





Abstract
Objectives Pulmonary endarterectomy (PEA) is recommended for eligible patients with chronic thromboembolic pulmonary hypertension (CTEPH) and is potentially curative. However, persistent/recurrent CTEPH post-PEA can occur. Here we describe symptom and diagnostic assessment rates for residual disease post-PEA and longitudinal diagnostic patterns before and after riociguat approval for persistent/recurrent CTEPH after PEA.
Methods This US retrospective cohort study analysed MarketScan data (1 January 2002–30 September 2018) from patients who underwent PEA following a CTEPH/pulmonary hypertension (PH) claim with at least 730 days of continuous enrolment post-PEA. Data on pre-specified PH symptoms and the types and timings of diagnostic assessments were collected.
Results Of 103 patients (pre-riociguat approval, n=55; post-riociguat approval, n=48), residual PH symptoms >3 months after PEA were reported in 89% of patients. Overall, 89% of patients underwent one or more diagnostic tests (mean 4.6 tests/patient), most commonly echocardiography (84%), with only 5% of patients undergoing right heart catheterisation (RHC). In the post- versus pre-riociguat approval subgroup, assessments were more specific for CTEPH with an approximately two-fold increase in 6-min walk distance and N-terminal prohormone of brain natriuretic protein measurements and ventilation/perfusion scans, and a four-fold increase in RHCs.
Conclusions Low RHC rates suggest that many patients with PH symptoms post-PEA are not being referred for full diagnostic workup. Changes to longitudinal diagnostic patterns may indicate increased recognition of persistent/recurrent CTEPH post-PEA; however, there remains a need for greater awareness around the importance of continued follow-up for patients with residual PH symptoms post-PEA.
Abstract
Rates of residual PH symptoms are high after PEA but referral of patients with suspected persistent/recurrent CTEPH following PEA for CTEPH-specific diagnostic assessments is suboptimal, highlighting potential gaps in CTEPH patient care post-PEA https://bit.ly/3jfUZlO
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a progressive form of pulmonary hypertension (PH) characterised by organised thromboembolic material and vascular remodelling due to defective angiogenesis, impaired fibrinolysis and endothelial dysfunction, leading to right ventricular failure and ultimately death [1–4]. CTEPH is a complication of one or more episodes of pulmonary embolism (PE) [3]; however, ∼25% of patients do not present with a history of previous PE [5], although geographical differences have been noted in PE rates [4].
While the signs and symptoms of CTEPH are broadly similar to those of other forms of PH, such as pulmonary arterial hypertension, CTEPH is potentially curable with pulmonary endarterectomy (PEA) to remove the obstructive thrombofibrotic material [1]; however, up to 40% of patients are deemed inoperable or refuse surgery [6]. PEA is an intricate surgical technique requiring complex peri-procedural management and is therefore performed in specialised centres. It is associated with good outcomes, with low mortality rates reported in experienced centres, and improvements in haemodynamics and functional status [7, 8]. However, approximately one-third and up to one-half of patients may have some residual PH symptoms after surgery [7, 9], often the result of incomplete removal of proximal thrombotic material and/or small-vessel disease caused by vascular remodelling of the microscopic pulmonary arteries that is not amenable to PEA [2].
CTEPH is difficult to diagnose and remains an under-diagnosed condition [10]. The INFORM study (conducted 2010‒2011) retrospectively analysed data from a claims database and showed that 87% of patients had a claim for a PH-related symptom within 2 years following initial PE, but only 55% of patients had diagnostic procedural claims related to the identification of PH or CTEPH [11]. The INFORM study did not, however, investigate rates of persistent/recurrent CTEPH in the post-PEA setting.
Given the occurrence of persistent/recurrent CTEPH in patients undergoing PEA for CTEPH, we conducted a similar analysis to INFORM, to describe the number of diagnoses and symptoms related to PH, and the number of diagnostic tests used to assess the presence of CTEPH or PH symptoms in patients post-PEA to highlight any disconnect between patients showing signs of residual disease and receiving appropriate diagnostic assessments. During the data collection time period of this study (PEA conducted 2002–2016), the soluble guanylate cyclase stimulator riociguat was approved (October 2013 in the USA) as the first licensed medical therapy for use in patients with persistent/recurrent CTEPH after PEA [12]. Therefore, we also investigated whether the approval of riociguat and any concomitant changes in diagnostic options or disease awareness had an impact on the recognition of residual PH symptoms post-PEA.
