





Abstract
Background Systemic biologic agents can increase the risk of re-activation of latent tuberculosis (TB). Prior to initiation, screening for latent TB using an interferon-γ release assay (IGRA) is recommended. There is concern that false-negative IGRAs may be more likely in this context.
Methods This retrospective analysis of IGRAs, specifically T-SPOT.TB, results and outcomes of patients already on or due to start biologics identifies the rate of TB re-activation in a low TB incidence setting. Additionally, we estimate the negative predictive value (NPV) of IGRAs in this population.
Results Patients on biologics were more likely to have a negative IGRA result than patients not on biologics. There was no statistically significant change in conversion or reversion rates between groups. Of 9263 patients on biologics, 19 developed active TB after starting biologics at an incidence rate of 55.1 per 100 000 patient-years. This occurred despite screening in half of the 16 patients for whom we were able to review medical records. Most drugs implicated were known to be high risk, although rituximab and natalizumab were being taken by five patients and one patient, respectively. The T-SPOT.TB NPV was 99.20% and dropped only slightly to 99.17% when we simulated an approach where all borderline IGRA results were regarded as being negative.
Conclusions Negative IGRA results confer a low risk of subsequent active TB in patients on biologics in a low TB incidence setting. However, continued awareness is needed given that a number of active TB cases will have had a prior negative result.
Abstract
This retrospective analysis examines TB outcomes and IGRA performance in a large cohort of patients on biologics. It signals that negative and even borderline IGRA results confer a low risk of subsequent active TB in patients on biologics. https://bit.ly/3T9rlQ7
Introduction
Latent TB screening
Interferon (IFN)-γ release assays (IGRAs), including the QuantiFERON-TB Gold (QFT-G) (QIAGEN, Hilden, Germany) and the T-SPOT.TB (Oxford Immunotec, Abingdon, UK) tests, measure IFN-γ release by T-cells following exposure to Mycobacterium tuberculosis antigens and are used as screening tools. Positive IGRA results do not distinguish between active TB and latent TB infection (LTBI) [1]. A difference in the accuracy of the interpretation of both tests is that only T-SPOT.TB uses a borderline zone to reduce false-positive and false-negative results around the T-SPOT.TB test cut-off. The manufacturer frames borderline results as belonging to a group of patients among whom a substantial proportion will test positive if the test is repeated. They recommend a repeat T-SPOT.TB for borderline and invalid results [2].
On repeating IGRAs in the same patient, conversions or reversions may occur. Within high-risk populations in TB endemic areas, conversions are more common and more likely to represent a true new infection [3]. There are limited data evaluating repeat test “within-person” variability, especially where there is low risk of new TB exposure. Furthermore, variability occurs between samples taken at the same time on the same patient. There is neither consensus regarding the expected amount of variation in serial measurements nor how to act on them clinically and concern that this phenomenon is incompletely explained [4].
Biologics
Certain biologics confer a high risk of re-activation of LTBI. Risk of re-activation must be considered when commencing these medications [5]. Patients on anti-tumour necrosis factor (TNF)-α therapy have a 14-fold higher risk of developing active TB than healthy controls, although this varies between agents [6, 7].
Patients on biologics may also be at greater risk of TB infection or re-activation due to concomitant use of other immunosuppressive agents such as disease-modifying anti-rheumatic drugs or glucocorticoids [7, 8]. IGRAs may be unreliable in patients taking steroids, disease-modifying agents or biologics. The latter can cause a decrease in circulating T-cells releasing IFN-γ or in overall IFN-γ production. This may cause indeterminate or false-negative IGRA results. Biologics may affect IFN-γ in a dose-dependent manner. In vitro studies in whole-blood cultures from patients due to start anti-TNF-α treatment have demonstrated that higher doses of adalimumab are associated with decreased IFN-γ production [9].
Our TB service at Imperial College Healthcare NHS Trust, based across three hospital sites in north west London in the UK, spans low TB incidence boroughs such as Kensington and Chelsea (15.1 per 100 000 population) and high TB incidence boroughs such as Brent (45.6 per 100 000 population) [10]. The highest incidence of TB within the UK is in London, where the incidence was 25.1 per 100 000 between 2013 and 2019 [11]. Annually, our TB service sees approximately 120 cases in outpatient and inpatient settings. Our locally derived guidance tool classifies biologic agents into a “traffic light” system based on their risk of TB re-activation (table 1): red group drugs confer the highest risk of re-activation and require screening before commencement; amber group drugs confer a lower risk of re-activation, but LTBI screening is still required in all patients; and green group drugs are thought to confer the lowest risk of re-activation, in which case LTBI is not routinely required and depends on individual risk factors.
