





Abstract
Study question Is there a difference in the number of repetitions in the 1-minute sit-to-stand (1MSTS) test using an individually adapted seat height to 90° knee flexion (1MSTSIND), compared with the commonly used standard chair seat height of 46 cm (1MSTSSTD), in people with COPD?
Methods We conducted a single-centre, single-blinded, randomised crossover trial in people with COPD between August 2020 and March 2021 at a specialised rehabilitation clinic in Switzerland. After a learning 1MSTS test, all participants performed two 1MSTS tests in random order on consecutive days. Participants were blinded, as they did not receive detailed information on the testing protocols.
Results 49 individuals with COPD (47% female) participated. In a regression model adjusted for sequence period and subject, 1MSTS test performance was lower on 1MSTSIND compared to 1MSTSSTD (−0.78 repetitions, 95% CI −1.47 to −0.11). In a second regression model additionally including the knee angle and an interaction term (1MSTSIND×knee angle), the interaction term was significant: 0.18 (95% CI 0.05 to 0.30). The limits of agreement were between −5.5 and 4 repetitions.
Conclusion Although we observed a statistically significant difference between 1MSTSIND and 1MSTSSTD on a population level, the difference is negligible. Further studies may be needed to determine whether individual adaptation of seat height is needed for very tall or short people to ensure a valid assessment of 1MSTS test performance in COPD.
Abstract
Performing the 1MSTS test on an individually adjusted chair versus a standard chair results in fewer repetitions (mean difference −0.78, 95% CI −1.47 to −0.11). However, the difference in repetitions is clinically negligible. https://bit.ly/3Oc8Rvp
Introduction
Evaluation of functional exercise capacity of people with COPD is a cornerstone of pulmonary rehabilitation programmes [1]. In recent years, the 1-min sit-to-stand (1MSTS) test has gained increasing interest among clinicians and researchers [2, 3]. It is a simple, valid, reliable and responsive exercise test in people with COPD [4], and a strong predictor of 2-year mortality [5].
The 1MSTS is commonly performed using a chair with a seat height of 46–48 cm [4–10]. However, using a standard seat height for all individuals – irrespective of their body height – may lead to invalid estimates of functional exercise capacity. Taller people are potentially disadvantaged, because they need to cover a greater distance during the sit-to-stand (STS) movement, whereas shorter people may have an advantage resulting in better performance [11–14]. Previous work on determinants of STS performance revealed that seat height (among other factors such as the use of armrests and foot position) influence STS performance [12, 15, 16]. In elderly people, seat heights between 80 and 120% of an individual's leg length revealed a tendency towards reduced quickness and force production in the phases of trunk flexion and knee and hip joint extension [16], suggesting that individual adaptation of seat height is necessary when performing STS tests [12, 16].
To date, the impact of an individually adjusted seat height versus standard seat height on 1MSTS test performance in COPD is unknown. This study aimed to evaluate the impact of an individually adapted seat height to 90° knee flexion (1MSTSIND) compared to the commonly used seat height of 46 cm (1MSTSSTD) on 1MSTS test performance in people with COPD.
We hypothesised that taller people perform more STS repetitions when performing the test on a higher 1MSTSIND than on the lower 1MSTSSTD, whereas shorter people perform fewer STS repetitions on 1MSTSIND than on the higher 1MSTSSTD.
Methods
Study subjects
Participants were recruited at the Berner Reha Zentrum AG in Bern, Switzerland. They were included in this study if they had a diagnosis of COPD and a forced expiratory volume in 1 s (FEV1) / forced vital capacity (FVC) ratio below the lower limit of normal [17, 18]. We excluded participants who 1) were not able to bend their knee at least 90° while sitting on a standard chair; 2) did not understand the test instructions, either because of language or for cognitive reasons; 3) were unable to perform the 1MSTS test due to functional disability (i.e. not being able to stand up from a chair without hand support); 4) had a previous surgery or reported pain that would interfere with the performance of the 1MSTS, as judged by the responsible physician. All participants provided written informed consent, after they were given at least 24 h to decide [19]. The recruitment was performed consecutively between August 2020 and March 2021. The study protocol was approved by the Cantonal Ethics Committee Bern (BASEC-ID 2020-01677), and the study was registered at www.ClinicalTrials.gov (NCT04579055).
