





Abstract
Introduction Following the easing of COVID-19 restrictions in many countries, a surge in respiratory syncytial virus (RSV) hospitalisations was reported, surpassing yearly trends pre-pandemic. The changes to RSV epidemiology may have unforeseen effects on healthcare systems and populations globally, adding to the burden generated during the pandemic and placing increased demand on resources. Here we aim to identify recent global trends of RSV hospitalisation amongst children aged ≤5 years, to help inform policy makers in the planning of preventative interventions.
Methods We conducted a scoping review of published literature between January 2009 and May 2021. Using keywords “Hospital admissions, Respiratory syncytial virus, RSV, Bronchiolitis, Children” we located studies using Medline, EMCARE, CINAHL and HMIC. Studies were eligible if they reported on trends/data for RSV hospitalisation amongst children aged ≤5 years. The articles were reviewed by two independent reviewers.
Findings We assessed 3310 abstracts, reviewed 70 studies and included 56 studies in the final review. Findings were categorised into themes. The review highlighted that, although RSV incidence has been steadily increasing since 2009, the number of reported RSV hospitalisations decreased during lockdown. The highest numbers of hospitalisations were reported in children <1 year of age, particularly 0–2-month-old infants. Globally, RSV hospitalisations tend to peak in the winter months; however, since COVID-19 restrictions have eased, countries are reporting incidence peaks at different times, in contrast to the trends of previous years.
Conclusion With greater physical interactions due to the relaxation of COVID-19 restriction measures, RSV-related hospitalisations can be seen to increase amongst children aged ≤5 years, possibly surpassing the numbers reported in previous RSV seasons.
Abstract
With #COVID19 restriction measures being eased globally, #RSV-related hospitalisation among children will increase, possibly surpassing pre-pandemic levels https://bit.ly/35lg4Iv
Introduction
Respiratory syncytial virus (RSV) is an enveloped RNA virus which causes acute lower respiratory infections (ALRI) and bronchiolitis in young children [1] and is responsible for >3 million hospitalisations and over 65 000 deaths globally each year [2]. Although over 80% of infants have experienced at least one RSV infection by the age of 2 years, infants in their first year of life are more likely to experience a severe infection requiring hospitalisation [3]. RSV-related complications other than bronchiolitis include pneumonia, acute otitis media and conjunctivitis [4]. Despite over 50 years of effort, a licensed vaccine is still not available for RSV [5].
RSV is known to create a significant burden on healthcare systems. A systematic review and meta-analysis of 329 studies conducted by Shi et al. in 2017 [6] estimated that there were about 33.1 million (uncertainty range (UR) 21.6–50.3) RSV-ALRI episodes globally, resulting in about 3.2 (UR 2.7–3.8) million hospital admissions and 59 600 (48 000–74 500) in-hospital deaths in (670.5 million) children younger than 5 years. In the UK alone, 450 000 general practitioner (GP) appointments, 29 000 hospitalisations and 83 deaths per year are reported amongst children and are attributed to RSV infection – with the majority of the burden reported in infants [6]. In England, it has been estimated that RSV causes ∼78% (95% CI 75%–83%) of bronchiolitis admissions in children <5 years of age [7]. Reeves et al. (2017) [8] confirm a mean annual admission rate of 35.1 (95% CI 32.9–38.9) per 1000 children aged <1 year and 5.31 (95% CI 4.5–6.6) per 1000 children aged 1–4 years in England when analysing data from 2007 to 2012. Shi et al. (2017) [6] report that direct medical costs associated with hospital care for childhood ALRI have been estimated to range from USD 243 (95% CI 154–341) to USD 559 (269–887) at secondary and tertiary care facilities, respectively, in low- to middle-income countries; and USD 2804 (2001–3683) to USS 7037 (4286–11 311) at secondary and tertiary care facilities, respectively, in high-income countries. These data highlight the importance of managing RSV-related illness in the UK and globally during the pandemic. Furthermore, it is important to consider the direct effects that sociological and economical changes attributable to COVID-19 may have on the epidemiology of RSV in the short, medium and long term. As a result of changes in infection rates and contact patterns, it is likely that levels of immunity in the population are not reflective of recent years. Failure to consider these effects could have an impact on populations and healthcare systems both in the UK and globally.
