





Abstract
Background Chronic cough is a common troublesome condition, but risk factors for developing chronic cough are poorly understood. The aim of this study was to understand the relationship between mental health disorders, personality traits and chronic cough.
Methods The Canadian Longitudinal Study on Aging is a prospective, nationally generalisable, random sample of adults aged 45–85 years at baseline recruited between 2011 and 2015, and followed-up 3 years later. Chronic cough was defined as a daily cough over the last 12 months. Incident chronic cough was defined as those participants who reported new-onset chronic cough between baseline and follow-up 1. Current depressive symptoms and psychological distress were assessed using the Center for Epidemiologic Study Short Depression Scale (CESD-10) and Kessler Psychological Distress Scale (K-10), respectively. The “Big Five” personality traits were assessed using the Ten-Item Personality Inventory. Relative risks are reported using a multivariate mutually adjusted model.
Results At follow-up 1, 2506 participants (11.1%) reported new-onset chronic cough during the ∼3-year interval. Depressive symptoms (CESD-10 ≥10: relative risk 1.22 (95% CI 1.03–1.44)) and psychological distress (K-10 ≥22: relative risk 1.20 (95% CI 1.07–1.36)) at baseline were both independent predictors of a higher risk of incident chronic cough. Prevalent and incident chronic cough were also independently associated with an increased risk of developing depressive symptoms and psychological distress. Personality traits did not influence the development of chronic cough but did increase the risk of depressive symptoms and psychological distress.
Conclusions This study shows that there is a bidirectional relationship between chronic cough, and depressive symptoms and psychological distress, and personality traits do not independently influence the development of chronic cough.
Abstract
There is a bidirectional relationship between chronic cough, and depressive symptoms and psychological distress. Personality traits do not independently influence the development of chronic cough. https://bit.ly/3NOMXi3
Introduction
Chronic cough is a common troublesome condition with a global prevalence ranging from 2% to 18% [1]. Cough is also the leading cause for ambulatory and primary care visits to physicians [2–4], and chronic cough lasting >8 weeks is one of the commonest reasons for referrals to a pulmonologist [5]. Chronic cough is associated with significant impairment in quality of life, including physical, social and psychological domains [6]. Understanding the risk factors that lead to chronic cough could help identify at-risk populations and knowledge of the consequences can help provide better care by providing a more holistic patient-centred approach.
Risk factors for developing chronic cough from epidemiological studies from the general community and specialist cough clinics have identified an increase in the prevalence and incidence of chronic cough with ageing, sex, current smoking, higher body mass index (BMI), respiratory airways diseases (asthma, chronic obstructive airways diseases and bronchiectasis), worsening lung function, airflow obstruction and gastro-oesophageal reflux disease [7–9]. However, patients with chronic cough attending cough clinics often have none of these conditions.
A number of cross-sectional studies have recognised depression and mood disorders as one of the most common comorbidities associated with chronic cough [10–14]. However, it is not possible to determine if mental health disorders are a risk factor or a consequence from cross-sectional data. Current data from longitudinal studies are also inconclusive. The Rotterdam Study found no increase in the incidence of chronic cough in those with high depressive symptom scores [15]. In contrast, descriptive data from the Canadian Longitudinal Study on Aging (CLSA) recently demonstrated that participants with self-reported prior history of depression and anxiety had a greater incidence of chronic cough [8]. However, further analyses are required to determine if the association of mental health with chronic cough is independent of other covariates. Also, current symptoms of depression as well as psychological distress may be more relevant predictors of chronic cough than a previous lifetime history of depression or anxiety. The impact of personality traits should also be considered, as these are considered important predictors of mental health disorders [16, 17].
The objectives of this study were to investigate 1) if mental health disorders and personality traits are independently associated with the development of chronic cough, and 2) whether chronic cough is independently associated with the development of depressive symptoms and psychological distress.
Study design and methods
Study design and population
The CLSA is a large, nationally generalisable, stratified random sample of 51 338 Canadian men and women aged 45–85 years at baseline (2011–2015) from the 10 Canadian provinces [18]. Eligible participants had to be physically and cognitively able to participate on their own and not living in institutions such as long-term care facilities. Participants were recruited in the tracking cohort (n=21 241) and the comprehensive cohort (n=30 097). Participants in the comprehensive cohort were randomly selected from within 25–50 km of 11 data collection sites, located in seven provinces (n=30 097). In addition to completing in-person interviews, the comprehensive participants completed in-depth physical assessments. Details on the study design have been described elsewhere [19]. Each participant is followed every 3 years for 20 years or until death. The first follow-up was conducted between 2015 and 2018. The comprehensive data from baseline and follow-up 1 were included in the current analyses. This study was approved by the Hamilton integrated Research Ethics Board and by the CLSA Scientific Advisory Board (1909024).