Methods
Study design
This retrospective cohort study analysed data from the MarketScan Commercial Claims and Encounters Database and Medicare Supplemental and Coordination of Benefits Database (Truven Health Analytics). MarketScan captures longitudinal, individual-level administrative claims data, including inpatient and outpatient claims, outpatient prescription claims, clinical utilisation records and healthcare expenditures, from patients in the USA. All data collected in this study were de-identified to comply with data protection regulations and compliance with the Health Insurance Portability and Accountability Act of 1996 to preserve participant anonymity and confidentiality. Additional informed consent or institutional review board/ethical approval was not required. Patients were identified with specified inclusion/exclusion criteria between 1 January 2002 and 30 September 2016 (inclusive), with a follow-up period of up to 2 years following the index date until 30 September 2018 (supplementary figure S1). Adult patients aged 18 years or over who underwent PEA following a claim of PH or CTEPH with at least 730 days of continuous enrolment post-PEA were eligible for inclusion in the study. The index event was defined as the first claim related to PEA in eligible patients with a prior history of a claim of PH or CTEPH. Claims arising in the 3 months after PEA were excluded to account for symptoms resulting from the PEA index event or from immediate post-operative haemodynamic measurements. Claims were assessed based on codes from the 9th and 10th revisions of the International Classification of Diseases (ICD) and the current procedure terminology (CPT) for PH, CTEPH and PEA, as described in supplementary table S1.
Variables and end-points
Claims were assessed for 10 pre-specified PH symptoms: syncope, malaise and fatigue, dyspnoea, haemoptysis, chest pain (unspecified), dizziness, gait abnormality, cardiomegaly, ascites and peripheral oedema. Claims were also assessed for the following seven diagnostic tests: echocardiogram, computed tomography angiogram (CTA), pulmonary angiogram (PAG), right heart catheterisation (RHC), ventilation/perfusion (V′/Q′) scan, 6-min walk distance (6MWD) and measurement of N-terminal prohormone of brain natriuretic protein (NT-proBNP) levels. ICD and CPT codes for PH symptoms and diagnostic tests are shown in supplementary table S2 and table S3, respectively.
End-points assessed were the number and percentage of patients who underwent diagnostic assessments and/or had residual PH symptoms after the index date, after a 3-month wash-out period post-PEA. Thus, symptoms and diagnostic procedures occurring during the first 3 months post-PEA were excluded from the primary analysis to rule out symptoms arising from the PEA index event or during the immediate post-operative period. The number of diagnostic assessments and days from the index date to the earliest diagnostic assessment were also evaluated.
For the pre-specified time trends analysis, patients who underwent PEA between 1 January 2002 and 30 September 2013 (inclusive) were included in the pre-riociguat approval subgroup, and patients who underwent PEA between 1 October 2013 and 30 September 2016 (inclusive) were included in the post-riociguat approval subgroup. Subsequently, it was noted that for those patients who underwent PEA after 30 September 2011, the 730-day follow-up period included both the pre- and post-riociguat approval periods; consequently, post hoc these patients were excluded from the pre-riociguat approval subgroup and were incorporated into the post-riociguat approval subgroup.
Statistical methods
All analyses were descriptive in nature and no formal hypothesis testing was conducted. Univariate statistics were used to describe the study population for categorical and continuous variables. Rates of diagnostic assessments were performed in the overall population and in a subgroup of patients with at least one of 10 pre-specified PH symptoms, as described above, excluding a wash-out period of the first 3 months. Sensitivity analyses were conducted to assess the rate of these events without a wash-out period, or with 1- and 7-day wash-out periods.
Diagnostic assessment pathways were visualised using Sankey plots, calculated with R Studio version 3.6.3; only the first record for each assessment was used to construct the plots. Tests occurring on the same day were included in the same node of a pathway to provide an overview of the preferred assessment patterns.
No imputation of missing data was performed, and data analysis was conducted using SAS version 9.4 by using the SAS Macro algorithms developed by Bayer Global Data Analytics group (Whippany, NJ, USA).