Throughout much of 2020 and 2021, non-pharmaceutical interventions (NPIs), including physical distancing, reduced social mixing and quarantine measures, were implemented worldwide to limit the spread of SARS-CoV-2. Hygiene measures were also introduced to reduce viral transmission, including the use of face masks, with governments delivering campaigns with the aim of increasing hand hygiene. This was the first time in many years that such dramatic changes to sociological and behavioural dynamics had occurred, leading to changes in the epidemiology of other communicable diseases [9]. Following a nationwide lockdown in 2020, Finland reported a decrease in paediatric hospital admissions caused by respiratory tract infections [10]. The initial trajectory of the RSV season itself was similar to that of previous years; however, 1 week after the start of lockdown, case numbers decreased rapidly, attributed to reduced social mixing and mobility [10].
The changes in RSV epidemiology may have unforeseen effects on healthcare systems and populations globally, adding to the burden generated during the pandemic and placing increased demand on resources. A recent study in Australia highlighted the potential implications of easing COVID-19-related restrictions on numbers of RSV hospitalisations. In Western Australia, RSV case numbers started to increase once physical distancing measures were relaxed, exceeding the seasonal peak reported in the previous eight RSV seasons [11]. A change in the temporal dynamics of RSV was also reported, with the season occurring during spring and summer instead of the winter months [11]. A study in the USA also demonstrated an absence of their usual RSV season during state-wide lockdowns and a delayed resurgence in cases and hospitalisations [12].
The primary objective of this scoping review is to identify and gain insight into the recent trends of RSV-associated hospitalisations globally. Secondary objectives include assessing the impact of the following measures on RSV hospitalisation:
COVID-19 lockdown
Relaxation of COVID-19 restrictions
Methods
A scoping literature review was conducted by two reviewers (M.N. and R.K.). All shortlisted studies were entered into a Microsoft Excel table and shared with the other authors of this article.
Literature search strategy
Key terms including “Hospital admissions, Respiratory syncytial virus, RSV, Bronchiolitis, Children” were searched using Medline, EMCARE, CINAHL and HMIC.
The inclusion criteria were:
Primary and secondary research assessing/reporting RSV illness and hospitalisation globally
Published 2009 onwards
Age group ≤5 years
The exclusion criteria were:
Published 2009 onwards but utilised data from before 2009
Impact assessments of medication/antibiotics/vaccines
Reporting clinical outcomes for RSV patients
Evaluated RSV-related cost of hospitalisation
The shortlisted literature was then categorised into three groups: 1) trends in RSV-associated hospitalisation; 2) seasonality of RSV hospitalisation; and 3) incidence/prevalence of RSV infection. Trends in RSV-associated hospitalisation were further grouped into three themes: i) increase in incidence/rate over time; ii) patient age at time of RSV hospitalisation; and iii) impact of COVID-19 restrictions on number of RSV hospitalisations.
Findings
The literature search located 3310 papers, of which 56 were shortlisted for further review and 56 studies were included in the final review. The studies included in the review are presented in tables 1 and 2. Data, where extractable, have been plotted as figure 1 (RSV incidence) and figure 2 (RSV hospitalisations).