Study design
We conducted a single-centre, single-blinded, randomised crossover trial. All assessments were performed during the inpatient pulmonary rehabilitation and were carried out by the same investigator.
First, a 1MSTS familiarisation test (1MSTSTEST) was performed, followed by the randomisation process. Participants were not informed about the randomisation result, and they did not receive any further information about the testing protocol. After randomisation, each participant performed two 1MSTS tests in random order on two consecutive days at the same time of day. We scheduled the study visits to ensure that the participants had at least 1 h rest before the examination.
Randomisation and masking
A computer-generated list of random numbers was created by an external biostatistician using the R package “blockrand” [20] and implemented into the database by a person who was not involved in the recruitment process. The randomisation of chair order (1MSTSSTD then 1MSTSIND, or vice versa) was stratified by type of seat height adjustment: 1) lower seat height (knee angle <89°), 2) standard seat height (knee angle 89–91°) or 3) higher individual seat height (knee angle >91°). Randomisation was performed within REDCap (Research Electronic Data Capture, Vanderbilt University, USA) [21], hosted by Berner Reha Zentrum AG. We were able to mask participants because the investigator prepared the chair height for the 1MSTS tests before the study visits.
Measurements and test procedure
Leg length
Leg length, defined as the length from the great trochanter of the femur to the malleolus lateralis, was measured while the participant was lying in a supine position [22]. Length of the lower leg, defined as the distance from the floor to the top of the fibula head, was measured while the participant was in a sitting position where the lower leg was placed vertically to the floor.
Adjustment of seat height
During the 1MSTSTEST, participants were asked to sit down with the buttock in the middle of the standardised chair. The lower leg was placed in a vertical position with a 90° angle construction (floor to lower leg). The knee flexion angle was measured with the Easy Angle Digital Goniometer (Meloq, Sweden) [23] using a standardised lever from the trochanter major to the knee joint (figure 1). Depending on the knee flexion angle of the participant sitting on the standard chair, the seat height of the chair was adjusted, aiming to ensure a 90° knee flexion.

Measurement of knee flexion angle: a) start position with vertical position of lower leg, b) measurement of knee angle on the standard chair with 46 cm seat height, c) measurement of knee flexion angle of 90° after chair adjustment.
1MSTS test and additional assessments
The aim of the 1MSTS test is to perform as many STS repetitions as possible in 1 min [2, 4, 5]. We used a height-adjustable chair (Embru, Switzerland) without an armrest, stabilised against the wall. We only counted correctly performed STS repetitions.
We performed all 1MSTS tests on a chair with an individually adjusted seat height (90° knee flexion when sitting on the chair). Before each 1MSTS test, participants received standardised instructions [4] that did not include information about seat height. In this way, participants were blinded to the experimental condition. Before, immediately after, and for 1 min after completing each test, we monitored heart rate and oxygen saturation (SpO2) with a handheld pulse oximeter (Covidien Nellcor PM10N, Dublin, Ireland). At the same time points, we assessed ratings of perceived exertion and dyspnoea using a 0–10 Borg scale [24]. If participants needed oxygen while performing the tests, the same amount of oxygen was delivered for each test.
After completing the 1MSTS tests, subjects filled out a self-administered questionnaire. Questions evaluated understanding of the test instructions, the preferred sitting position on the chair, preferred change in seat height compared with the chair set-up that was used in the prior test condition and perceived difficulties during the test. The questionnaire was completed by each participant without asking the participant about the seat height (see online supplementary material).
Analysis
The primary outcome was analysed using two linear regression models. The first model (Model 1) focused on the difference in 1MSTS performance adjusting for the experimental condition (1MSTSSTD versus 1MSTSIND), period and subject [25]. This was based on our initial hypothesis and the assumption that taller people might be disadvantaged (and vice versa for shorter people) when performing the 1MSTS on a standard chair (1MSTSSTD). We assumed no difference in 1MSTS performance between the two experimental conditions on a population level, challenging the interpretation of the mean difference and 95% confidence intervals (CI). To account for that, we set up a second regression model (Model 2), in which we adjusted for experimental condition (1MSTSSTD versus 1MSTSIND), knee angle, the interaction of experimental condition and knee angle, period and subject. A significant chair times angle interaction would indicate that shorter people have advantages and taller people have disadvantages of different magnitudes with the different chairs.