Results
Study cohort
Of 182 286 926 patients in the MarketScan database, 103 met the analysis inclusion criteria (figure 1). Of 76 patients originally assigned to the pre-riociguat approval group (per-protocol), 21 patients were reassigned post hoc to the post-riociguat approval subgroup as their follow-up occurred after riociguat approval. Consequently, there were 55 patients in the pre-riociguat approval subgroup and 48 patients in the post-riociguat approval subgroups (figure 1).
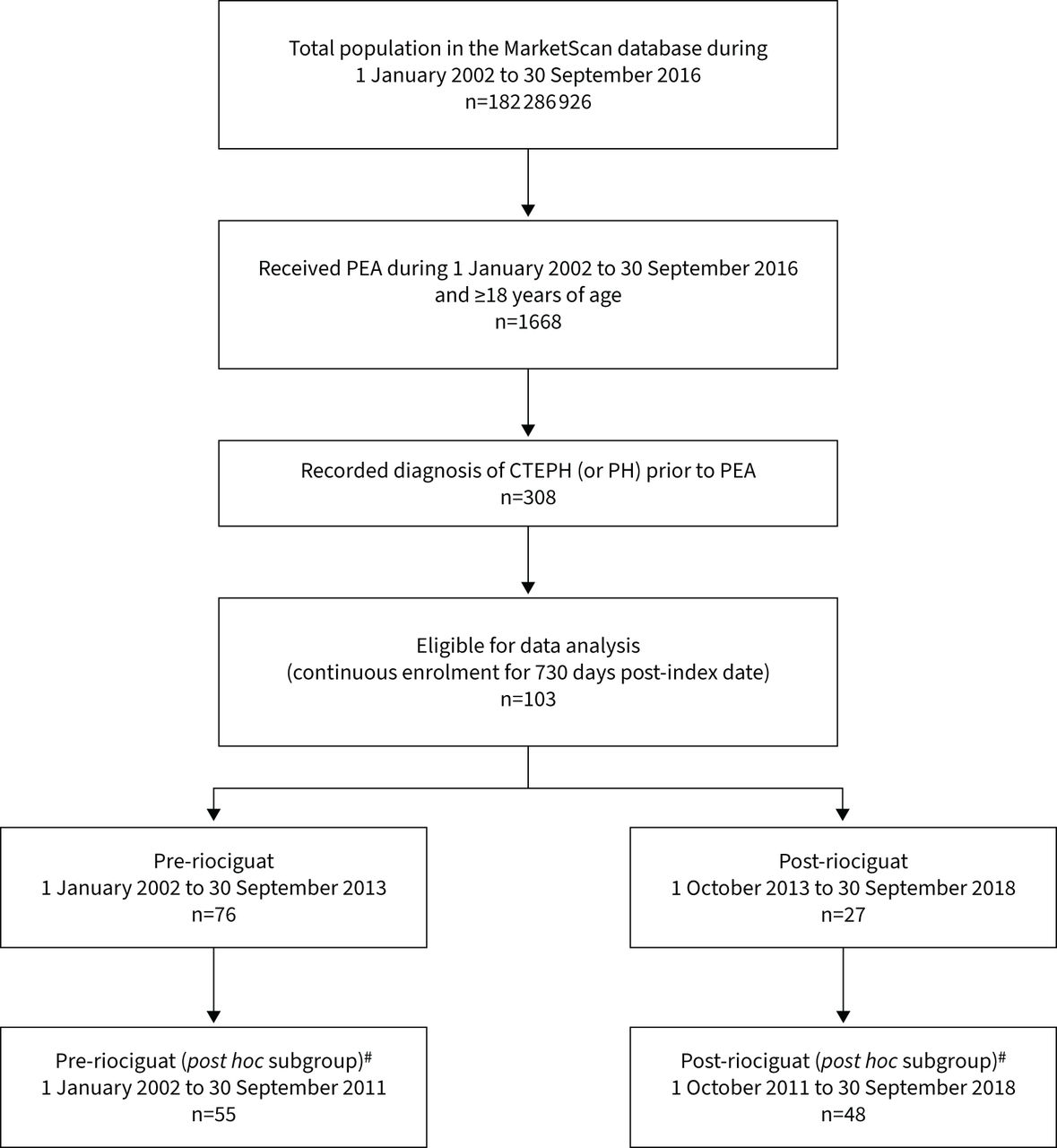
Flowchart of patient selection. #: post hoc defined subgroups, whereby 21 patients whose pulmonary endarterectomy (PEA) surgery occurred before the approval of riociguat in the USA but whose observation period extended beyond the riociguat approval date were reassigned from the pre-riociguat approval subgroup to the post-riociguat approval subgroup. A recorded diagnosis of chronic thromboembolic pulmonary hypertension (CTEPH) (or pulmonary hypertension (PH)) was not available in the MarketScan database for 1360 of the 1668 patients identified who underwent PEA.