Studies on respiratory syncytial virus (RSV)-associated hospital admissions
Studies on the seasonality of respiratory syncytial virus (RSV) hospitalisation
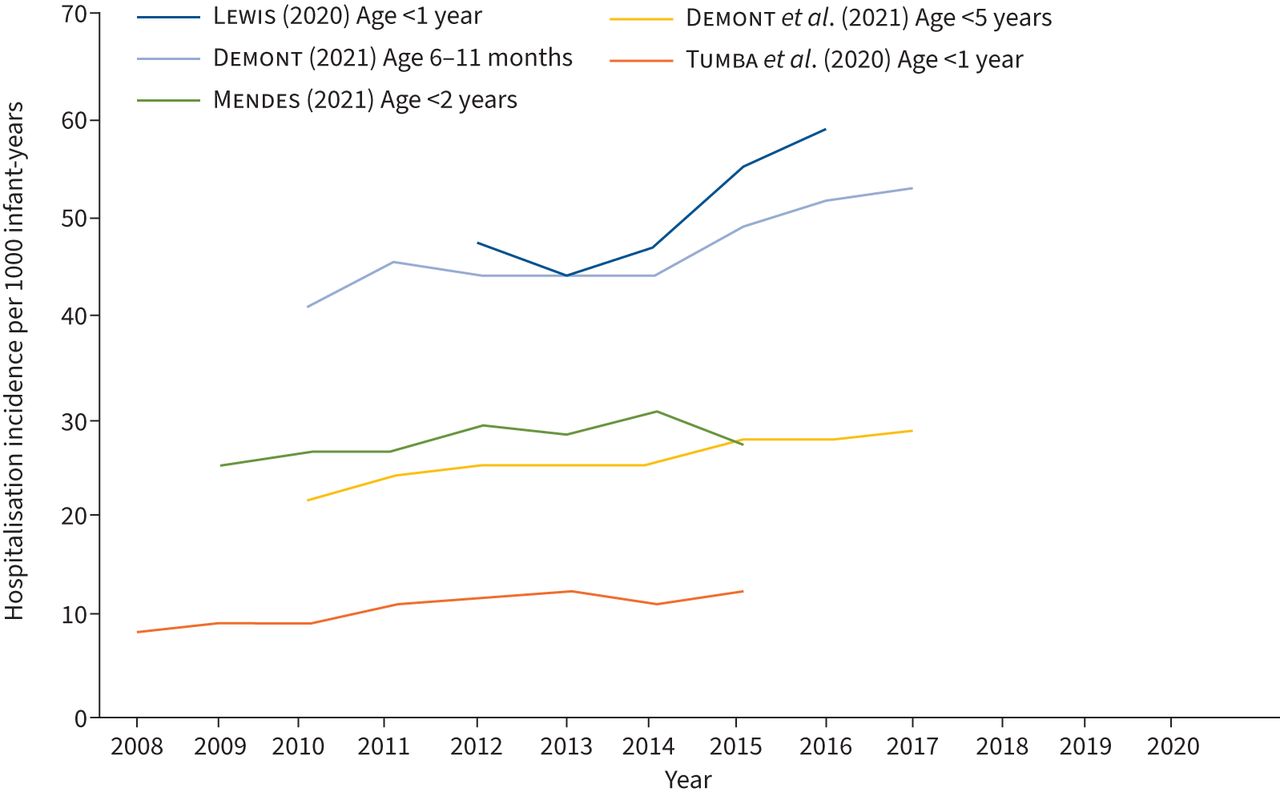
Respiratory syncytial virus (RSV) hospitalisation incidence per 1000 infant-years, from 2008 onwards.