To further explore the differences between the two experimental conditions, we used Bland–Altman plots to visually assess agreement in number of 1MSTS repetitions [26]. Such plots show average agreement (should be reasonably close to 0) and limits of agreement (gives a range of differences between the two conditions within which 95% of the observations fall). Additionally, we considered Bland–Altman plots adjusted for knee angle [27].
Secondary outcomes were the STS power index (STSPOWER) [22], post-test heart rate, nadir SpO2, perceived leg exertion and dyspnoea, and the number of incorrectly performed 1MSTS repetitions (e.g. legs were not fully straight during standing phase, or the chair was not touched with the buttock, or arms were used to support movement). All secondary outcomes were analysed with Models 1 and 2, except the number of incorrectly performed repetitions that were analysed qualitatively, and the self-administered questionnaire was analysed descriptively (n, %).
Sample size calculations were done using simulations in the R-Project, Version 4.0.3, www.r-project.org. Based on previous research from our group [4] we knew that repeated 1MSTS tests are highly correlated in people with COPD (r=0.95), and that we could expect a sd of about 6.3 for 1MSTS repetitions. With 33 participants, we estimated to have 80% power to detect a difference of 2 in the interaction term of the model including type of chair, knee angle, and the interaction between type of chair and knee angle. Additionally, based on the distribution of body height in our typical COPD population entering pulmonary rehabilitation (i.e. data were available from clinical charts), we expected fewer participants needing a higher seat height than the standard seat height. To account for this, we planned to extend recruitment until there were at least ten participants in this group. We planned to stop recruitment after inclusion of a total of 60 study participants, irrespective of the three group sizes.
The statistical analysis was performed using the R-Project, Version 4.0.3, www.r-project.org.
Results
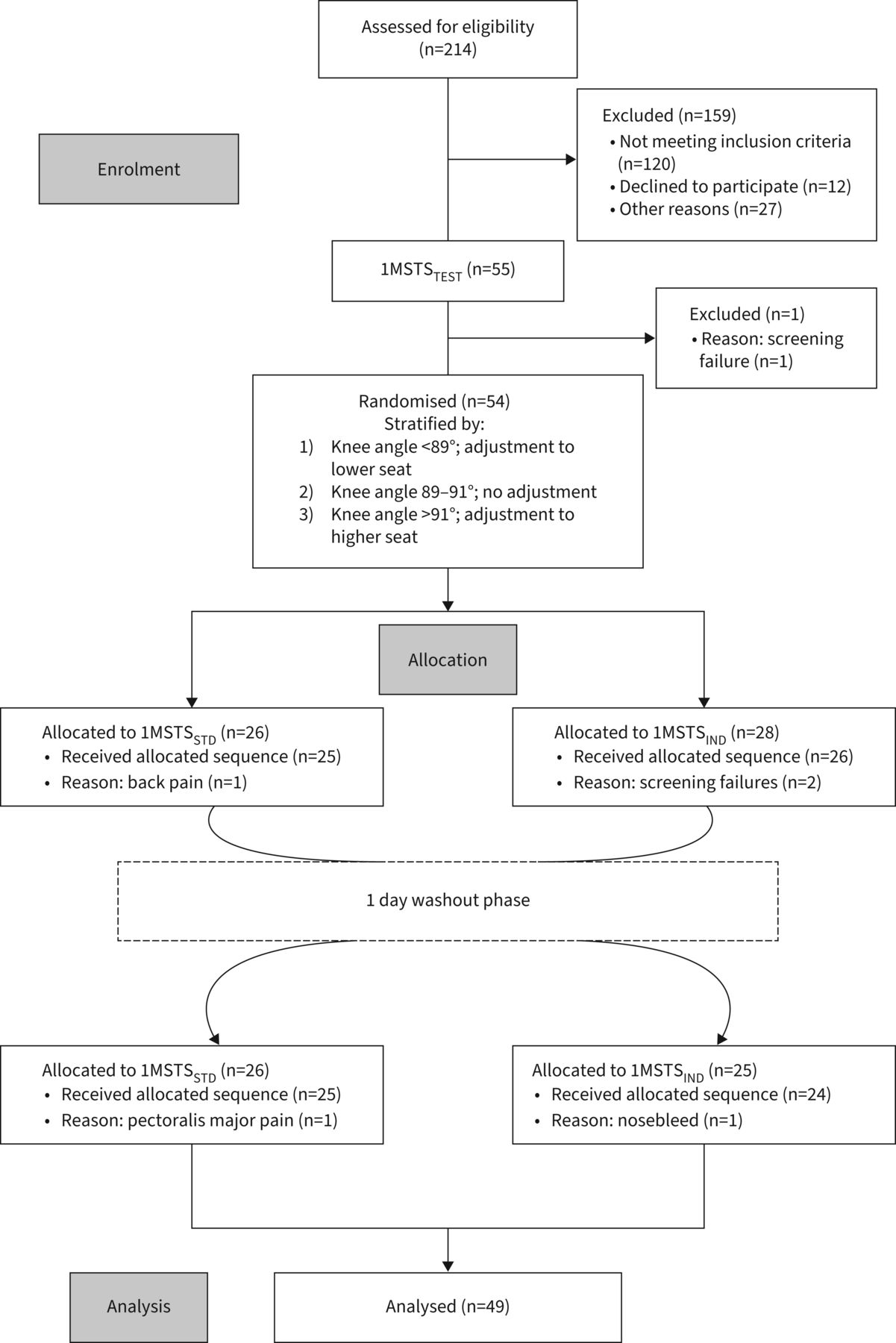
55 participants were included in the study. Six participants were excluded from the analyses due to screening failures (n=3) and health issues (n=3), leaving 49 participants for the final analysis (table 1, figure 2).
Participant characteristics

Flow chart. 1MSTSTEST: 1-min sit-to-stand test, familiarisation test performed on individually adjusted chair; 1MSTSSTD: 1-min sit-to-stand test performed on standard chair with a seat height of 46 cm; 1MSTSIND: 1-min sit-to-stand test performed on individually adjusted chair of 90° knee flexion.