In the overall population, mean age was 55.6 years and 59% of patients were male (table 1). Age and the Charlson comorbidity index score were similar in the post hoc defined pre-riociguat and post-riociguat approval subgroups, although there was a higher proportion of males (71% versus 49%) in the post- versus pre-riociguat approval subgroup (table 1). The demographic and clinical characteristics data for patients in the per-protocol pre- and post-approval subgroups are summarised in supplementary table S4.
Demographic and clinical characteristics in the overall population and in the subgroups defined post hoc according to completion of clinical assessment either pre- or post-riociguat approval
Residual symptoms of PH
Residual PH symptoms >3 months after PEA were reported in 92 patients (89%) in the overall cohort. The most common PH symptoms reported across the overall and post hoc pre- and post-riociguat approval groups were dyspnoea (range: 60–73%) and chest pain (unspecified) (range: 31–35%). Full details of PH symptoms relative to tests undertaken for the overall cohort and subgroups are provided in supplementary table S5. Rates of residual PH symptoms and diagnostic assessments occurring in the 2-year follow-up period, with varying exclusion periods, are shown in supplementary table S6.
Rates of diagnostic assessment
In total, 89% of patients (n=92) underwent one or more of the seven pre-specified tests for residual disease after PEA with a mean±sd of 4.6±3.8 diagnostic tests per patient (table 2). The mean±sd time from PEA (index date) to the first diagnostic test (after the 3-month wash-out period) was 183±100 days (table 2). Equivalent