{kind=link}
{kind=link}
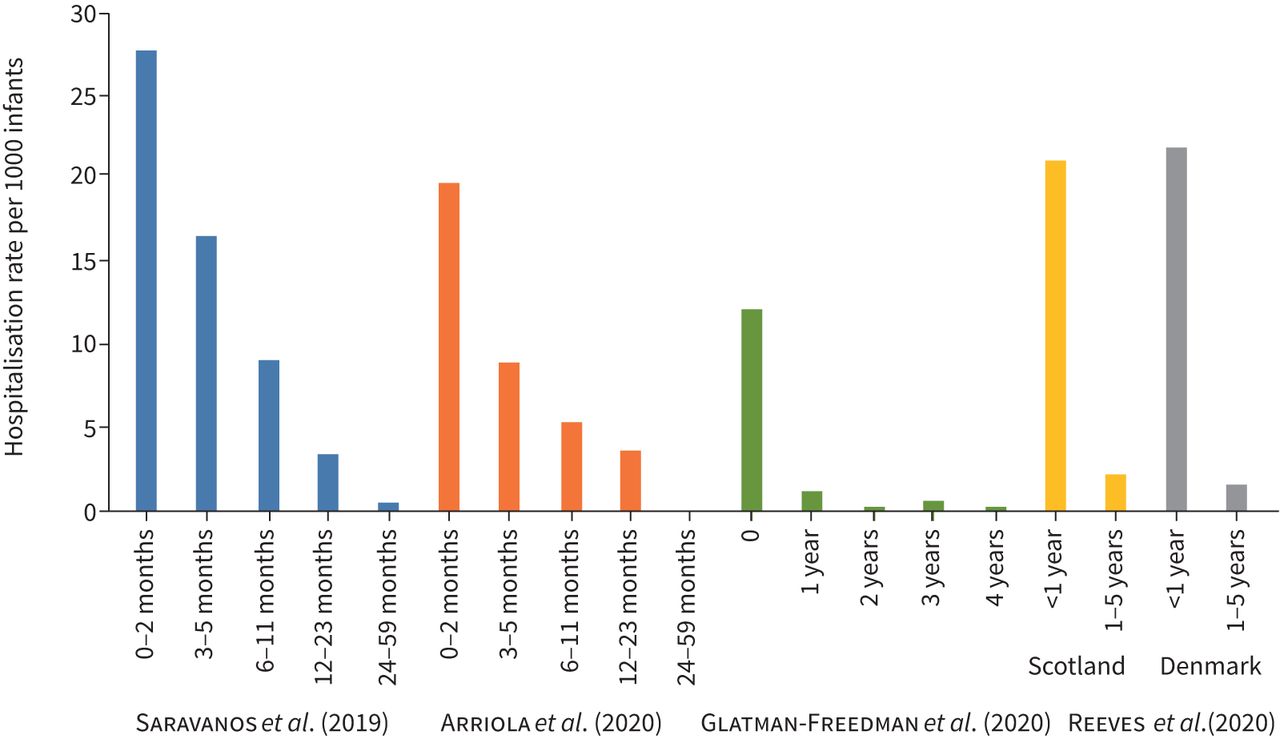
Annual respiratory syncytial virus (RSV)-associated hospitalisation rate per 1000 infants, broken down by age. Please note that the age group brackets of the included studies differ.
RSV-associated hospital admissions (table 1, figure 1)
Increase in incidence/rate over time
We found evidence that the number of infant RSV hospital admissions has been increasing in recent years across the world before the COVID-19 pandemic, with several studies reporting a year-on-year increase in RSV hospitalisations from 2004 [7, 13, 14] (figure 1). Approximately 80% of hospitalised bronchiolitis cases among children under 1 year in England are attributable to RSV [15] (table 1). Lewis et al. (2020) [16] documented the increased bronchiolitis admission rate in England from 47.4 (95% CI 46.8–47.9) to 58.9 per 1000 infant-years (95% CI 58.3–59.5) between 2012 and 2016. A study by Tumba et al. (2020) [14] reported a 49% increase in the incidence of hospitalisation for bronchiolitis in Brazil between January 2008 and December 2015 (8.5 to 12.7 per 1000 infant-years), with RSV attributed as the aetiologic factor. Chung et al. (2020) [7] conducted a 15-year longitudinal study (2001–2016) of RSV admission rates for children under 2 years of age in Scotland and found a 2.20-fold increase (95% CI 1.4–3.6-fold) from 17.2 (15.9–18.5) to 37.7 (37.4–38.1) admissions per 1000 infant-years [7]. A French study by Demont et al. (2021) [17] investigating the economic burden of RSV hospitalisations found that incidence of RSV hospitalisations in under 5s increased from 21.96 to 28.8 per 1000 infant-years between 2010 and 2018. However, the absence of an increased number of RSV cases during the 2020 season is likely attributable to external factors, such as the SARS-CoV-2 pandemic and subsequent behavioural and sociological shifts due to NPIs.
