furthermore, they cannot assess whether other dimensions of cough (i.e. intensity) may be improved with treatment. A measure that directly assesses patients’ experience of cough and sequelae (herein referred to as “symptom severity”) might address the limitations of currently available instruments.
The visual analogue scale (VAS) [12] and Cough Severity Diary (CSD) [13] represent existing instruments to assess cough severity. Limitations of the cough severity VAS include lack of evidence supporting its measurement properties and limitations of single-item instruments in fully capturing complex patient experiences [14]. While the CSD has undergone psychometric testing [15], it is currently a proprietary questionnaire with restrictions on use for clinical and research purposes. Furthermore, the CSD lacks conceptual clarity in that the domain “disruption” measures cough impact on daytime activities and sleep. A widely available instrument with established measurement properties that measures cough symptom severity rather than cough QoL remains unavailable.
We aim to develop a cough symptom severity instrument—the McMaster Cough Severity Questionnaire—for use in patients with RCC/UCC. To inform item generation for the instrument, we conducted a systematic survey in which we identified 43 items addressing the following domains: urge-to-cough sensations (subdomains: frequency and intensity) and cough symptom (subdomains: frequency, control, bout duration, intensity and associated features/sequelae) [16]. To assess the comprehensiveness and appropriateness of items, domains and subdomains identified in our systematic survey, we conducted patient focus groups and consultation with clinical experts, and report here our findings.
Methods
Patient focus groups
We conducted focus groups with patients with RCC/UCC to explore: 1) attributes of their cough and its severity; and 2) issues important to patients in relation to their cough severity. This report adheres to consolidated criteria for reporting qualitative research standards [17].
Patient recruitment
We recruited 16 adult (≥18 years old) patients with RCC/UCC from a tertiary care clinic at the McMaster University Medical Centre (Hamilton, Ontario, Canada). Eligible patients experienced cough lasting >8 weeks. We excluded patients who currently smoked or had a smoking history of >10 pack-years; whose English was limited; or who presented with memory, cognitive or psychiatric issues preventing optimal participation. Patients provided written informed consent and received $50 for participating. The Hamilton Integrated Research Ethics Board provided ethics approval (No. 12-881).
Sample
We employed purposive sampling to obtain experiences among a diversity of patients with RCC/UCC [18]. Our sample size was based on the anticipated number of patients required to reach thematic saturation on the concept of cough symptom severity [19].
Group configuration and data collection
Following informed consent, a study coordinator (E.K.) contacted patients over the telephone to establish their age, sex, smoking history and comorbidities. The coordinator convened three focus groups, each with five to six patients.
Following a semi-structured guide (supplementary Appendix E1), a trained interview facilitator (E.K.) led the focus group discussions over Zoom videoconferencing, each for 60–90 min. A prior systematic survey [16] informed an initial draft of the interview guide that was subsequently revised based on input from the steering group (G.H.G., I.S.). The facilitator asked open-ended questions, followed by directed questions on themes identified from the systematic survey. As patients discussed, the facilitator identified emerging themes for further discussion. To ensure full exploration of themes, we provided patients with the opportunity to add comments at the end. Focus groups were audio-recorded, transcribed verbatim and de-identified.
Data analysis
We used directed content analysis, informed by a prior conceptual framework [16], to identify related themes [20]. Two researchers (E.K., C.M.) independently coded transcripts by assigning statements to items or domains in the framework. The two researchers discussed statements that could not be categorised within existing items or domains, and if relevant, created a new code. Researchers then summarised these codes as a new item or domain contributing to our evolving conceptual framework. The study team, comprised of clinical experts, methodologists and patient partners, reviewed the results of the analysis, and resolved disagreements through discussion leading to consensus.