Chronic cough definition
Definitions were based on responses from direct questioning of participants by trained research assistants at baseline and follow-up using standardised questionnaires. Participants at some sites in Ontario and Quebec were given a choice to complete the interview in English or French. The language used to complete the questionnaire was used as the dominant language of the participant in this study. Participants who self-reported as having a daily cough on most days in the last 12 months were categorised as having a chronic cough at baseline or follow-up 1. Prevalent chronic cough was defined as those participants reporting chronic cough at baseline, while incident chronic cough was defined as those participants who did not report chronic cough at baseline but did at follow-up 1.
Assessment of mental health disorders
The Center for Epidemiologic Study Short Depression Scale (CESD-10) was administered to assess depressive symptoms at baseline and follow-up 1 [20]. The short version is a 10-item questionnaire that assesses feelings in the past 1 week of being easily bothered, difficulty concentrating, depression, the effort required to perform activities, fearfulness, restless sleep, loneliness, hopefulness about the future and happiness. Each item has four possible responses: 0=rarely or never, 1=some of the time, 2=occasionally and 3=all of the time. The positive questions on happiness and hopefulness about the future are reversed scored and added to the other eight questions to provide a total range of 0–30, where a score ≥10 indicates current depressive symptoms [20, 21].
The Kessler Psychological Distress Scale (K-10) was administered to identify the more severe range of psychological distress as it has been shown to predict a diagnosis of serious mental illness [22, 23]. Questions are based on a 4-week recall of feeling tired out, nervous, unable to calm down, hopeless, restless or fidgety, unable to sit still, depressed, everything is an effort, unable to be cheered up and worthless. These 10 questions are rated on a scale of 1 (none of the time) to 5 (all of the time) with a total possible score of 50, where a score ≥22 is considered high or very high psychological distress [23].
Assessment of personality traits
The “Big Five” personality traits of openness, conscientiousness, extraversion, agreeableness and emotional stability were measured using the Ten-Item Personality Inventory [24]. This is a 10-item questionnaire with two paired items for each “Big Five” trait. Each item is scored on a 7-point Likert scale where 1=disagree strongly, 4=neither agree nor disagree and 7=agree strongly. Five of the 10 items are reversed scored, added with their matching pair in the relevant “Big Five” traits and averaged to provide a single score for each domain out of 7. A score <4 is considered low in that specific personality trait.
Statistical analysis
Descriptive statistics for demographics and covariates are presented as categorical variables for incident chronic cough and reported as frequencies (percentages). Covariates that impact the incidence of chronic cough were included in the core model: age, sex, smoking status, BMI, educational level, province, self-reported general health, interview language (French versus English) and physician-diagnosed respiratory airways diseases (asthma and COPD) [8].
Baseline CESD-10, K-10 and individual personality trait scores were added to the final mutually adjusted incidence model for chronic cough. The same covariates were used for incident depressive symptoms and psychological distress. Incident depressive symptoms were considered in those participants who scored <10 at baseline but ≥10 at follow-up 1, and likewise for K-10 <22 at baseline and ≥22 at follow-up 1.
We employed Proc GENMOD in SAS version 9.4 (SAS Institute, Cary, NC, USA) with Poisson distribution and log link for calculating the multivariable relative risk, and assessed the association of all covariates with the outcomes of incident cough, depressive symptoms and psychological distress. The analyses were also stratified by language (English versus French).
Results
Study population and demographics
The comprehensive cohort included 30 097 participants at baseline. A total of 29 972 completed the chronic cough question at baseline. At follow-up 1, 22 547 participants who did not report chronic cough at baseline completed the chronic cough question. In this follow-up sample who did not report baseline cough, 2506 participants (11.1%; mean±sd age 64.4±10.0 years) reported new-onset chronic cough during the ∼3-year interval. The proportion of participants with incident chronic cough was higher with increasing age, in males and current smokers, and was lowest in Quebec compared with Ontario (8.0% versus 13.6%, respectively) (table 1). There was a greater proportion of participants who developed chronic cough and scored lower (<4) on the agreeableness, conscientiousness and emotional stability personality traits at baseline. Similarly, there was also a greater proportion who demonstrated higher depressive symptoms (CESD-10 ≥10: 15.2%) and psychological distress (K-10 ≥22: 16.0%) at baseline.
