





Abstract
Background The incidence of bronchopulmonary dysplasia (BPD) following preterm birth is increasing. Bronchodilators are often used to treat patients with BPD with little evidence to guide therapy. The aim of this study was to test the hypothesis that there are infant pulmonary function test (iPFT) parameters that can predict subsequent bronchodilator response in infants with BPD.
Methods Subjects in this study were part of a patient group in which we reported three BPD phenotypes (obstructive, restrictive and mixed) based on iPFT data. From that group, a cohort of 93 patients with iPFT data including bronchodilator response was eligible for this study.
Results Bronchodilator responsiveness was found in 59 people (63%) in the cohort. There were no differences in demographics between the responders and non-responders. There was no difference in forced vital capacity (FVC) between the two groups. Responders had significantly lower forced expiratory volume in 0.5 s (FEV0.5) and FEV0.5/FVC (p<0.005) and greater indices of hyperinflation than did non-responders (p<0.005). Logistic regression modelling found that pre-bronchodilator FEV0.5 and functional residual capacity/total lung capacity were significantly associated with bronchodilator response. The magnitude of response to bronchodilators was negatively correlated (R= −0.49, R2= 0.24, p<0.001) with the FEV0.5. The median dysanapsis ratio in responders (0.08, 95% CI 0.05–0.19) was significantly (p=0.005) smaller than in non-responders (0.18, 95% CI 0.06–0.38).
Conclusion These findings demonstrate that there are pulmonary function test parameters associated with bronchodilator response. Responders had evidence of greater dysanaptic lung growth than non-responders.
Abstract
In 93 BPD patients, 63% were responsive to bronchodilators and responders had significantly lower FEV0.5 and greater hyperinflation than did non-responders. The dysanapsis ratio in responders was significantly smaller than in non-responders. https://bit.ly/3yaWieK
Introduction
Bronchopulmonary dysplasia (BPD) was first described by Northway et al. [1] in 1967 and is now the most common morbidity following preterm birth, with an incidence that is increasing [2, 3]. A recent definition of BPD based on respiratory support at 36 weeks post-menstrual age (PMA) divides BPD into three grades: Grade 1, low-flow nasal cannula; Grade 2, noninvasive positive pressure; and Grade 3, invasive positive pressure [4]. There is little high-grade evidence to support therapeutic approaches in patients with BPD, but despite this lack of evidence patients with BPD are often treated with bronchodilators [5, 6]. However, the use of bronchodilators in BPD is extremely variable between providers and between centres [7, 8].
Pulmonary function studies have been reported in children and young adult survivors of BPD [9–11] as well as in preterm infants developing BPD [12]. However, there is little pulmonary function data from infants with established BPD during their neonatal intensive care unit (NICU) hospitalisation. We recently described a cohort of patients with BPD who had infant pulmonary function testing (iPFT) done during their NICU hospitalisation and found that the iPFT data divided the patients into three phenotypes: obstructive, restrictive and mixed [13]. We also reported [13] that in those infants tested for bronchodilator responsiveness (BDR), 66% had BDR and those with BDR had a lower pre-bronchodilator (pre-BD) forced expiratory volume in 0.5 s (FEV0.5). This finding led us to hypothesise that iPFT parameters can be used to predict BDR in infants with established BPD during their NICU hospitalisation.
Modelling the airways as tubes and using Poiseuille's law suggests that airway diameter has the greatest effect on airway resistance and the smallest airways have the greatest resistance [14]. It has been shown even in young children and infants without lung disease that peripheral airways have high resistance, and that there is a marked decrease in resistance at 4–5 years of age [15]. Dysanaptic lung growth refers to the non-proportional growth of airways and lung resulting in relatively small airways for lung size [16]. It has been suggested that the dysanapsis ratio (DR) can be used as a noninvasive method of describing the relationship between airway calibre and lung size, where the smaller the DR, the greater the dysanaptic lung growth [17]. The DR has been shown in adults to be a predictor of expiratory flow limitation [18, 19]. To the best of our knowledge, no one has examined the DR in relation to BDR in infants with established BPD. Therefore, we tested the hypothesis in these infants with BPD and assessment of BDR, that those with BDR would have a smaller DR than non-responders. In other words, infants with BDR would have relatively smaller airways relative to their lung size than non-responsive infants.