In the allocated experiments requiring individual adjustment of seat height, 28 were tested on a lower seat height, and 10 participants were tested on a higher seat height than the standard chair. For the remaining 11 participants no seat height adjustment was necessary (i.e. knee angle on the standard chair was between 89° and 91°), and they performed both tests on the standard chair.
Primary outcome: 1MSTS test performance
In Model 1, 1MSTS test performance was −0.78 repetitions (95% CI −1.47 to −0.11, p=0.028) lower with 1MSTSIND compared to 1MSTSSTD. In Model 2, the interaction term for experimental condition and knee angle was statistically significant: 0.18 (95% CI 0.05 to 0.30, p=0.008) (table 2).
Mean differences between the two experimental conditions
The mean difference in repetitions of the two experimental conditions in participants with a knee angle less than 89° was −1.18 (limits of agreement −6.01 to 3.65) repetitions less on 1MSTSIND compared to 1MSTSSTD. The mean difference in repetitions in participants with a knee angle more than 91° was 0.8 (limits of agreement −4.24 to 5.84) repetitions more on 1MSTSIND compared to 1MSTSSTD. The mean difference in repetitions in participants with a knee angle of 89–91°, who performed the two 1MSTS tests on the standard chair, was −1.27 (limits of agreement −4.68 to 2.13) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Bland–Altman plot: difference (in repetitions) in the two experimental conditions. Solid lines: mean difference of repetitions; dashed lines: limits of agreement (1.96×sd); circles: representation of participants; 1MSTSSTD: 1 min sit-to-stand test performed on 46 cm height chair; 1MSTSIND: 1 min sit-to-stand test performed on chair adapted to 90° knee flexion.
There were three participants who had a difference in STS repetitions outside the limits of agreement (figure 3). Of those, two participants with a knee angle of 72° and 82° on 1MSTSSTD performed six and eight repetitions more than on the 7.2 cm and 5.5 cm lower 1MSTSIND, respectively, and one participant with a knee flexion angle of 93° on 1MSTSSTD performed six repetitions more on the 2.2 cm higher 1MSTSIND.
Figure S3 (see online supplementary material) gives an overview of the mean differences for the different knee flexion angles. We did not find a significant difference for a specific knee angle.
Incorrectly performed STS repetitions
Seventeen (34.7%) participants performed at least one and a maximum of three STS repetitions incorrectly. Four participants performed more incorrect STS repetitions on 1MSTSSTD, and 11 performed more incorrect STS repetitions on 1MSTSIND.