Descriptive data on incident chronic cough at follow-up 1 (n=22 547)
Effects of mental health disorders and personality traits on the incidence of chronic cough
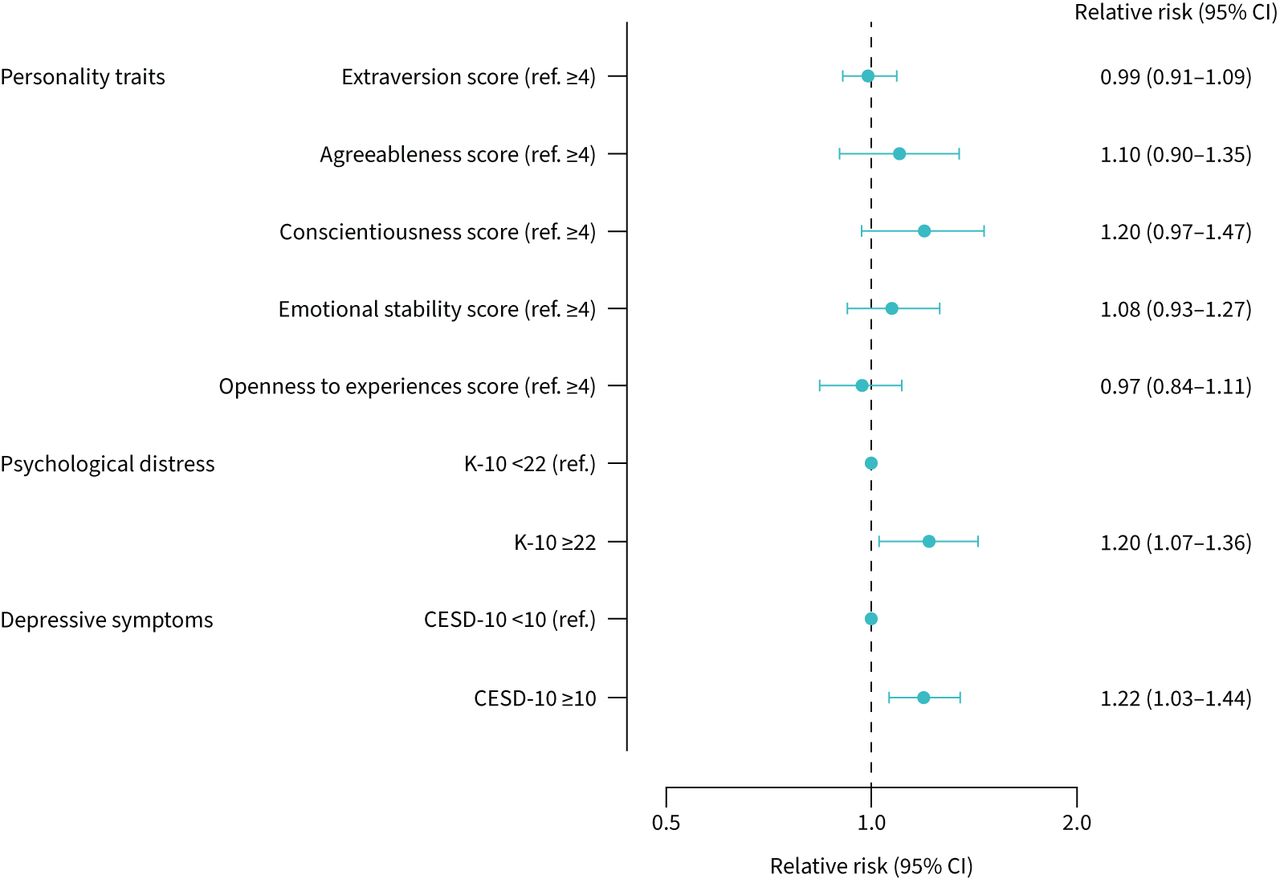
After adjusting for all the variables in the core model, depressive symptoms (CESD-10 ≥10: relative risk 1.22 (95% CI 1.03–1.44)) and psychological distress (K-10 ≥22: relative risk 1.20 (95% CI 1.07–1.36)) at baseline were both independent predictors of a higher risk of incident chronic cough 3 years later by 22% and 20%, respectively (figure 1 and supplementary table E1). None of the five personality traits independently demonstrated any increased risk on the incidence of chronic cough. The effect of psychological distress and depressive symptoms was similar for prevalent chronic cough (supplementary figure E1).

The independent effects of personality traits, depressive symptoms and psychological distress on the incidence of chronic cough. The complete model is mutually adjusted for all variables including age, sex, smoking status, body mass index, educational level, province, self-reported general health, interview language and physician-diagnosed respiratory airways diseases (asthma and COPD). K-10: Kessler Psychological Distress Scale; CESD-10: Center for Epidemiologic Study Short Depression Scale.
The CESD-10 individual item scores were further explored by subclassifying into lack of positive affect scores (two questions, maximum 6 points) and depressive affect scores (eight questions, maximum 16 points) with increasing cut-off values. A cut-off score of 1 for lack of positive affect scores was associated with a 12% increase in chronic cough (relative risk 1.12 (95% CI 1.02–1.23)) while a cut-off of 8 for depressive affect scores demonstrated a 29% increase (relative risk 1.29 (95% CI 1.15–1.45)) (supplementary table E2).
Effects of chronic cough on depressive symptoms
Compared with participants without chronic cough, those who had chronic cough at baseline, at follow-up 1 or both had a greater proportion of participants with new depressive symptoms at follow-up 1 (CESD-10 ≥10) (table 2). A greater proportion of participants who developed depressive symptoms scored lower (<4) on the agreeableness, conscientiousness, emotional stability and openness to new experiences personality traits at baseline. In addition, there was also a greater proportion who demonstrated higher psychological distress scores (K-10 ≥22: 35.0%) at baseline.