Expert consensus study
We elicited feedback from an international panel of chronic cough experts on the comprehensiveness and appropriateness of items and domains identified from the systematic survey and patient focus groups. Using purposive sampling, we invited 14 key opinion leaders in chronic cough, all of whom agreed to participate. The final group consisted of 18 members (the steering group: E.K., G.H.G., P.M.O.B., I.S., and 14 experts: R.A., H.B., L.P.B., R.C., P.D., L.D., S.K.F., .CL.F., P.G.G., R.S.I., P.M., L.M., J.A.S., W.J.S.). Experts came from the UK, USA, Canada and one each from Australia, Belgium, China, Ireland, Saudi Arabia and South Korea.
Pre-meeting survey and feedback
Without having seen our conceptual framework, expert panel members provided 3–10 questions to assess patients’ severity of cough. Once returned, the steering group then sent a draft conceptual framework, from which experts could provide written suggestions to either drop, merge and/or add items or domains.
Consensus meeting
The steering group and expert panel participated in a 1-hour videoconference to reach consensus on the items and domains for a cough symptom severity instrument. The steering group presented the results of the systematic survey, patient focus groups and pre-meeting feedback. Following presentation of the results, experts participated in discussions addressing the proposed items and domains. After the conference, the steering group sent expert panel members a report of the discussion and a modified list of items and domains based on their feedback. Experts had the opportunity, if desired, to provide additional written feedback.
Results
The 16 focus group patients had a median age of 61 years. Most identified as female (68.8%), reported no history of smoking (81.3%) and coughed for a median duration of 13.5 years (table 1).
Characteristics of focus group patients (n=16)
Statements from patients provided 48 items that we categorised under two broad domains of cough symptom severity: urge-to-cough sensations (subdomains: frequency and intensity) and cough symptom (subdomains: control, frequency, fit/bout duration, intensity, quality and associated features/sequelae) (figure 1; table 2).
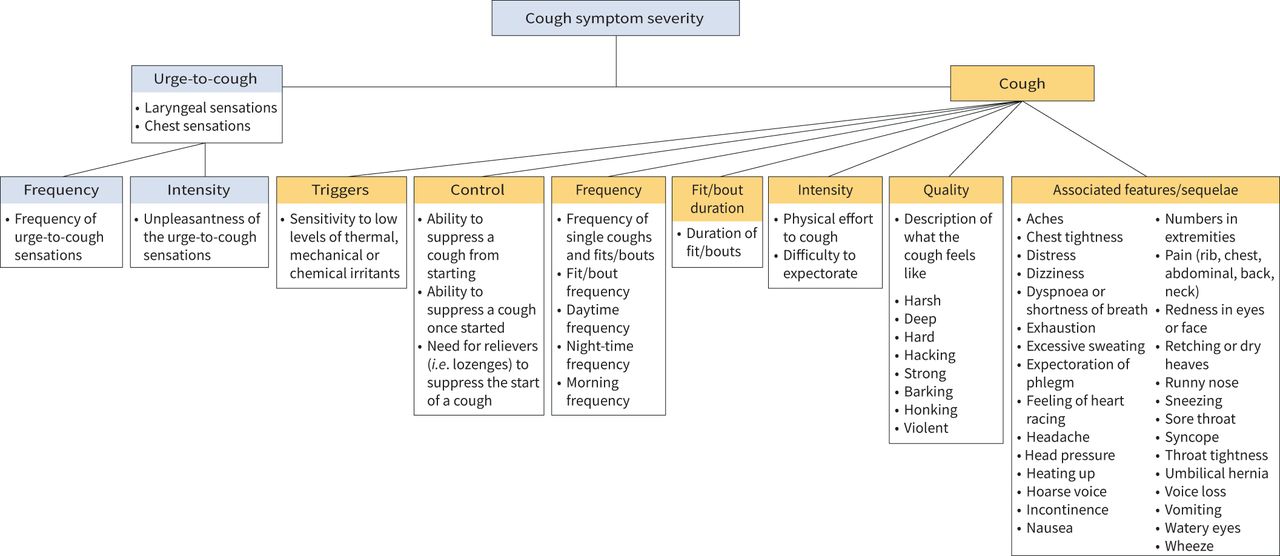
Conceptual framework of cough symptom severity in patients with refractory or unexplained chronic cough (RCC/UCC).