Methods
This study was approved by the institutional review board at Nationwide Children's Hospital, Columbus, Ohio, USA, and informed parental consent was obtained from all subjects.
Subjects
The subjects in this cohort are the subset of a cohort that was described in our recent publication [13] who had BDR testing done. Briefly, data were collected from infants hospitalised in the NICU with a primary diagnosis of BPD who were referred for their first iPFT from May 1, 2003, to October 8, 2015. In our BPD unit, patients are referred for iPFT when they fail to make significant progress; the decision to refer for iPFT is made by consensus of the multidisciplinary BPD team. We estimate that the cohort represents ∼15% of all BPD patients admitted to our BPD unit during this time frame.
iPFT
All iPFTs were performed using the Infant Pulmonary Laboratory (nSpire Health, Inc., Longmont, CO, USA). If present at the time of iPFT, endotracheal tubes or tracheostomy tubes were replaced with cuffed tubes prior to testing. Infants were sedated with chloral hydrate and underwent raised volume rapid thoracic compression spirometry and body plethysmography measurements as previously described [13, 20–22]. The reproducibility of these measurements in our iPFT laboratory has been previously reported, as have the normative data [20–22].
BDR testing
Albuterol was held for 8 h prior to testing. After pre-BD iPFTs were completed, two puffs of albuterol were given every 2 min until a 10% increase in heart rate was noted or a maximum of eight puffs were given, and then the iPFTs were repeated. For this study, we defined BDR as a >10% increase in FEV0.5 (% predicted) as previously described by Goldstein et al. [21], which represents ≥2 sd above the normative mean for change in FEV0.5 in infants. The coefficient of variation for FEV0.5 is 2.2% [21].
DR
The DR is calculated from the forced expiratory flow at 50% (FEF50) of forced vital capacity (FVC), using the equation FEF50/(FVC×Pst(l)50) [19], where Pst(l)50 is the static recoil pressure at 50% of FVC. We used data from Turner et al. [23] to extrapolate Pst(l)50 based on the equation Pst(l)50= −0.056×age (years)+6.3038, as previously described in both adults [18, 19] and children [24]. The DR is inversely related to dysanaptic lung growth, i.e. the smaller the DR, the more dysanapsis.
Data analysis
Pulmonary function data were collected in accordance with American Thoracic Society/European Respiratory Society guidelines [25], and for each subject represent three measurements within 5–10% of each other. iPFT data are given as % predicted. Data were also collected on subject demographics and outcomes.
Statistical analysis
Data are presented as median and interquartile range (IQR), mean±sd or number (%). The continuous data were compared between groups using a Mann–Whitney U test (Sigmaplot 14.0, Jandel Scientific, Carlsbad, CA, USA). A Fisher's exact test was used to compare categorical data between groups (GraphPad Prism 8, GraphPad, San Diego, CA, USA). Selected variables were used in multiple logistic regression modelling (Sigmaplot) and results are presented as odds ratio and 95% confidence interval. The area under the receiver operating characteristic curve (AUROC) was calculated for selected variables (GraphPad). Linear regression modelling was used for some data pairs (Sigmaplot). A p-value of <0.05 was considered significant.
Results
There were 93 patients with BDR testing: 59 (63%) met criteria for BDR and were termed responders, and the remaining 34 (37%) were termed non-responders. There were no differences in any of the demographic variables between the two groups (table 1). Importantly, at the time of iPFT there were no differences between the two groups in terms of PMA, length, weight or type of respiratory support. The majority of infants (62%) had Grade 3 BPD, 24% had Grade 2 BPD and 2% had Grade 1 BPD. An additional nine infants (11%) lacked reliable respiratory support data at 36 weeks PMA and were therefore non-classifiable.
Demographics
The pre-BD iPFT results are shown in table 2. There were 47 infants (51%) categorised as having obstructive BPD (FEV0.5 <80% predicted and total lung capacity (TLC) ≥90% predicted), 38 (41%) categorised as having mixed BPD (TLC <90% predicted and FEV0.5/FVC <90% predicted) and eight (9%) categorised as having restrictive BPD (TLC <90% predicted and FEV0.5/FVC ≥90% predicted). There were more infants with moderate/severe obstruction in the responder group than in the non-responder group. Responders had lower FEV0.5 and FEV0.5/FVC than non-responders. Responders had greater indices of hyperinflation on iPFT (residual volume (RV)/TLC and functional residual capacity (FRC)/TLC) than non-responders.