data for patients in the per-protocol pre- and post-riociguat approval subgroups are summarised in supplementary table S7. The majority of patients with PH symptoms (n=92) underwent at least one diagnostic assessment after the 3-month post-PEA wash-out period (n=84, 91%), with the most common assessment being echocardiography (n=80, 87%) (supplementary table S5).
Number of tests and days to the first diagnostic test after pulmonary endarterectomy (PEA) in the overall population, and in the post hoc defined pre-riociguat approval and post-riociguat approval subgroups
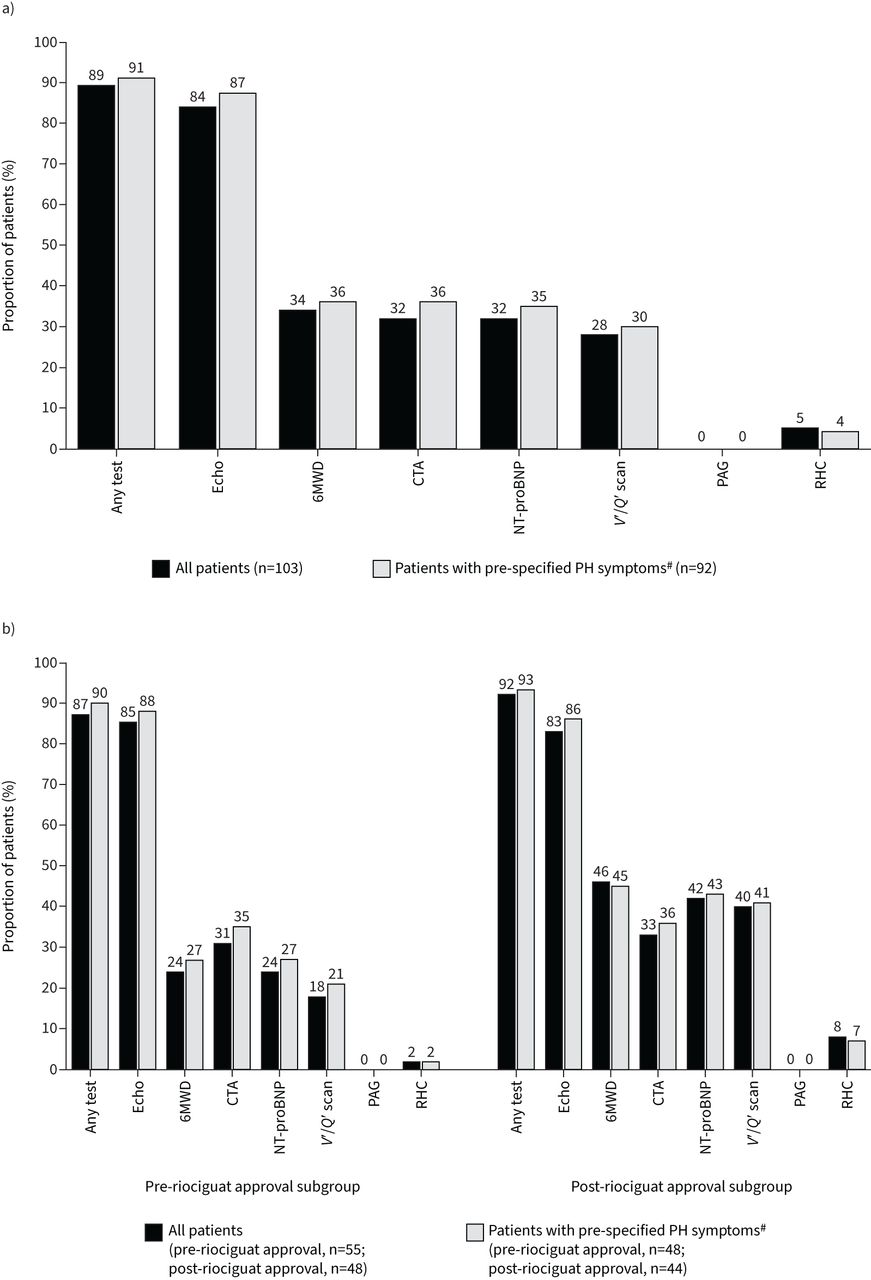
The most commonly performed assessment was echocardiography, which was undertaken in 84% of patients (n=87) with approximately one-third of all patients receiving CTA (32%; n=33) or a V′/Q′ scan (28%; n=29) or being assessed for NT-proBNP levels (32%; n=33) or 6MWD (34%; n=35) (figure 2a). Only 5% of patients (n=5) underwent RHC, and a PAG was not obtained for any patient. Echocardiography and 6MWD tended to be assessed first with a mean±sd of 222±128 and 221±148 days post-PEA, respectively, with RHC assessed last at 410±249 days post-PEA (table 2).
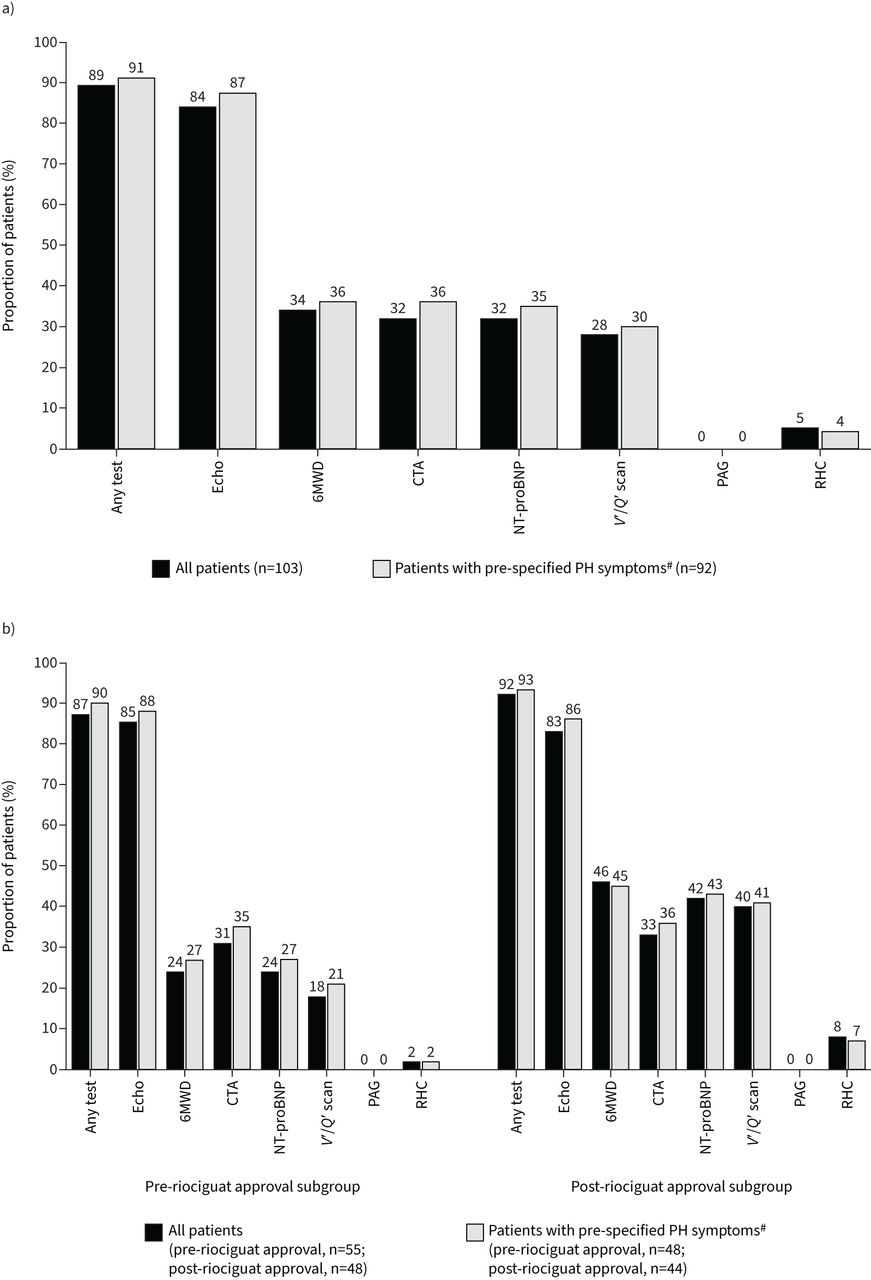
Rates of diagnostic assessment 2 years post-pulmonary endarterectomy for all patients and patients with pre-specified residual pulmonary hypertension symptoms a) in the overall population and b) in the post hoc defined pre-riociguat approval subgroup and post-riociguat approval subgroup (post hoc analysis including the 21 patients whose post-PEA observation period overlapped with the period following riociguat approval in the USA). 