Domains and items related to measurement of cough symptom severity in patients with refractory or unexplained chronic cough (RCC/UCC)
Urge-to-cough sensations
Patients described sensations, including “tickle”, “chest pressure”, “chest tightness”, “something in the back of the throat” and “hoarseness”, as antecedents to coughing. These sensations could vary in terms of intensity: “Most of the severe ones start with that karate chop effect in my throat. […] Another time, I will feel pressure in my chest… like someone's pushing with their hand down on my chest” (Patient 15). The frequency with which patients experienced these sensations ranged considerably, some reporting a constant sensation and others reporting that it occurs less consistently or not at all:
I'm constantly feeling as though I want to clear the back of my throat.
(Patient 3)
So there's not always any sensation or sign that it's going to come on. I do get sometimes that dry tickle [but] it's not consistent.
(Patient 1)
When asked to compare the severity of their urge-to-cough sensations in relation to their cough, patients reported different experiences:
When I said my urge-to-cough is severe, it's just as severe as the cough… one is not worse than the other.
(Patient 12)
My urge-to-cough, is it more severe than the cough itself? Not necessarily.
(Patient 6)
Cough control
Patients perceived an ability to suppress the start of their cough as a less severe cough: “At the beginning, I know I could take a cough drop, and it would make it less severe or I could drink water and it may control it a bit, but I mean those possibilities are long gone way in the past” (Patient 14). The lack of control was often attributed to an urge sensation: “It just seems that, as the phlegm builds up it just gets to a point where you just have no choice. I mean you're going to cough” (Patient 3). Patients also described cough severity in terms of control once a cough had started: “There's no ability to stop it or control it; it's like it takes over, it just takes over your body and until that cough is out” (Patient 10). Some patients shared that, once started, their ability to bring a cough under control was dependent upon bringing up phlegm.
Cough frequency and fit/bout duration
Patients assessed cough severity in terms of the number of coughs (single or episodes) that they experience in a day: “I judge severity by frequency, so some days I may only have three to four episodes which I would classify as a good day, other days I may have 12 to 15 episodes which obviously, is not so good of a day, so I kind of throw that in there with severity – how many episodes I have” (Patient 1). When describing cough frequency, patients noted that periods of the day (i.e. morning, daytime and/or night-time) may be more or less problematic: “Whether at any time of day or night I'm worse in the morning [and] worse at night, but I do cough all day long” (Patient 11). In addition to variation within a day, patients noted that each day could differ in terms of frequency: “It's not really a daily thing, like the milds would be daily, sometimes like anywhere from 10–20 times in a day I'll have a mild cough. The severe ones, it all depends upon when somebody tells a good joke or somebody makes me laugh is when I get my more severe coughs so it varies right? It could be once a week, some maybe once a month” (Patient 16). When asked to recall cough frequency, some patients struggled to provide an estimate and alluded to preoccupation with their coughing or the fact it had become inured to them: “I don't keep track of how many times I cough a day, I just know I cough constantly” (Patient 10). The number of fits/bouts of coughing seemed easier to recall: “I have it mostly everyday, some days I may have 1 or maximum 2 of what I would call the severe cough” (Patient 6). The duration of coughing fits/bouts was seen as a factor to their overall perception of cough severity: “Many times, my cough gets so bad that I will go for 5–10 min” (Patient 15).
Cough quality and intensity
Patients provided descriptions about the sensory experience of coughing, including “hacking”, “harsh”, “strong”, “deep” and “barking”. The study team classified these terms separately from intensity, which patients conveyed in terms of the physical effort required to cough and the difficulty expectorating:
It can get so severe that I literally have to go to the sink just to hold on just to keep my body.
(Patient 9)
It's just sometimes, the phlegm comes up very easily, very quickly. Other times I'll have to really start to expel it and pressure it.