Age at time of RSV hospitalisation (figure 2)
Several studies have confirmed an increase in RSV hospitalisations with a decrease in patient age, with infants <1 year old having the highest burden of RSV hospitalisations, with admissions peaking for those below 2 months of age [18–23] (figure 2). Reeves et al. (2020) [22] found the mean annual RSV-coded admission rates ranged from 20.5 to 22.3 per 1000 children aged <1 year in Scotland, Finland, Norway and Denmark, as compared with a range of 1.25 to 2.24 per 1000 children in children aged 1–4 years. Arriola et al. (2020) [18] reported similar findings with the adjusted age-specific RSV hospitalisation rates per 1000 population being 19.7 (95% CI 17.87–21.77), 8.97 (95% CI 7.61–10.73), 5.31 (95% CI 4.59–6.24) and 3.58 (95% CI 3.17–4.05) for ages 0–2, 3–5, 6–11 and 12–23 months, respectively. Saravanos et al. (2019) [19] also found that the highest RSV hospitalisation rate was for infants aged <2 months (27.78 per 1000 population). Glatman-Freedman et al.’s (2020) [20] study in Israel concurred with the other studies, with hospitalisation load of RSV-related diagnoses reported as highest in infants <1 year of age (mean yearly rate of 12.18 per 1000 infants), rapidly declining in the following years. According to Hardelid et al. (2019) [21], the overall RSV admission rate in the first, second and third year of life was 21.9, 7.0 and 2.0 per 1000 infant-years, respectively, indicating a clear reduction in hospitalisation with age. Demont et al. (2021) [17] found that the most burdened age group in terms of RSV hospitalisation was aged <1 year, representing 69% of hospitalisations. Incidence of RSV hospitalisations in this population increased from 0.52 to 0.74 per 1000 infant-years between 2010 and 2018 and was significantly higher than in other age groups.
Impact of COVID-19 restrictions on RSV
Three of the studies conducted during the COVID-19 pandemic confirmed a change in RSV hospitalisation dynamics during periods of NPI, as compared with previous years [24–26]. Pelletier et al. (2020) [24] demonstrated a decrease in the number of RSV hospital admissions in the USA beginning in March 2020 compared with the period from 2010 to 2019. In April 2020, hospital admissions were reduced by 45.4% compared with previous years (23 798 in April 2020 compared with a median (interquartile range) of 43 550 (42 110–43 946) in April 2010–2019). An Australian study conducted by Britton et al. (2020) [25] observed a reduced mean frequency of RSV detections between April and June 2020, which was 94.3% lower than predicted based on 2015–2019 data (mean±se 99±24; p=0.026). Furthermore, Wilder et al. (2020) [26] found that the mean number of bronchiolitis admissions was lower in the COVID-19 cohort than the pre-COVID-19 cohort (1 versus 7; p=0.008). A retrospective analysis of the sentinel surveillance system for viruses in Austria by Redlberger-Fritz et al. (2021) [27] also confirmed a rapid reduction in RSV prevalence, a week after national lockdown measures were imposed in Austria in March 2020. The study confirmed 19 RSV detections after lockdown compared to 82 (95% CI 65−104) (p<0.001) detections observed in the equivalent period during the previous seasons [27]. Together, these studies suggest an association between the introduction of COVID-19 social distancing and lockdown measures and a reduction in burden of RSV hospitalisations amongst infants.
Seasonality of RSV infections (table 2)
A global study by Pangesti et al. (2019) [28] established that generally in temperate countries located in the Northern and Southern hemispheres, a peak of RSV admissions occurs in winter months, while in subtropical and tropical countries, admissions peak mostly during the rainy season. The results of a 17-year Israeli study by Glatman-Freedman et al. (2020) [20] reported that RSV-related hospitalisations followed a clear seasonal pattern, in which the peak occurred in January for 14 seasons, in December for two seasons (2014/2015 and 2015/2016) and in February for one season (2004/2005). In India, Broor et al. [29] observed RSV detection to peak in winter (November–February) and in rainy seasons.