Descriptive data on incident depressive symptoms and psychological distress at follow-up 1
After adjusting for all the variables in the core model, chronic cough at baseline, follow-up 1 or both were all independently associated with an estimated 27% and 22% increase in the risk of incident depressive symptoms (relative risk 1.27 (95% CI 1.06–1.52), 1.22 (95% CI 1.04–1.43) and 1.27 (95% CI 1.07–1.50), respectively) (figure 2). This was independent of the increased risk associated with a higher psychological distress score (K-10 ≥22: relative risk 3.13 (95% CI 2.67–3.66)) at baseline and lower scores (<4) on extraversion, conscientiousness, emotional stability and openness to new experiences personality traits.
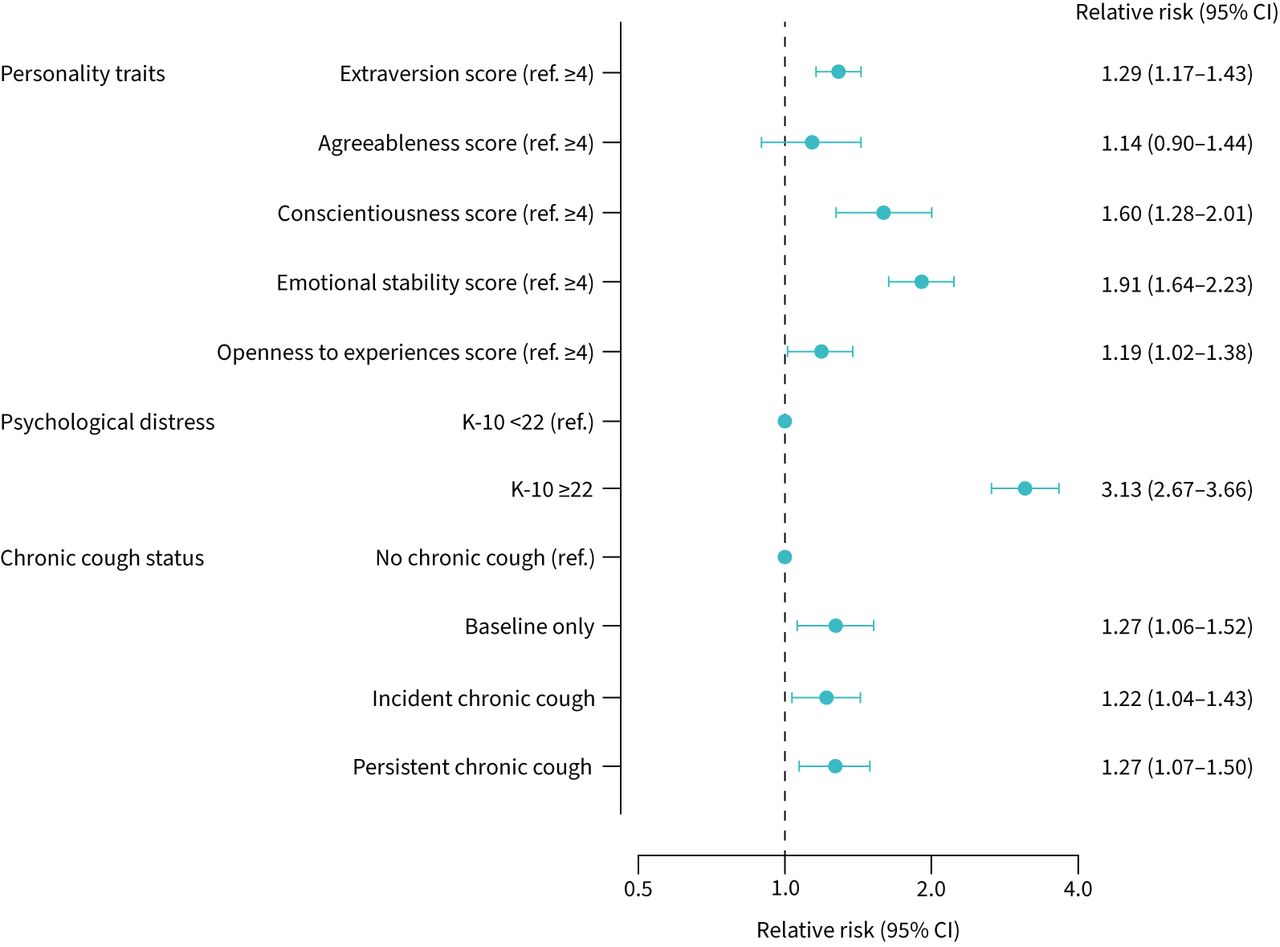
The independent effects of chronic cough, personality traits and psychological distress on the incidence of depressive symptoms (Center for Epidemiologic Study Short Depression Scale (CESD-10) ≥10). The complete model is mutually adjusted for all variables including age, sex, smoking status, body mass index, educational level, province, self-reported general health, interview language and physician-diagnosed respiratory airways diseases (asthma and COPD). K-10: Kessler Psychological Distress Scale.