(Patient 6)
Associated features/sequelae
Patients described symptoms during or immediately after an episode of coughing, including headache and pain around their chest, ribs, abdomen or back: “It just seems to be like every part of your chest and all around there ache, like really ache, when it's really bad” (Patient 5). Patients described feeling breathless, dizzy, wheezy and/or on the verge of fainting after a fit of coughing: “At times it'll get bad enough, where I blackout, or I feel like I'm going to blackout, like I can't get my breath, I'm choking constantly” (Patient 4). Coughing drove some patients to vomit or retch, and many felt exhausted: “You just feel very weak, like you just feel sick and helpless. It takes a lot out of you, a lot of energy” (Patient 15). Female patients described stress incontinence following a severe cough. Less common symptoms included hernia, rib fracture, voice loss, hoarseness, chest and head pressure, throat and chest tightness, and feeling overly heated (figure 1, table 2).
Conceptual difference between cough symptom severity and impact
Although cough symptom severity is related to cough impact on QoL, patients reported differences in the extent to which the same symptom could be viewed as bothersome: “I feel like my cough is very minimal, because I do not have these violent coughs. I do not choke, my heart rate is always normal and my cough, as I said, I do not get violent coughs. But still it's bothering me a lot, especially during the night” (Patient 8). The study team therefore classified impact on QoL as a separate concept from symptom severity.
Expert consensus
An open-ended survey to members of the expert panel identified 32 potential items/domains considered relevant to cough symptom severity (table 3). During the consensus meeting, experts agreed that severity should be conceptualised as an overarching term encompassing domains of frequency, intensity, duration, quality and associated features/sequelae. Experts also agreed that urge-to-cough is an important symptom to capture in a cough severity instrument. A small minority viewed the impact of cough symptoms on QoL (i.e. daily activities, ability to speak, social life) as a necessary aspect of symptom severity. Experts raised cough hypersensitivity as a potentially missing concept from the framework. Thus, the steering group added “triggers” as an additional subdomain (figure 1).
Open-ended responses among 11 experts regarding items/domains to assess of cough symptom severity
Discussion
We report consensus findings from patient focus groups and expert panel discussions regarding items and domains to assess cough symptom severity in patients with RCC/UCC. The study confirms findings from a prior systematic survey and identifies eight additional items/domains. The final conceptual framework includes 51 items arranged under two broad domains of urge-to-cough (subdomains: frequency and intensity) and cough symptom (subdomains: triggers, control, frequency, fit/bout duration, intensity, quality and associated features/sequelae) (figure 1).
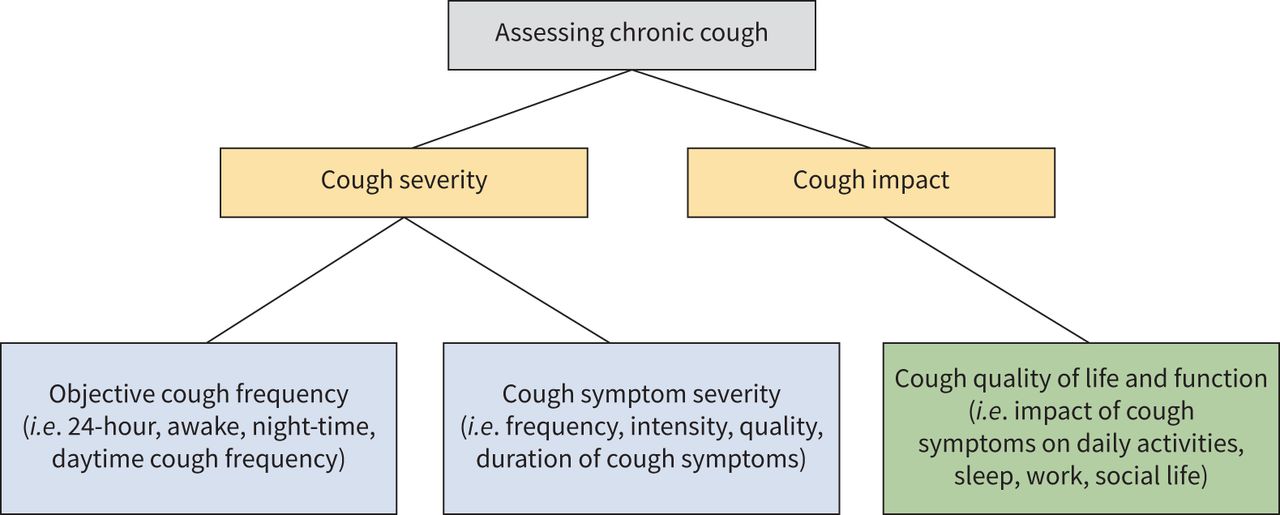
Although experts and patients agreed on the appropriateness of items and domains, a small minority of experts viewed the impact of cough on QoL as a necessary component of symptom severity. Evaluation of symptom severity and impact on QoL provides a complete assessment of cough (figure 2). An instrument addressing symptom severity alone may, however, be important for several reasons.