Among those 11 participants, the seat height of the 1MSTSIND was lower than 1MSTSSTS, in two participants it was higher, and in another two participants the seat height was 46 cm in both testing conditions (no adjustment needed as per study protocol).
STS power index
The STSPOWER – calculated with Model 1 – was not different between 1MSTSIND compared to 1MSTSSTD (0.05 Watts (95% CI −2.74 to 2.64)). In addition, the interaction term (Model 2) was not statistically significant: −0.23 (95% CI −0.76 to 0.30); see table 2.
Oxygen saturation, heart rate, and perceived dyspnoea and leg exertion
Post-test heart rate data were available for 46 (94%) participants. In three individuals, measurement artefacts were noted, and heart rate data had to be discarded. Nadir SpO2, post-test heart rate and perceived dyspnoea were no different between experimental conditions.
Perceived post-test leg exertion was 0.55 (95% CI 0.15 to 0.95) units higher on 1MSTSIND compared to 1MSTSSTD. The interaction term in Model 2 did not show a significant effect for leg exertion: −0.06 (95% CI −0.14 to 0.02); see table 2.
Self-administered questionnaire
All participants reported having understood the instructions of the 1MSTS test. Among 49 participants: 40 (82%) participants reported no need for adaptation of seat height when the test was performed on a standard chair (1MSTSSTD); 27% of participants who performed the 1MSTS with a lower seat height (1MSTSIND) preferred to raise the seat height; 18% of participants who performed both 1MSTS tests on the standard height chair preferred to raise the seat height; 50% of participants who performed the test with a higher seat height (1MSTSIND) reported to prefer to raise the seat height.
The participants reported the following reasons for preferring to perform the test on a higher seat height: “shorter distance to cover” (n=9), “less exhausting” (n=8), “more comfortable” (n=2), “easier to perform” (n=6).
Discussion
This randomised crossover study investigated the impact of an individually adjusted seat height on 1MSTS test performance compared with a commonly used seat height in people with COPD. We observed fewer repetitions and higher self-reported leg exertion on the individually adjusted seat height compared to the standard seat height. No differences between the two experimental conditions were observed in STSPOWER, subjective perception of dyspnoea or nadir SpO2.
Primary outcome: 1MSTS test performance
This study revealed a statistically significant difference between 1MSTSIND compared with 1MSTSSTD. However, the mean difference (95% CI) of −0.78 repetitions (95% CI −1.47 to −0.11) is negligible when interpreted on a study population level.
Our study sample included participants with a knee flexion angle of 72°–96° when sitting on the standard chair, resulting in an individual seat height ranging from 37.5 cm to 50.1 cm. We observed that a smaller knee angle (i.e. lower individual chair height) seems to result in fewer repetitions on 1MSTSIND compared to 1MSTSSTD, whereas a larger knee angle (i.e. higher individual chair height), seems to result in more repetitions on 1MSTSIND compared to 1MSTSSTD. Of note, the significant interaction term in Model 2 should not be overinterpreted. The mean difference of 0.78 repetitions is statistically significant, but probably not relevant for clinical practice. Notably, three of 49 individuals had a difference in STS repetitions outside the limits of agreement, as seen in figure 3. However, among those individuals, there was no clear association between difference in STS performance and body height, leg length or knee angle. Because our cohort did not include a sufficient number of very tall or short individuals, further studies may be necessary to determine whether adaptation of seat height is required to ensure a valid assessment of 1MSTS test performance in people with chronic disease.
Demura and Yamada [16] found no differences in floor reaction force parameters during a single STS movement using different seat heights in healthy elderly men. In their experiments, the differences in seat height were less than 20% of lower leg length [16]. In another study, a 19 cm difference in seat height was associated with a 12% increase in the time to stand up from a higher chair in healthy men aged 21–60 years [12]. In our study, the magnitude of individual changes in seat height was always less than 20% of an individual's lower leg length and ranged between 4.1 cm and 8.5 cm (i.e. in both directions).