Effects of chronic cough on psychological distress
Compared with participants without chronic cough, those who had chronic cough at baseline, at follow-up 1 or both had a 1.5–2.5% greater proportion of participants with new-onset symptoms of psychological distress at follow-up 1 (K-10 ≥22) (table 2). There was also a greater proportion of participants who developed symptoms of psychological distress and scored lower (<4) on the conscientiousness and emotional stability personality traits at baseline. In addition, there was also a greater proportion who demonstrated higher depressive symptoms scores (CESD-10 ≥10: 13.0%) at baseline.
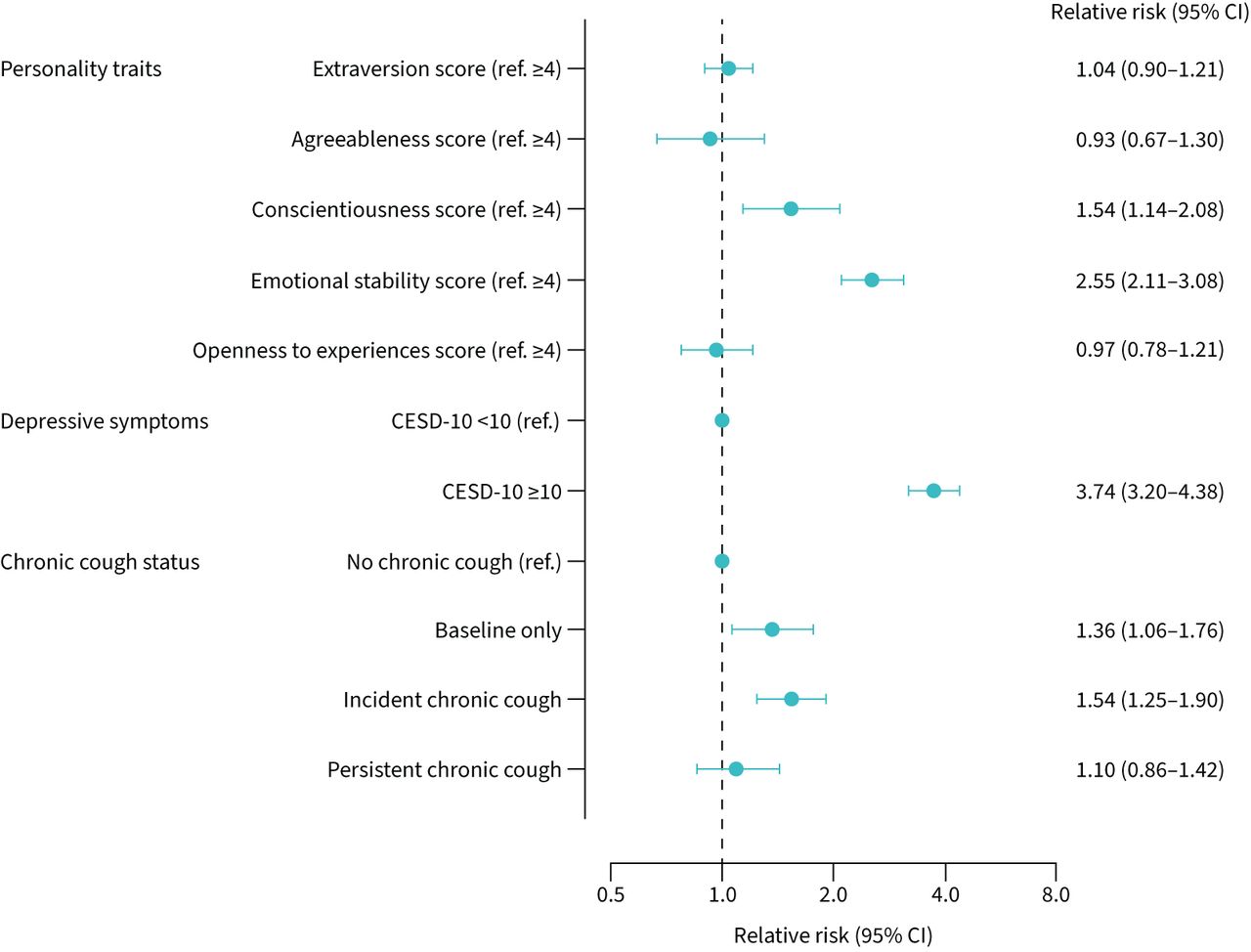
After adjusting for all the variables in the core model, chronic cough at baseline and follow-up 1 were both independently associated with an estimated 36% and 54% increase in the risk of incident psychological distress (relative risk 1.36 (95% CI 1.06–1.76) and 1.54 (95% CI 1.25–1.90), respectively) (figure 3). This was independent of the increased risk associated with a higher depressive symptom score (CESD-10 ≥10: relative risk 3.74 (95% CI 3.20–4.38)) at baseline and lower scores (<4) on conscientiousness and emotional stability personality traits.