Three studies in the UK produced similar findings, with a peak in admissions seen in infants born during the winter months of September to December [7, 15, 16]. Reeves et al. (2019) [30] found that RSV-associated admissions peaked in infants born in September to November. Similarly, Chung et al. (2020) [7] found that RSV admissions peaked in infants born in the 3 months preceding December, the month when cases of bronchiolitis are highest. Across the Clinical Commissioning Groups in England, Lewis et al. (2020) [16] found there was a 5.3-fold variation in incidence with area-level deprivation and the epidemic peak ranged from week 49.3 to 52.2. A study by Glick et al. (2020) [31], comparing paediatric RSV hospitalisations with regional RSV activity in the USA, produced similar findings to the British studies and confirmed that the mean RSV hospitalisation season fell in early November.
Furthermore, in the study by Reeves et al. (2020) [22], biennial peaks were seen in RSV-coded admission rates for Finland, Norway and Denmark, with a higher admission rate one year followed by a lower rate in the next. This shows a clear pattern of seasonality within RSV that should enable a country to predict the approximate timeframe in which an increased number of infections and hospitalisations might occur.
Discussion
This scoping review provides an overview of the global trends in RSV-associated detections and hospitalisations reported in the literature since 2009 to present. RSV hospitalisations have been widely studied, given the impact on infant mortality and financial burden on healthcare systems. We located studies from Mali, Nicaragua, Philippines, Spain, England, Israel, Hong Kong, Austria, USA and beyond to inform trends amongst individuals from diverse and varied socioeconomic backgrounds.
The results of our review indicate that the incidence of RSV hospitalisations has been increasing longitudinally and that the highest number of hospitalisations is reported in 0–2-month-old infants. Green et al. (2016) [13] suggest that the general increase in bronchiolitis admissions may not be due to changes in the severity or transmissibility of RSV but to changes to healthcare; changes in healthcare policies such as admission thresholds, as well as an increase in hospital bed availability, have been suggested as drivers of the increase, rather than a true increase in incidence. Tumba et al. (2020) [14] suggest that the increase is down to external factors, speculating that the increase in bronchiolitis hospitalisations seen in Brazilian children could be due to an increase in caesarean sections being performed, prematurity rates and increased urbanisation. Premature babies are prone to developing incomplete lung function and are more susceptible to respiratory problems [14]. Nenna et al. (2017) [32] found both indoor and outdoor pollution to be risk factors for acute bronchiolitis in infants aged <3 years old. In addition, a study by Robledo-Aceves et al. (2018) [33] showed that neonatal infection with other respiratory viruses, including rhinovirus, were risk factors for bronchiolitis. Hardelid et al. (2019) [21] reported premature birth, having older siblings, maternal age <30, low socioeconomic status and delayed infant vaccination as risk factors significantly associated with increased RSV hospitalisation. Additionally, Carbonell et al. (2012) [34] found that male sex, tobacco smoking while pregnant, month of birth, duration of breastfeeding, number of siblings at school and number of smokers in a household all contributed to the risk of RSV hospitalisation amongst infants. Similar risk factors were associated with the need for mechanical ventilation and supplemental oxygen in a prospective cohort study of 299 RSV-positive infants admitted to the Alder Hey Children's Hospital, Liverpool [35].
We also found some evidence for an association between socioeconomic status, deprivation and RSV admissions; early RSV epidemic peaks have been associated with areas of higher population densities, such as London and Manchester in England [15] and in Scotland [7].
The reduction in RSV-associated hospitalisations during the COVID-19 pandemic can possibly be attributed to the implementation of public health interventions to prevent or reduce the transmission of SARS-CoV-2 [25–27, 36]. Handwashing and isolation are known effective measures against nosocomial RSV transmission. A very high uptake (>84%) of enhanced hygiene and physical distancing measures could explain the large reduction in RSV incidence and hospitalisation reported in Australia in March 2020 [25]. Significant reductions in other diseases associated with social distancing measures were also reported, e.g. in overall hospitalisations for bronchiolitis, pneumonia and asthma during the initial SARS-CoV-2 outbreak, compared with the same calendar period in the 4 previous years [26]. By contrast, there was no change in hospitalisations for those conditions, such as cellulitis, gastroesophageal reflux disease and urinary tract infection, not known to be associated with viral infections and social distancing measures [26].