{kind=link}
{kind=link}
Assessing cough in patients with refractory or unexplained chronic cough (RCC/UCC).
First, there is substantial variation in the extent to which patients find the same symptoms bothersome. Impact on QoL can be influenced by factors other than cough symptom severity, including comorbid anxiety and depression [21]. As this study focused solely on symptom severity, rather than impact, the domains identified are less likely to be influenced by distal factors.
Second, the experience of chronic cough over years can have a cumulative impact on QoL that may not be responsive to change in symptom severity over short periods of treatment. As current patient-reported outcome measures primarily assess cough impact on QoL and demonstrate modest association with objective measures [22–24], cough symptom severity requires directed and targeted measurement that responds well to treatment effects.
Third, neuromodulatory agents can improve cough QoL with little to no effect on underlying objective cough frequency [8, 9]. A subjective instrument assessing change in cough severity, rather than impact, is therefore needed to establish whether treatment is targeting the intended symptom. For this reason, regulatory agencies often require that primary end-points measure on-target effects to establish effectiveness for claimed indications.
Fourth, although cough frequency monitors are ideal to objectively assess cough, their limited feasibility in clinical practice suggests potential utility in developing a symptom severity instrument for better longitudinal assessment. The cough severity VAS, although widely used in clinical practice, has limitations as a single-item instrument, and there is lack of evidence supporting its measurement properties.
Finally, a cough symptom severity instrument that assesses domains of cough and urge-to-cough sensations may identify subgroups of patients who share cough pathophysiology [25]. Although current guidelines recommend treatment with centrally acting neuromodulatory agents and speech therapy, there is currently limited evidence to inform patients who may benefit more from a specific treatment. As new therapies, including peripherally acting P2×3 antagonists [26–31], that target specific pathophysiology are introduced, stratification of patients with chronic cough based on domains of cough symptom severity may be useful for precision medicine.
A qualitative study informed development of the CSD and identified three concepts under cough severity: intensity, frequency and disruption [32]. Although our results are consistent with themes identified in their study, our work differs in that we involved patient partners and experts to optimally define the measurement construct of a cough symptom severity instrument [33–35] and strove for conceptual clarity by excluding items/domains related to cough impact on QoL.
Other strengths of this study include strict inclusion of patients who would qualify for phase 2/3 antitussive clinical trials [28, 29] and triangulation of focus groups with an existing framework, patient partners and clinical experts.
Limitations include recruitment of English-speaking patients from a single tertiary clinic; potential selection bias of experts; potential response bias among focus group patients; and subjectivity in interpretation of themes leading to consensus.
Conclusion
We outline a conceptual framework for measuring cough symptom severity in patients with RCC/UCC. The results support content validity of a patient-reported outcome measure. Future studies should address items and domains that are most important to patients for item reduction of a cough symptom severity questionnaire.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00667-2021.SUPPLEMENT
Acknowledgements
We thank our patient partners, Faye Johnston, Robert Newman and Nada Popovic, for providing feedback on our manuscript. We also thank Mariam Awadalla and Hisham Alkassem for their assistance transcribing the focus groups.