“Traffic light” classification to guide latent tuberculosis infection screening prior to starting biologics
Research gap
In clinical practice, there is concern regarding the increased likelihood of false-negative IGRA results in patients taking, or due to commence, biologics. If a false-negative occurs, patients being started on or allowed to continue biologic therapy without receiving LTBI treatment are theoretically at increased risk of developing active TB. We aimed to establish the negative predictive value (NPV) of IGRAs in immunosuppressed patients to determine how confident clinicians can be in negative and borderline IGRA results within this patient cohort. Additionally, we sought to identify the TB re-activation rate among patients on biologics.
Methods
We performed a retrospective review of all patients undergoing T-SPOT.TB testing prior to or during biologic therapy at our institution between 2013 and 2019. Dispensing and prescription activity for biologics between 2013 and 2019 were collated. Data included the earliest and most recent prescriptions of each drug. Data on whether a drug was stopped and restarted were not available. The London TB Registry (LTBR), a Public Health England-led reporting database of all patients diagnosed with active TB in London, was searched against the hospital prescription data to identify all patients who had ever had active TB and who had been prescribed biologics between 2013 and 2019. A dataset of all IGRA tests performed during this time by North West London Pathology, the laboratory which oversees IGRA testing for our institution, was also acquired. Finally, a dataset was collated of all patients who during the study period had been dispensed TB-relevant drugs, including ethambutol, isoniazid, levofloxacin, moxifloxacin, pyrazinamide, rifampicin, Rifater, Rifinah and Voractiv. Analyses conducted between these datasets were linked by the first letter of the forename, surname and date of birth.
Patients were included in the analysis if their date of TB diagnosis (as recorded in the LTBR) was after the first date they were dispensed a biologic agent. T-SPOT.TB timings are discussed with reference to the day the result was reported by the laboratory, which usually occurs 24–48 h after sampling. Once patients who developed TB following biologic therapy were identified, electronic medical records were used to collect further relevant information.
Results for the T-SPOT.TB test are interpreted by subtracting the spot count in the nil control well from the spot count in each of the panels A and B. Spots are produced as a result of antigen stimulation appear as large, round and dark spots. Samples are considered positive if the number of spots in panel A and/or panel B number ≤5 (after subtracting any spots in the nil control). If the spot count in panel A or B is 6 or 7, and neither panel has a spot count of ≥8, then the result is considered borderline (equivocal). Results are considered invalid if: the nil control has >10 spots, the phytohaemagglutinin positive control has <20 spots or there is a high background staining making it difficult to visualise the spots in each well.
Public Health England publications were used for estimates of TB incidence as comparators [10, 12]. Excel version 16.43 (Microsoft, Redmond, WA, USA) was used for manual data collection and analysis was conducted in RStudio version 1.1463 (RStudio, Boston, MA, USA). Chi-squared tests were performed with Yates’ correction to evaluate differences between groups; when observed variables were small, Fisher's exact test was used instead. 95% confidence intervals are used throughout and were modelled assuming a Poisson distribution. Approvals were obtained from the Imperial College Healthcare NHS Trust Clinical Audit Team.
Results
Local activity
Between 2013 and 2019, 9263 patients had biologics dispensed (with a total 11 433 unique prescriptions), of which 94 were found on the LTBR, suggesting that they had been diagnosed with active TB at some point. In our laboratory during the same period, 30 817 unique patients underwent IGRA testing, accounting for 39 890 tests. Of these, T-SPOT.TB accounted for 31 216 tests in 24 672 unique patients (demographic data summarised in table 2), with the remainder being QFT-G which were excluded from all further analyses. Combined, 4408 IGRAs were conducted on patients identified in our biologics dataset, with 4075 being T-SPOT.TB assays. In total, 27 141 T-SPOT.TB assays were conducted in patients not taking biologics.