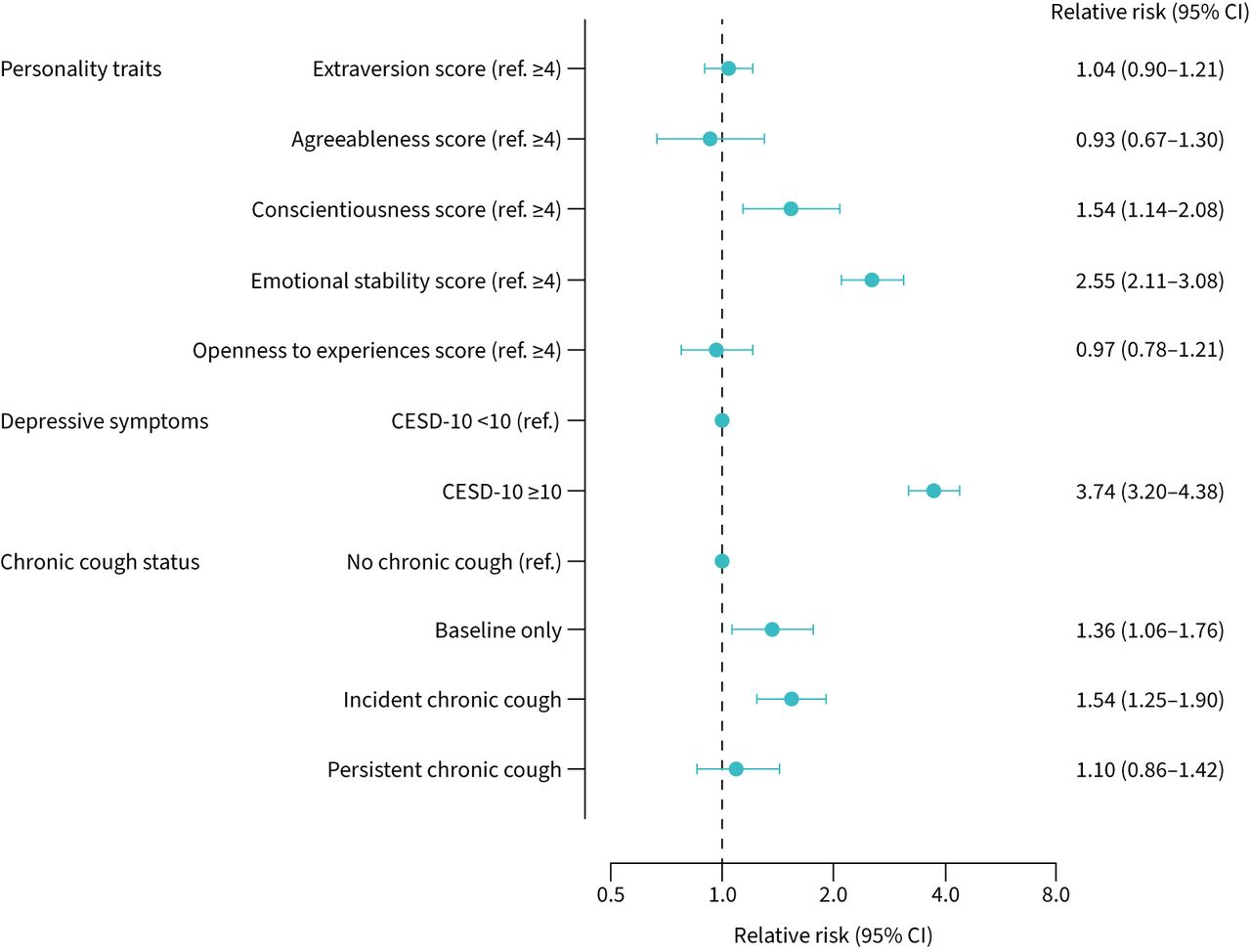
The independent effects of chronic cough, personality traits and depressive symptoms on the incidence of psychological distress (Kessler Psychological Distress Scale (K-10) ≥22). The complete model is mutually adjusted for all variables including age, sex, smoking status, body mass index, educational level, province, self-reported general health, interview language and physician-diagnosed respiratory airways diseases (asthma and COPD). CESD-10: Center for Epidemiologic Study Short Depression Scale.