6MWD: 6-min walk distance; CTA: computed tomography angiogram; Echo: echocardiogram; NT-proBNP: N-terminal prohormone of brain natriuretic protein; PAG: pulmonary angiogram; RHC: right heart catheterisation; V′/Q′: ventilation/perfusion. #: syncope, malaise and fatigue, dyspnoea, haemoptysis, chest pain (unspecified), dizziness, gait abnormality, cardiomegaly, ascites and peripheral oedema.
The results of the wash-out period sensitivity analysis are shown in supplementary table S6. Of note, 71% of the patients with residual PH symptoms underwent RHC assessment when no wash-out period post-PEA was applied, with the percentage dropping to 36% when a wash-out of 1 day after PEA was applied, and further to 9% with a wash-out of 1 week and 5% with the pre-specified 3-month wash-out of the primary analysis.
An overview of assessment pathways followed for all patients is shown in a Sankey plot in figure 3a.

{kind=link}
{kind=link}
{kind=link}
Sankey plots illustrating diagnostic pathways a) in the overall patient population (n=103), b) in the post hoc defined pre-riociguat approval subgroup (n=55) and c) in the post-riociguat approval (n=48) subgroup (post hoc analysis including the 21 patients whose post-PEA observation period overlapped with the period following riociguat approval in the USA). The thickness of the bars indicates higher level of use of a particular diagnostic pathway. Nodes describing the simultaneous occurrences of two or more assessments were collapsed into a single node. 6MWD: 6-min walk distance; CTA: computed tomography angiogram; Echo: echocardiogram; NT-proBNP: N-terminal prohormone of brain natriuretic protein; RHC: right heart catheterisation.