Demographic data for patients who underwent T-SPOT.TB testing
In all T-SPOT.TB assays, the majority of assays were reported as negative (21 862/31 216 (70.03%)), more frequently in patients on biologics than in those who were not (77.0% versus 69.0%; p<0.001). Patients on biologics were less likely to have positive assay results (5.6% versus 12.5%; p<0.001) or borderline results (2.4% versus 3.2%; p=0.010). T-SPOT.TB assays in those on biologics were more frequently indeterminate (8.5% versus 6.6%; p<0.001). Patients on green biologics returned the greatest proportion of positive, borderline, indeterminate and “other” results, with the lowest proportion of negative results in comparison to other groups; those on amber biologics had the highest proportion of negative results (table 3).
Results of T-SPOT.TB assays by patient and drug grouping#
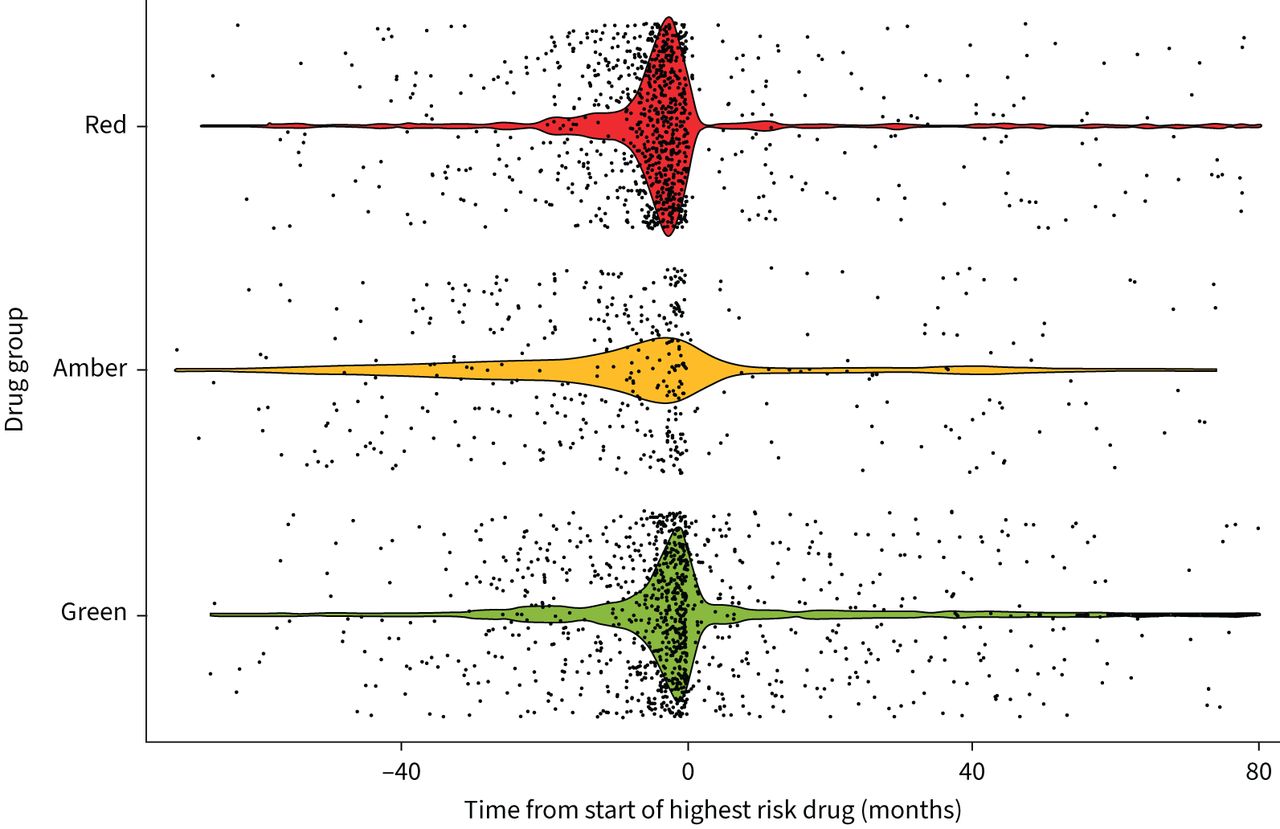
The median (interquartile range (IQR)) time difference from date of biologic prescription to date of IGRA test was −2.8 (−8.3– −0.3) months, suggesting that the majority of the tests were likely conducted as screening tests (figure 1).