Effects of English and French language on the incidence of chronic cough
As the incidence of chronic cough was lowest in Quebec and highest in Ontario, the language the interview was conducted in was included in the core model for incidence of chronic cough. Compared with French speaking participants, those who were English speakers had a trend of 27% higher risk of incident chronic cough (relative risk 1.27 (95% CI 0.99–1.64)) (supplementary table E1), independent of all other covariates in the model. Hence, the relative risk of all covariates including mental health disorders and personality traits for incident chronic cough were stratified based on English and French speaking (supplementary table E1). Personality traits were not associated with an increased risk in either English and French speakers; however, only in English speakers were high depressive symptoms (relative risk 1.30 (95% CI 1.14–1.48)) and high psychological distress (relative risk 1.21 (95% CI 1.00–1.47)) associated with an increased risk of developing chronic cough.
Discussion
Healthcare professionals investigating and managing patients with refractory or unexplained chronic cough often question whether excessive coughing is due to expression of an underlying mental health disorder or personality trait. The results of this study provide novel insights which suggest that there is a bidirectional relationship that is indirectly influenced by personality traits and also varies between English and French speakers. Depressive symptoms and psychological distress are independently associated with the development of chronic cough, but chronic cough also independently increases the risk of developing depressive symptoms and psychological distress. Personality traits do not directly influence the development of chronic cough, but may do so indirectly via their contribution to the development of depressive symptoms and psychological distress (figure 4). Furthermore, the association of mental health disorders on the development of chronic cough was only found in English speakers but not in French speakers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of findings.
Understanding the mechanisms by which mental health disorders might influence coughing requires an appreciation of the neurophysiology of cough. Coughing is under both voluntary and involuntary control, but it is widely recognised that the cough reflex is the archetypal airway defensive reflex which can be initiated by mechanical, chemical and thermal stimulation. Chronic cough is currently thought to be due to dysregulation of the peripheral and/or central nervous system [25, 26], and is often described as cough hypersensitivity syndrome [27] due to either 1) increased stimulation of the peripheral nerve terminals, 2) neuronal hyperexcitability of the afferent vagal nerve, brainstem and higher cortical projections [28–30], and/or 3) impaired central inhibitory control [30–32]. Recent studies suggest patients with chronic cough demonstrate a lack of voluntary cough suppression [33] and impairment in the descending inhibitory control neurons [31, 33]. Impairment in these inhibitory neurons has also been demonstrated in depression [34], as well as in irritable bowel syndrome [35], fibromyalgia [36] and chronic pain [37], which are also associated with chronic cough [15, 38, 39]. The neurotransmitters responsible for these inhibitory neurons to be functional are currently thought to be endogenous opioids, endorphins, serotonin, norepinephrine and dopamine [40–43]. Current guidelines suggest off-label use of low-dose opioids, pregabalin, gabapentin and amitriptyline for chronic cough, which would increase the levels of such neurotransmitters [44–46]. This is further supported by two studies demonstrating improvement in depressive symptoms after treatment of chronic cough [11, 47]. Therefore, depression and chronic cough have a shared neurobiology.
The idea that chronic cough increases depressive symptoms and psychological distress is conceptually more intuitive. The median cough frequency in patients with refractory or unexplained chronic cough recruited into clinical trials over a 24-h period is ∼20 coughs·h−1, with more coughing during the daytime than night-time [48–52]. This high number of coughs results in impairment in physical, social and psychological quality of life, including fatigue, exhaustion, chest pains, hernia, rib fractures, sleep disturbance, urinary incontinence in females and syncope in males [6, 53, 54]. Chronic cough significantly impacts work-life, with recent evidence showing increased time missed from work, absenteeism and increased sick days [55]. These provide reasons why patients with chronic cough might develop depressive symptoms and psychological distress. Some of these symptoms are captured in cough quality-of-life questionnaires such as the Leicester Cough Questionnaire and Cough-specific Quality of Life Questionnaire used in clinical trials and recommended in clinical practice [56, 57].
Personality traits do not directly and independently influence chronic cough, but the fact that personality traits independently predict depressive symptoms and psychological distress is well described, and provides some internal validity of the measurement tools used in the CLSA [58]. The nature of the relationship between personality and depression has been highly debated, with up to seven classical models described, divided into three groups. The first three (common cause, continuum/spectrum and precursor) suggest personality and depression are distinct but they arise from the same or similar aetiological processes. The fourth and fifth (predisposition and patho-plasticity) imply personality directly affects the onset or maintenance of depression. The sixth and seventh models (concomitant and consequences) reverse the direction of causality by suggesting depression has a causal influence on personality. These concepts consider traits to be stable, but other evidence suggests personality traits are dynamic and amenable to change [59]. Genetic factors do contribute to long-term stability, but life stressors and changes in relationships and work/social roles can also influence a change in personality traits [60]. In contrast, pathological trait trajectories can also be reversed by positive life experiences [61]. This is important because if depressive symptoms could lead to chronic cough, it would be important to further evaluate the mediating processes and potentially modifiable risk factors between personality traits and depression.