Diagnostic assessment in the pre- versus post-riociguat approval subgroups
In the pre- and post-riociguat approval subgroups, 87% (n=48) and 92% (n=44) of patients underwent one or more of the pre-specified diagnostic assessments with a mean±sd number of tests of 3.8±2.3 and 5.4±4.8, respectively (figure 2b; table 2). The mean±sd time to first test was 197±118 days pre-riociguat approval and 167±76 days post-riociguat approval (table 2). For patients with pre-specified PH symptoms, 90% (n=43) and 93% (n=41) underwent one or more of the pre-specified diagnostic assessments in the pre- and post-riociguat approval subgroups, respectively (supplementary table S5). These findings are similar to the subgroups defined per-protocol (supplementary figure S2 and table S8) where 91% (n=61) and 92% (n=23) of patients in the pre- and post-riociguat approval subgroups, respectively, underwent one or more of the pre-specified diagnostic assessments.
Use of echocardiography, the most commonly used assessment, occurred at a similar rate in the post hoc pre- and post-riociguat approval subgroups (85% (n=47) and 83% (n=40), respectively; figure 2b). Numerical differences were observed between subgroups for the use of 6MWD, V′/Q′ scans and measurement of NT-proBNP levels with approximately twice as many patients undergoing these diagnostic tests in the post- versus pre-riociguat approval subgroup (figure 2b). The proportion of patients undergoing RHC also increased from 2% (n=1) in the pre-riociguat approval subgroup to 8% (n=4) in the post-riociguat approval subgroup, although the patient numbers were very low. No differences between pre- and post-riociguat approval subgroups were observed for the use of CTA (in 31% (n=17) and 33% (n=16) of patients, respectively). Overall, similar but less marked differences between the subgroups for diagnostic assessment utilisation were also observed in the per-protocol determined subgroups (supplementary figure S2 and table S8).
In the pre-riociguat approval subgroup, when not considering RHC due to the small number of patients undergoing this procedure, the earliest assessments performed were 6MWD (mean±sd time to first test: 174±101 days) followed by echocardiography (223±122 days) and CTA (224±128 days), while in the post-riociguat approval subgroup, the earliest assessments were measurement of NT-proBNP levels (205±107 days) then echocardiography (221±136 days) (table 2).
Increased use of diagnostic methodologies that are more specific for CTEPH was observed in the post- versus pre-riociguat approval subgroup when comparing the Sankey plots (figure 3b and c). Similar findings but with less marked subgroup differences were also observed in the per-protocol determined subgroups (supplementary figure S3a and b).
Discussion
In this retrospective cohort study, based on the format of the INFORM study [11], analysing MarketScan data from a 2-year period in patients who had undergone PEA following a claim of PH or CTEPH, rates of residual PH symptoms were high. Overall, 89% of patients had residual PH symptoms >3 months after PEA, most commonly dyspnoea reported in 66% of patients. Rates of diagnostic assessment that occurred >3 months after PEA were also high, with 89% and 91% of all patients and those experiencing residual PH symptoms, respectively, undergoing one or more assessment.
The majority (84%) of patients underwent echocardiography with approximately one-third of patients receiving CTA, a V′/Q′ scan and/or an assessment of 6MWD or NT-proBNP levels. The percentage of patients with residual PH symptoms who underwent RHC assessment was substantially reduced when a post-PEA wash-out period was applied, suggesting that the vast majority of patients who underwent RHC did so during the immediate post-operative period. This sensitivity analysis highlighted the importance of applying a 3-month wash-out period to ensure that the assessments occurred in response to subsequent residual symptoms of PH rather than the PEA index event. Overall rates of RHC were low, although they increased from 2% to 8% in the period post-riociguat approval, suggesting relatively few patients reporting residual PH symptoms were referred for full diagnostic workup despite European Society of Cardiology and the European Respiratory Society guidelines recommending at least one haemodynamic assessment 6–12 months after PEA [1]. The results of this study therefore suggest that the diagnostic follow-up of patients with residual PH symptoms post-PEA is suboptimal, indicating a need for increased awareness of the importance of continued management for patients with CTEPH-related symptoms following surgery.