Pre-bronchodilator iPFT results
The expiratory flow or indices of hyperinflation from the pre-BD iPFTs that were significantly different between responders and non-responders were used in multiple logistic regression models. To avoid over-fitting our models we examined flows (parameters=7) and indices of hyperinflation (parameters=6) separately, and included PMA, length and weight at the time of iPFT in the models. When pre-BD expiratory flows were used in the logistic regression model, only pre-BD FEV0.5 was significantly associated with BDR (table 3). When the indices of hyperinflation were used in the logistic regression model, only pre-BD FRC/TLC was associated with BDR (table 3). The AUROCs for pre-BD FEV0.5, FEF50 and FRC/TLC are given in table 4.
Logistic regression parameters
AUROCs
To determine if the magnitude of BDR in responders was related to pre-BD flows, hyperinflation or both, we examined the magnitude of BDR as given by the change in FEV0.5 pre-BD to post-BD in responders. The median magnitude of BDR in the 59 responder patients was 26% (IQR 19–39%). The magnitude of BDR in the responders was negatively correlated with the pre-BD FEV0.5 (figure 1). The magnitude of BDR in responders was not correlated with the pre-BD FRC/TLC (R=0.21, R2=0.04, p=0.11).
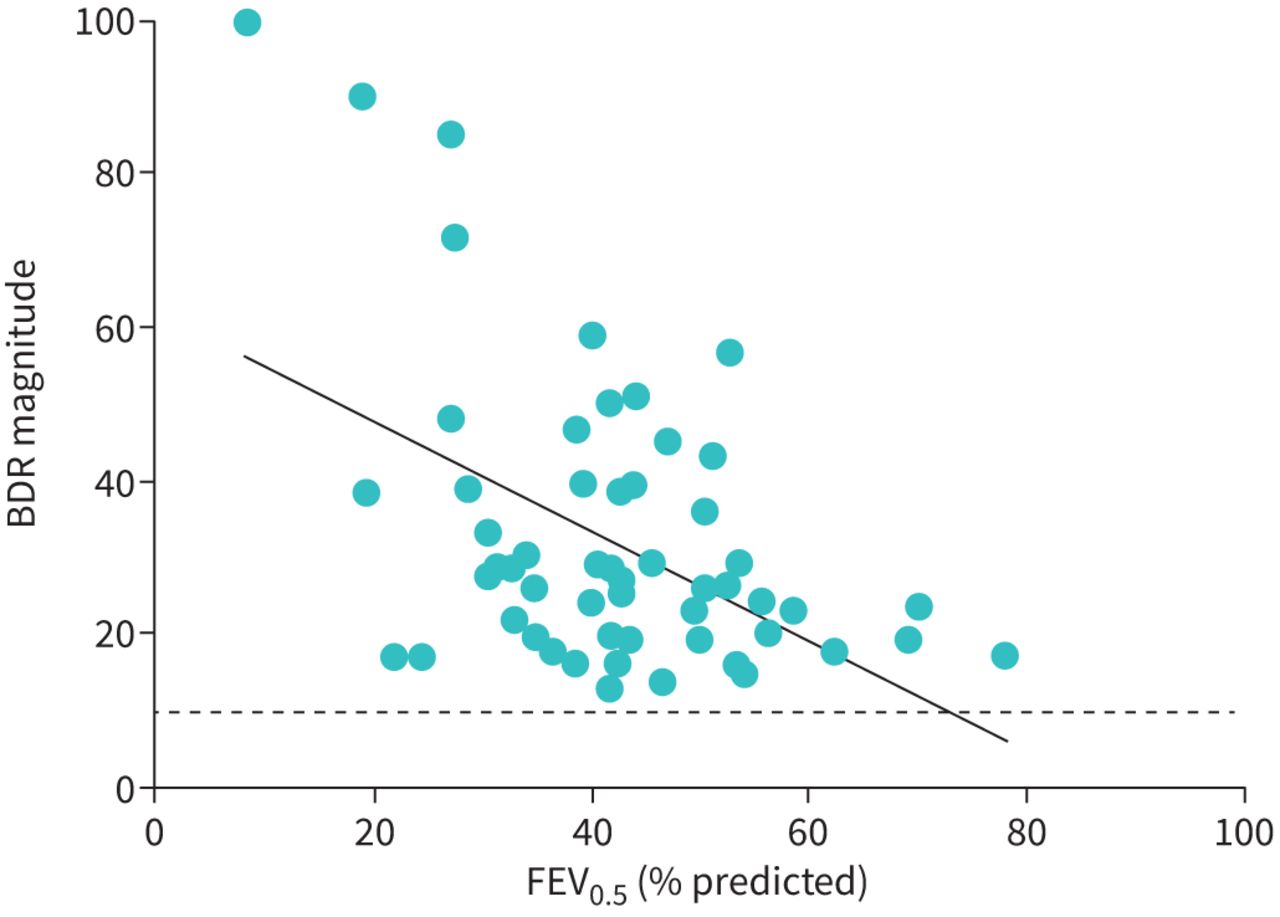
The magnitude of bronchodilator responsiveness (BDR) is negatively correlated with forced expiratory volume in 0.5 s (FEV0.5). The linear regression fit (solid line) (y= −0.72x+62, R= −0.49, R2=0.24, p<0.001) suggests that 24% of the variation in the magnitude of BDR is due to FEV0.5. The dashed line represents the threshold for BDR.