{kind=link}
Violin/scatter plot of timing of interferon-γ release assay (IGRA) relative to the start of biologic therapy. Green, amber and red refer to the traffic light categorisation of biologic agents used locally and correspond to increasing risk of tuberculosis re-activation (table 1). Where individual patients were on multiple biologics in different categorisations, their time of assay is plotted relative to the time at which they started their first “highest risk” drug (i.e. their first red drug); if no red drug was started, then their first amber drug. The median time for T-SPOT.TB assays conducted in patients in the amber group was earlier than the red group, which was in turn earlier than those in the green group; these differences all met statistical significance using a Welch two-sample t-test (amber versus red: p=0.02; red versus green: p<0.001; amber versus green: p<0.001).
Patient-level data
The LTBR searches identified 94 patients who had been diagnosed with active TB and started biologic medication, among whom 19 developed active TB following our first recorded instance of biologic therapy use.
Medical records were available for 16 of these patients. The remaining three patients were managed by other centres. Of the 16 patients included, review of clinical notes, laboratory results (blood, sputum and histology) and imaging demonstrated clear evidence of pre-screening for LTBI before initiation of biologics in eight patients (supplementary table S1). There was no evidence of LTBI screening in four patients and it was unclear in the remaining four patients due to lack of historical data in clinical notes. Of the 16 patients, four patients had received previous treatment for LTBI; of these, one patient had stopped LTBI treatment after 1 month due to hepatotoxicity. Of the four patients treated for LTBI, three had clear evidence of LTBI screening.
There were no clear shared characteristics or risk factors for these 16 patients, although 11 patients were aged >50 years and five were born in high TB incidence countries. A cancer diagnoses (either current or historical) was present in seven patients, most commonly lymphoma. Rheumatoid arthritis occurred in four patients, two had psoriatic arthropathy, two had Crohn's disease and two had ulcerative colitis. Due to the small sample size, no statistical inferences could be made.
At the time of their first screening IGRA test, 14 patients were immunosuppressed. The two patients who were not immunosuppressed had an initial positive IGRA. All patients who had a negative IGRA were immunosuppressed. Of those who were immunosuppressed, three had a positive first IGRA, five were indeterminate and six were negative. Of the 11 patients who had an indeterminate or negative first IGRA, there were various subsequent outcomes: no further IGRA (n=1), positive IGRA on subsequent testing (n=4), no future positive IGRA despite subsequent testing (n=4) and positive IGRA after multiple tests (n=1; positive result on third serial IGRA). Subsequent IGRA tests occurred 1–10 months after the initial IGRA.
TB incidence by group
Within our data, 34 468 patient-years of observational data were available, over which time 19 patients developed TB after starting biologic therapy. The prevalence was 0.36% in the group on red biologics and 0.18% in those on green biologics; neither met statistical significance when compared with the entire population on biologics, for which the prevalence was 0.21%. Comparative incidence rates are described in table 4.
Incidence of tuberculosis (TB) across biologic risk groups
Specific biologic agents
Various biologics known to increase TB re-activation risk were shown to have been dispensed prior to diagnosis of active TB: most commonly infliximab (implicated in five cases), etanercept (three cases) and adalimumab (two cases). Of note, rituximab was dispensed prior to diagnosis of active TB in five cases and natalizumab in one case. Neither have previously been demonstrated to increase TB re-activation risk, although this must be interpreted with caution as we cannot contextualise these occurrences as relative risks of re-activation and our data do not allow testing of causation.
Serial testing
It was possible to pair a proportion of the IGRAs by identifying sequential tests conducted in the same patient. We identified 6500 pairs of T-SPOT.TB assays (i.e. serial testing in the same patient). Overall, 1443 (22.2%) were for those on biologics and 5057 (77.8%) were for those not on biologics. Of the 6500 paired IGRAs, 89 were conversions (1.4%). In those on biologics, conversions accounted for 18/1443 pairs (1.2%) compared with 71/5057 (1.4%) in those not on biologics, with no statistically significant difference between the groups (p=0.747, χ2=0.104). Reversions occurred in 70 pairs (1.1%). In those on biologics, reversions accounted for 21/1443 pairs (1.5%), whereas in those not on biologics, reversions accounted for 49/5057 pairs (1.0%), again a difference which did not reach statistical significance (p=0.152, χ2=2.06).