Chung et al.'s (2020) [7] study of bronchiolitis amongst children under 2 years of age in Scotland concluded that the increase in bronchiolitis admissions may be due to similar factors which have contributed to an increase in all paediatric hospital admissions in Scotland: infants attending day-care at younger age (resulting in an earlier exposure to pathogens); a decrease in out-of-hours care availability due to changes of GP practice contracts; and changes in parental expectations of treatment. Given the varying healthcare and social systems across the globe, these reasons might not be generalisable elsewhere but do provide potential insights.
Redlberger-Fritz et al. (2021) [27] state that the Austrian national lockdown led to 70% reduction of mobility and had a significant impact on the prevalence of respiratory viruses in Austria, including RSV. The study also cites Belingheri et al. (2020) [36] confirming that lockdown measures led to a reduction in epidemic diseases of childhood in Italy, including chickenpox, rubella, pertussis and measles. The reductions are attributed to the forced lockdown, closure of schools and public meeting places and the intensive use of masks in the general population leading to a reduction in inhalation of airborne respiratory droplets [36]. The study also highlights that a reduction in viral diseases during the pandemic could be a result of a decrease in individuals visiting emergency departments due to the fear of being infected at the hospital [36]. However, the global reduction in RSV hospitalisations of such a magnitude cannot be solely attributed to individuals avoiding emergency care. Hence, one can conclude that the preventative measures in place for COVID-19 also curbed the transmission of other viral diseases, including RSV.
Our findings suggest that there is a distinct seasonal pattern to RSV incidence and RSV hospitalisations, with a peak in RSV infections observed during the winter in temperate regions; however, there is no general agreement as to why this occurs. It has been suggested that this may be due to a link between temperature and RSV infection [37], or the inhalation of the air in cold temperatures causing nasal passages to cool thus inhibiting their respiratory defence [38]. However, it has also been argued that the seasonal peaks of RSV are associated with higher environmental temperature [39] or the crowding of susceptible individuals indoors during cold winter weather leading to greater transmission of respiratory viruses [40]. Relative humidity and rainfall have also been suggested to affect RSV activity [37, 39, 41].
Having older siblings at nursery or school has also been identified to increase the risk of RSV hospitalisation. Attending closed settings outside of the home increases infection risks through greater contact with other children [21, 42].
This review has a number of limitations. Since this is a scoping review, the literature search may have missed some relevant publications within grey literature and articles from the Cochrane Library that might encompass further eligible studies. We also could not provide cumulative means for the trends in hospitalisations as we were unable to extract data from all the studies. None of the eligible studies were critically appraised and might include biases owing to respective study designs, definitions and sources of data. Definitions for hospitalisation may vary from study to study and among countries. We also have not grouped the studies/findings based on low-, middle- and high-income countries.
Conclusion
Evidence strongly suggests that RSV hospitalisation amongst children aged ≤5 years has increased in the past decade and follows a distinct seasonal pattern. The highest number of hospitalisations was reported in the 0–2-month-old age group. When comparing the <1-year-old age group with the 1–5-year-old group, hospitalisations were considerably higher in the infants <1 year old. RSV hospitalisation rates decreased with the introduction of social distancing measures; in some cases a reduction of up to 94.3% as compared with previous years has been reported. As countries have begun to lift restrictions, emerging reports of spikes in RSV hospitalisations from Australia, Austria and the UK are concerning. Countries have also reported out of season spikes, with the southern states of the USA reporting a spike in the summer months of 2021, at variance with the predictable seasonality of RSV in the Northern Hemisphere. Furthermore, with older siblings returning to school, infants born during lockdowns, particularly those born prematurely, will be highly prone to contracting RSV from their siblings. Further research is required to understand the changes in the epidemiology of RSV due to waves of COVID-19 restrictions and subsequent easements to support planning for increased demands on often already overburdened paediatric intensive care and medical services.
Acknowledgements
We would like to extend our gratitude to our colleagues at the UK Health Security Agency: Hannah Williams and Joseph Shingleton for providing valuable advice on the search strategy, and Thomas Finnie and Andre Charlett for reviewing the final draft of the paper.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: The authors have nothing to disclose.
- Received October 19, 2021.
- Accepted March 22, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