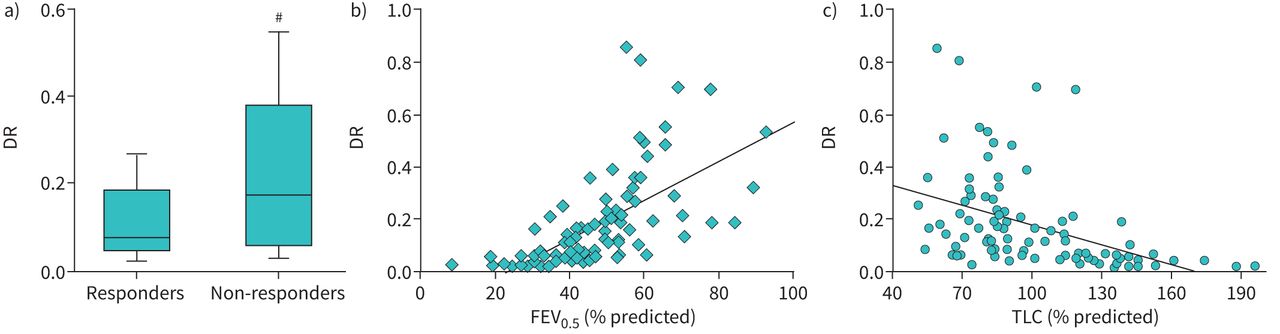
The median DR in responders was significantly smaller than the median DR in non-responders (figure 2a), suggesting greater dysanaptic lung growth in responders than non-responders. Because we were using an algorithm for calculating Pst(l)50 that used age in years, and given that our range of ages in years was quite narrow (0.23–1.91 years), we examined the relationship between DR and chronological age in years for the entire cohort and found no significant correlation by linear regression (R=0.11, R2=0.01, p=0.31). There was also no correlation between DR and PMA (in weeks) (R=0.12, R2=0.01, p=0.27). Examining the relationship between DR and FEV0.5 using linear regression we found a significant correlation (figure 2b). We also examined the relationship of DR to TLC using linear regression and found a significant negative correlation (figure 2c). Using multiple logistic regression modelling and including PMA and length and weight at time of iPFT, DR predicted BDR with OR 0.011 (95% CI 0.001–0.195, p=0.002; table 3).

{kind=link}
{kind=link}
a) Dysanapsis ratio (DR) was significantly larger in non-responders than in responders. b) DR was correlated with the forced expiratory volume in 0.5 s (FEV0.5) (linear regression fit; y=0.007x–0.174, R=0.62, R2=0.39, p<0.001). c) DR is negatively correlated with total lung capacity (TLC) (y= −0.003x+0.434, R= −0.44, R2=0.19, p<0.001).