Another study in community-dwelling older adults investigated the effect of seat height on 30 second STS test performance [28] and found a significantly lower test performance on a 43 cm standard chair compared to a seat height corresponding to 100%, 110% and 120% of lower leg length. A seat height of 100%, 110% and 120% of lower leg length was between 36 and 59 cm [28], and the magnitude of differences in STS repetitions was larger than in our study (−1.5, 95% CI −3.0 to −3.9), most likely because the range of individual adjustment was larger in their study compared to ours. Furthermore, participants in the study by Kuo [28] had better health status and performed as many repetitions during 30 seconds as our participants during 1 minute. It is important to note that individual adjustment of seat height may improve the accuracy of an individual's assessment of functional capacity. Irrespective of using a standard versus individually adapted chair, standardised testing methodology is critical in pre- and post-test study designs, and for the interpretation of an individual's change in functional capacity over time.
Secondary outcomes
In our study, participants reported significantly higher subjective leg exertion on 1MSTSIND compared to 1MSTSSTD (mean difference 0.55, 95% CI 0.15 to 0.95). Yamada and Demura [14] have shown that standing up from the seated position is more difficult for people with a more flexed lower leg. That means using a lower seat height increases the distance that a person must cover to perform the STS movement, thus increasing leg muscle activity [14]. This may have resulted in a higher subjective perception of leg muscle exertion in our study with little impact on overall 1MSTS performance on a study population level. Interestingly, during an STS task, people with COPD have a longer standing and stand-to-sit phase compared to healthy controls, resulting in lower performance [29]. The latter phase requires eccentric muscle contractions and a high knee extensor muscle activity, which might be one reason for the higher perceived leg exertion during 1MSTSIND compared to 1MSTSSTD. We further evaluated the force-generating capacity of the knee extensor muscles by calculating STSPOWER, a measure of mechanical power and functional capacity [21, 26]. We found no differences in STSPOWER between the two experimental conditions. It may well be that the difference in chair heights between the experimental conditions was not large enough to affect mechanical power values. Nevertheless, our observations of higher perceived leg exertion after performing the 1MSTSIND seem to be supported by the participants’ responses in the questionnaires. Among those who reported a desire to change the seat height, upward adjustment was preferred. Other secondary outcomes were not different between experimental conditions.
Strengths and limitations
We chose a crossover design in which each participant served as their own control in order to minimise confounding [30]. All assessments and test instructions were done by the same assessor, eliminating inter-rater variability. Moreover, we were able to mask participants as they did not receive details about the different experimental conditions and were not aware of seat height adjustments.
Our trial has limitations. We used the Easy Angle Digital Goniometer to measure knee flexion angles of the participants. The measurement is possible with a standard error of 1.15–1.48° and has a very high intra-rater (ICC 0.997) and inter-rater reliability (ICC 0.994) [23]. We decided not to change the height of the standard chair if the participant had a knee flexion angle between 89° and 91° while in a sitting position. We could have been more conservative by using a slightly greater range of knee angles.
In our study, we used a standard seat height of 46 cm, frequently used in people with chronic respiratory disease [6–8, 10]. Seat heights from 44.1 to 48.0 cm have been reported in different studies in elderly people and those with COPD [3–5]. Based on our experience in people with chronic respiratory diseases [4, 31–33], and exchange with other pulmonary rehabilitation centres across Switzerland, a chair height of 46–48 cm is commonly used. To best mimic current clinical rehabilitation practice, we decided to use a chair with 46 cm height as the standard chair. It is important to note that the generalisability of our findings to other chronic disease populations might be limited, in particular for populations with a larger distribution of relatively smaller or taller persons.
In conclusion, our data suggest no clinically relevant difference in 1MSTS performance between the use of an individually adjusted versus standard chair in people with COPD when interpreted on a group level.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Online Supplementary Material online_Supplementary_1MSTS_18_01_22_v1
Footnotes
Provenance: Submitted article, peer reviewed.
This study is registered at www.ClinicalTrials.gov identifier number NCT04579055.
Data availability: Our dataset has been deposited with Dryad (https://doi.org/10.5061/dryad.z8w9ghxfq).
Conflict of interest: V. Zumbrunnen has nothing to disclose.
Conflict of interest: T.F. Riegler has nothing to disclose.
Conflict of interest: S.R. Haile has nothing to disclose.
Conflict of interest: T. Radtke has nothing to disclose.
- Received January 18, 2022.
- Accepted June 10, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