It was recognised as early as 1975 that bilingual speakers responded to the CESD-10 questionnaire differently because the interviewee and interviewer may understand colloquial expressions differently [62]. Similarly, studies have shown inconsistent evidence of validity and reliability in the K-10 psychological distress scale among culturally diverse groups. In the CLSA, we have previously reported an overall lower incidence of chronic cough in French speakers compared with English speakers [63]. This study also suggests that higher depression and psychological distress in French speakers does not significantly increase the risk of chronic cough. This could be due to lower numbers of French speaking participants with chronic cough, such that depressive symptoms and psychological distress have insufficient power to detect differences, or that language represents cultural norms, expectations, values and willingness to disclose information that can differ across English and French speaking cultures.
There are limitations to this study. First, depressive symptoms and psychological distress levels were assessed using questionnaires. Although these are validated for use in epidemiological studies, high scores may not always result in a clinical diagnosis of depression. Second, we currently do not have available complete analysable data on antidepressant medication use, which could help ascertain the clinical validity of the high depressive symptoms scores. Third, CESD-10 and K-10 have questions that relate to anxiety, but we have not analysed the independent effect of every item on the questionnaire as this was not the intended use of the questionnaires and cut-points for individual items are unknown. Fourth, the recall time period was different for each of the questionnaires: chronic cough was 12 months, depressive symptoms over the previous 1 week and psychological distress over the previous 4 weeks. These different time intervals could result in an inadequate representation of patient symptoms over a 3-year time period between baseline and follow-up 1 where scores may have changed over time, due to personal, social and work stressors. Such factors are unaccounted for. We decided to use a baseline exposure model to investigate chronic cough. We have not analysed the change in mental health scores between baseline and follow-up 1. It is possible that an individual may improve in their depressive symptoms or psychological distress scores after baseline and then develop chronic cough 3 years later. Fifth, this is an epidemiological study from the general community and not from a specialist cough clinic, hence these findings may not be generalisable to patients attending a chronic cough clinic. Furthermore, detailed information about cough severity, intensity and therapeutic interventions was not available. The limitation of studying the effects of mental health disorders in a cough clinic is that chronic cough has already occurred, and retrospectively assessing the effect of mental health and personality is extremely challenging. Only the impact of chronic cough on mental health over time can be assessed.
Conclusions
Personality traits of low emotional stability, conscientiousness, extraversion and openness to experiences increase the risk of mental health disorders and psychological distress, which independently increase the risk of developing chronic cough. However, chronic cough also increases the risk of developing depressive symptoms and psychological distress.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00119-2022.supplement
Acknowledgements
This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the CLSA is provided by the Government of Canada through the Canadian Institutes of Health Research under grant reference LSA 94473 and the Canada Foundation for Innovation as well as the following provinces: Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta and British Columbia. This research has been conducted using the CLSA dataset, Baseline and Follow-up 1 Comprehensive Dataset, under application number 1909024. The CLSA is led by Parminder Raina (McMaster University, Hamilton, ON, Canada), Christina Wolfson (McGill University, Montreal, QC, Canada) and Susan Kirkland (Dalhousie University, Halifax, NS, Canada). The opinions expressed in this article are the authors’ own and do not reflect the views of the CLSA. The final manuscript was reviewed and approved by the Publication Review Committee of the CLSA.
Footnotes
Provenance: Submitted article, peer reviewed.
Data availability: Data are available from the Canadian Longitudinal Study on Aging (www.clsa-elcv.ca) for researchers who meet the criteria for access to de-identified CLSA data.
Author contributions: P. Raina had full access to all of the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis. I. Satia, A.J. Mayhew, K.J. Killian, P.M. O'Byrne and P. Raina contributed substantially to the study concept and design. All authors made substantial contributions to the acquisition, analysis or interpretation of data for the manuscript. I. Satia, A.J. Mayhew and N. Sohel contributed substantially to drafting of the manuscript. All authors contributed to the critical revision of the manuscript for important intellectual content, final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of interest: I. Satia reports grants and personal fees from Merck during the conduct of the study; and grants and personal fees from GSK, personal fees from AstraZeneca and Genentech, grants from the E.J. Moran Campbell Early Career Award, and personal fees from Respiplus, outside the submitted work; he is an Associate Editor of this journal.
Conflict of interest: A.J. Mayhew has nothing to disclose.
Conflict of interest: N. Sohel has nothing to disclose.
Conflict of interest: O. Kurmi has nothing to disclose.
Conflict of interest: K.J. Killian has nothing to disclose.
Conflict of interest: P.M. O'Byrne reports grants and personal fees from AstraZeneca, personal fees from GSK, grants from Novartis, grants and personal fees from Medimmune, and personal fees from Chiesi, outside the submitted work.
Conflict of interest: P. Raina has nothing to disclose.
Support statement: This study was funded by Merck Canada as an investigator-initiated grant to I. Satia and P.M. O'Byrne. I. Satia is currently supported by the E.J. Moran Campbell Early Career Award (Dept of Medicine, McMaster University, Hamilton, ON, Canada). The study sponsor had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received March 2, 2022.
- Accepted March 24, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