There were no differences in outcomes between the two groups (table 5).
Outcomes
Discussion
This study demonstrates that in a cohort of NICU patients with BPD referred for iPFT, the majority of which had Grade 3 BPD, 63% of patients were responsive to bronchodilators. There were no demographic differences between responders and non-responders in this cohort of infants. We did find that pre-BD values for FEV0.5 and FEF50 were lower in responders than in non-responders, with more hyperinflation as assessed by RV/TLC and FRC/TLC on the iPFT in responders than in non-responders. Indeed, the FEV0.5 and FRC/TLC were modestly predictive of BDR in this cohort using logistic regression modelling and AUROC analysis.
Infants in this cohort all had BPD and all but two subjects had either Grade 2 or Grade 3 BPD. Even in this population in which 91% had obstruction, 37% of the subjects were non-responsive to bronchodilators. The cohort is not a consecutive cohort of all patients with Grade 2 or Grade 3 BPD, but rather infants chosen for iPFT based on no clinical response to usual therapy. Several studies have examined BDR in older children or young adults who have BPD [9, 10, 11], but there are very few published studies examining BDR using iPFT in BPD infants during their initial NICU hospitalisation. Morrow et al. [26] evaluated 40 preterm infants with evolving BPD with iPFTs at a mean PMA of 35 weeks and found that 65% had a response to bronchodilators, and responders tended to have a greater baseline respiratory system resistance than non-responders [26], consistent with our findings that responders tended to have a lower FEV0.5 than non-responders. Robin et al. [27] evaluated 17 infants with BPD at a mean postnatal age of 68 weeks (our cohort had a mean postnatal age of 30 weeks) and found that 35% had significant BDR (defined as a change in FEF75 >24.3%). Furthermore, they reported that responders had significantly lower baseline FEF75 than non-responders [27], again consistent with our findings. Together with our data, these findings support the notion that not all patients with established BPD have BDR and that patients with greater obstruction at baseline are more likely to demonstrate BDR.
Responders had more hyperinflation on iPFT than non-responders, as evidenced by larger RV/TLC and FRC/TLC ratios as well as smaller vital capacity. It has been shown that infants with BPD have greater RV/TLC than infants without BPD [27]. Recently, Yoder et al. [28] used magnetic resonance imaging (MRI) to measure FRC in NICU patients at PMA between 35 and 42 weeks and found that subjects with severe BPD had significantly greater FRC than subjects with mild BPD. Dassios et al. [29] found that the greater the degree of hyperinflation in preterm infants (studied at a median of 6 weeks of age), the greater the ventilation/perfusion mismatch. To the best of our knowledge we are the first to describe in a cohort of patients with BPD that there are measurable differences in hyperinflation, with more hyperinflation in those infants who respond to bronchodilators than in those who do not respond. In adults with chronic obstructive pulmonary disease, it has also been reported that patients with lung hyperinflation have better bronchodilator responsiveness [30]. These findings suggest that the degree of hyperinflation may underlie BDR in BPD and further studies are needed to examine biomarkers of hyperinflation in relation to BDR. These findings also raise the question of whether bronchoconstriction is involved in the mechanism underlying hyperinflation in BPD.
We found no evidence of a pre-BD FEV0.5 cut-off value for predicting BDR, but there was a negative correlation between the magnitude of BDR and FEV0.5. The lung volume parameters FRC/TLC and RV/TLC were not significantly correlated with the magnitude of BDR. These findings have potential implications for precision therapeutics in BPD. Multicentre studies have shown extreme variability in bronchodilator use in patients with severe BPD [5–8], which suggests a lack of high-quality evidence to support the precise utilisation of bronchodilators targeting those patients who may benefit from the medication. In our unit, these patients are treated with bronchodilators. Our findings demonstrate that not all infants with severe BPD demonstrate BDR, which may lead clinicians to use other criteria (e.g. physical examination, changes in delivered tidal volumes or pressures on the ventilator, tolerance of therapies) that are not standardised to guide their use of bronchodilators. Our findings also suggest that iPFT data can predict BDR in the most severe forms of BPD. It should be remembered that though bronchodilators are widely used and generally considered safe in BPD patients, bronchodilators are not without risk [31, 32]. Targeting the use of bronchodilators to BPD patients with physiological evidence of expiratory flow limitation on iPFT may be one way to optimise therapeutic effects while avoiding medication side-effects.