In the longitudinal analysis of diagnostic pathways, our data suggested that there were implied differences in the assessment time and proportion of diagnostic tools used to assess patients post-PEA in the time periods before and after the approval of riociguat. Prior to riociguat approval, 6MWD assessments, echocardiography and CTA were among the earliest assessments provided, whereas post-riociguat approval the earliest assessments were measurement of NT-proBNP and echocardiography. When assessing the diagnostic pathway Sankey plots after an initial echocardiogram, most patients in the pre-riociguat approval subgroup received CTA or assessment of NT-proBNP, whereas most patients received CTA or a V′/Q′ scan in the post-riociguat approval subgroup. In the post-riociguat approval subgroup, a higher proportion of patients underwent many of the diagnostic tests, with twice as many patients undergoing a V′/Q′ scan and assessment of 6MWD and NT-proBNP levels. These data may suggest an increased awareness of specific CTEPH diagnostic procedures following the introduction of riociguat, which possibly reflects changes in the treatment landscape.
Limitations should be noted when assessing these data, including the small number of patients included in the analysis due to the limited number of eligible patients, particularly in the pre- and post-riociguat sub-analysis groups. It is also possible that comorbidities may have been responsible for the pre-specified symptoms in some patients. The use of diagnostic codes for PH may mean that some patients without CTEPH may have been included in the analysis, potentially resulting in an overestimation of the CTEPH population. The PH diagnostic code used as the CTEPH diagnostic code was only implemented on 1 October 2017, towards the end of our study. However, the combination of a code related to PH/CTEPH with a code related to PEA likely meant that the study population reflected the patients of interest. Two-component code-based algorithms have been demonstrated to have a higher positive predictive value than single-component algorithms for the identification of CTEPH [13]. The number of patients with confirmed residual CTEPH diagnoses by specific procedures and their continuation to further workup could also not be established due to limitations of the MarketScan database but may be useful to investigate in future using data from clinical practice and CTEPH registries. Furthermore, the MarketScan database is a convenience sample that may not represent the wider population of patients with CTEPH; for example, the database is skewed towards southern states of the USA [14, 15] and only includes patients with commercial insurance coverage. However, it should be noted that our data do reflect a diverse geographical and demographic US population due to the size and breadth of the MarketScan database. They may not, however, reflect other countries with different healthcare systems or reimbursement practices for diagnostic tests and treatments. It may be valuable for future studies, without the geographical limitations of the MarketScan database, to investigate whether differences in rates of symptoms or diagnostic assessments are impacted by a patient's location and distance from an expert centre for PEA. Finally, the temporal analysis with respect to riociguat approval may have missed other changes in the medical treatment landscape which could have influenced findings.
Conclusions
To conclude, low rates of RHC suggest that many patients showing signs or symptoms associated with persistent/recurrent CTEPH following PEA surgery are not being referred for full diagnostic workup. An increase in the use of specific diagnostic tests to assess persistent/recurrent CTEPH after PEA may indicate that awareness of CTEPH and understanding of disease diagnosis has increased in recent years, possibly due to the influence of an evolving treatment landscape following the approval of new medical therapies. Further research into real-world treatment patterns for persistent/recurrent CTEPH after PEA may increase awareness of undiagnosed and untreated residual disease, help healthcare professionals to recognise the potential gaps in care and raise awareness of the need for follow-up and screening for persistent/recurrent CTEPH after PEA.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00572-2021.SUPPLEMENT
Acknowledgements
Medical writing assistance was provided by Johanna Barry and Rachael Powis at Adelphi Communications Ltd (Bollington, UK), funded by Bayer AG (Berlin, Germany) in accordance with Good Publications Practice.
Footnotes
Provenance: Submitted article, peer reviewed.
Author contributions: All authors were involved in the concept and design of the study, analysis and interpretation of data, critical revision of the paper for important intellectual content, and gave final approval of the version to be published. S. Ju and K. Vogtländer were responsible for the statistical analysis. O. Butler supervised the study.
Conflict of interest: O. Butler is a current employee of Bayer AG.
Conflict of interest: S. Ju is a current employee of GlaxoSmithKline and was an employee of Bayer AG at the time of the submitted work.
Conflict of interest: S. Hoering is a current employee of Bayer AG.
Conflict of interest: K. Vogtländer is a current employee of Bayer AG.
Conflict of interest: S. Bansilal is a current employee of Bayer HealthCare Pharmaceuticals.
Conflict of interest: G.A. Heresi reports receiving advisory board fees from Bayer HealthCare and Janssen Pharmaceuticals, outside the submitted work.
Support statement: This study was funded by Bayer AG, Berlin, Germany, and Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received October 1, 2021.
- Accepted March 29, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