Footnotes
Provenance: Submitted article, peer reviewed.
Author contributions: I. Satia is the guarantor of the study. E. Kum, G.H. Guyatt, P.M. O'Byrne and I. Satia formed the steering group and conceived the study. E. Kum, C. Munoz, S. Beaudin and S-A. Li contributed to data collection. R. Abdulqawi, H. Badri, L-P. Boulet, R. Chen, P. Dicpinigaitis, L. Dupont, S.K. Field, C.L. French, P.G. Gibson, R.S. Irwin, P. Marsden, L. McGarvey, J.A. Smith and W-J. Song served as expert panel members. E. Kum, G.H. Guyatt and I. Satia analysed and interpreted the data. E. Kum wrote the first draft of the manuscript. All authors critically reviewed and approved the final manuscript.
Conflicts of interest: E. Kum, G.H. Guyatt, C. Munoz, S. Beaudin, S-A. Li, R. Abdulqawi, H. Badri, L. Dupont and L. McGarvey report no conflicts of interest. L-P. Boulet reports grants from Amgen, AstraZeneca, GlaxoSmithKline, Merck, Novartis and Sanofi-Regeneron, and personal fees from AstraZeneca, Covis, Novartis, GlaxoSmithKline, Merck and Sanofi-Regeneron, outside the submitted work. R. Chen reports grants and personal fees from AstraZeneca and GlaxoSmithKline, and personal fees from Novartis and Merck, outside the submitted work. P. Dicpinigaitis reports consulting fees from Merck, Bellus, Bayer, Shionogi and Chiesi, outside the submitted work. S.K. Field has served on advisory boards for GSK and Merck, has given sponsored talks for Boehringer Ingelheim, GlaxoSmithKline and Novartis, and has received research funding from AstraZeneca, CIHR, InsMed and Novartis, outside of the submitted work. C.L. French and R.S. Irwin disclose that they are co-developers and hold the copyright of the CQLQ and have each received less than $700 in fees over the past 3 years for its use in studies. P.G. Gibson reports grants from GlaxoSmithKline, and personal fees from AstraZeneca, Chiesi, GSK, Novartis and Sanofi, outside the submitted work. P. Marsden reports an investigator-initiated grant from Merck Sharpe & Dohme Ltd outside the submitted work. W-J. Song reports grants from MSD and AstraZeneca, consulting fees from MSD and AstraZeneca, and lecture fees from MSD, AstraZeneca, GlaxoSmithKline and Novartis, outside the submitted work. J.A. Smith reports grants from Merck, Ario Pharma, GlaxoSmithKline, NeRRe Pharmaceuticals, Menlo, Bellus and Bayer, and personal fees from Chiesi, Ario Pharma, GlaxoSmithKline, NeRRe Pharmaceuticals, Menlo, Bellus, Bayer, Boehringer Ingleheim, Genentech and Neomed, outside of the submitted work. J.A. Smith is a named inventor on a patent, owned by Manchester University NHS Foundation Trust and licensed to Vitalograph Ltd, describing the detection of cough from sound recordings. The VitaloJAK cough monitoring algorithm has been licensed by Manchester University Foundation Trust (MFT) and the University of Manchester to Vitalograph Ltd and Vitalograph Ireland (Ltd). MFT receives royalties that may be shared with the clinical division in which J.A. Smith works. P.M. O'Byrne reports grants and personal fees from AstraZeneca and Medimmune, personal fees from GlaxoSmithKline and Chiesi, and grants from Novartis and Biohaven, outside the submitted work. I. Satia reports an ERS Respire 3 Marie Curie Fellowship, grants and personal fees from Merck Canada, and personal fees from GlaxoSmithKline and AstraZeneca, outside the submitted work.
- Received November 26, 2021.
- Accepted January 14, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