The mechanisms underlying bronchoconstriction and BDR in patients with BPD are likely to be very complex and multifactorial; understanding exactly the mechanisms involved in this cohort are beyond the scope of this study or any single study. However, we did wonder how lung growth and, particularly, dysanaptic lung growth might affect BDR in established BPD in patients still in the NICU. We found in this cohort of BPD patients that the DR was smaller in responders than in non-responders, suggesting that BPD patients with BDR likely have relatively smaller airways in proportion to their lung size than non-responders. Duke et al. [19] reported in adult survivors of preterm birth that those with BPD had smaller DR than adult survivors of preterm birth without BPD, and that the DR was significantly correlated with peak expiratory airflow at rest and the extent of expiratory flow limitation during exercise. This suggests that at least some of the BD response in the responder group may be due to their relatively smaller airways in relation to lung size. Another way to think of this is that in patients with lower DR, the relatively smaller airways in relation to lung size would be more likely to have a measurable change in iPFT parameters following BD administration. Furthermore, patients with smaller DR would be expected to have lower FEV0.5 and FEF50 due to the relatively higher airway resistance, and we found a direct correlation between DR and FEV0.5 in this cohort. The relationship between DR and FEV0.5 also suggests that dysanaptic airway development underlies at least some of the BDR seen in the responder group in this cohort of NICU patients with BPD. The finding that DR was correlated with TLC and that the patients with the largest TLC (i.e. the greatest amount of hyperinflation) had the lowest DR may suggest that dysanaptic lung growth also contributes to the hyperinflation seen in patients with severe BPD. Further studies are needed that examine dysanaptic lung growth in BPD. It would be interesting to examine, for instance, whether DR increases with good somatic growth, i.e. if airway calibre increases relatively more than lung size increases as the lung grows, and whether this is a mechanism for the improvement in lung function seen in established BPD with good linear growth.
There are some limitations to this study that should be noted. First, it was not a consecutive cohort of subjects, and thus not a true epidemiological assessment of BDR in BPD. However, as far as we know this is the largest cohort of BPD infants with BDR testing during the initial NICU hospitalisation. Another aspect of this is that the patients studied represent the severest forms of BPD given that the patients were referred if they were not responding as expected. Thus, these data may not be widely generalisable to all BPD. Second, to obtain the measurement of DR we used static recoil pressures at 50% of lung volume (Pst(l)50) extrapolated from adult values [23] as has been previously described [18, 19, 24]. However, given the lung growth that occurs from birth through early childhood, the assumption of a linear relationship of Pst(l)50 values with age in early childhood may not be entirely valid [15]. However, despite this limitation we were able to find differences in DR between infants, expected correlations with other iPFT parameters, and no significant correlation between DR and age in this cohort. A third potential limitation might be that we were unable to correlate our iPFT findings with either thorough physical examination data or rigorous imaging data. Another potential limitation is that iPFT is not widely available in this age range of patients. However, with advances in ventilator technology, ventilators now provide in-line measurements of at least some aspects of pulmonary function and there continues to be the development of new methods of measuring pulmonary function in this age group (such as forced oscillometry, MRI, etc.). Finally, the parameters studied here to predict BDR were only moderately predictive using AUROC analysis; thus, further studies to find better predictive tests for BDR are required, and these predictive lung function tests should include parameters readily available to the clinician.
Conclusion
We found in a cohort of patients with BPD that most, but not all, were responsive to bronchodilators. The measured iPFT parameters associated with BDR in this cohort were FEV0.5 and FRC/TLC ratio. Our results suggest that future studies are needed to better predict BDR in patients with BPD. Interestingly, the group of responders demonstrated dysanaptic lung growth, suggesting relatively small airways compared to their lung size. A better understanding of how airways and lung parenchyma grow in BPD patients may shed light on disease progression.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: The authors have no conflicts of interest relevant to this article to disclose.
- Received December 3, 2021.
- Accepted April 26, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