In 395 of the 6500 paired T-SPOT.TB assays a borderline first result occurred. In this subgroup of paired IGRAs, 56 were from those on biologics. The second result was negative in 31 (55.4%), positive in four (7.1%), borderline in 11 (19.6%) and indeterminate in four (7.1%). In 339 paired tests in those not on biologics who initially had a borderline result, the subsequent result was negative in 164 (48.4%), positive in 90 (26.5%), borderline in 36 (10.6%) and indeterminate in 20 (5.9%). The outcomes of the second IGRAs, tested with Fisher's exact test between biologic or nonbiologic groups, were significantly different (p=0.007).
T-SPOT.TB performance
Without data on LTBI treatment, test performance was assessed against active TB diagnosis using the LTBR. Sensitivity analyses are presented with caveats due to the lack of LTBI treatment data; thus, the data only describe the ability to identify active TB. Specificity and NPV analyses were performed using three clinical decision models: the first modelled test performance where borderline results were disregarded, simulating a scenario where clinicians repeat IGRAs until a clear positive or negative result is obtained; the second included borderline results within the positive test results, simulating clinicians assuming all borderline results represent LTBI; and the third grouped borderline results with negative results, simulating clinicians taking the same reassurance from borderline results as they would from negative results. Each approach retained similar high NPVs and specificities remained high regardless of how borderline results were interpreted (table 5).
Selected interferon-γ release assay performance with different models, considering borderline results
Recognising the important confounder that some patients with a positive IGRA result will subsequently undergo treatment for LTBI, we re-assessed the performance of the assays excluding those who had ever been dispensed medication which could be used for TB treatment (table 6). This approach sought to overcome shortcomings in the scope of our datasets, e.g. where patients continue a part of their course outside our institution and their treatment data are unavailable. An unavoidable consequence is that patients treated for other indications (e.g. a short course of levofloxacin for a lower respiratory tract infection) will likely be excluded. The original 4075 T-SPOT.TB IGRAs included in table 5 were reduced to 3466 assays.
Selected interferon-γ release assay performance for patients on biologics comparing those with and without any courses of latent tuberculosis (TB) infection treatment, excluding borderline results
Discussion
This study describes a large cohort of patients who underwent T-SPOT.TB testing in a low TB incidence setting. The subpopulation of interest were patients on biologic therapy. Timing of these IGRAs suggests that the majority were conducted as screening tests prior to starting biologics, in keeping with local and international guidance. Those on biologics were less likely to have positive results than the population tested as a whole. However, indeterminate results were more common. The significance of this is unclear but is likely related to these cases having an abnormal immunological response or being on other anti-inflammatories or disease-modifying agents. Notably neither the rate of conversions nor the number of reversions appeared to differ between those on and not on biologics.
We identified 19 patients on biologics who developed active TB after biologic initiation: an incidence rate of 55.1 per 100 000 patient-years. This appears significantly higher than the average incidence in London during the period studied (25.1 per 100 000). It is likely that this difference is partly due to a direct result of biologic therapy and confounding factors not accounted for by our analysis, including concomitant steroid use.
Despite undergoing screening, at least eight patients subsequently developed active TB. This suggests that even perfect adherence to screening prior (and, if relevant, preventative treatment) to starting biologic therapy would not prevent all instances of subsequent active TB. The identification of various risk factors in those who developed active TB suggests that caution should be taken in patients with a history of malignancy, given the potential for compounded risk from the immune modulation from the disease as well as immunosuppression. No subgroup of biologics, as delineated by local guidance on TB re-activation risk, had a significant difference in TB prevalence when compared with the biologic population as a whole, which may reflect underpowering. In our cohort, some developed TB despite being on low-risk biologic agents, although all were noted to have had other drugs that are likely associated with increased risk of re-activation. This may indicate that the presence or absence of biologic agents is insufficient as an arbiter of screening and that clinicians should consider a composite of factors (supplementary table S1).
Borderline results, when repeated, most commonly reverted to negative and were only positive in 7.1% of cases when on biologics, which was significantly less than those not on biologics. In the latter group, 26.5% became positive when repeated. Our data support the approach of repeating borderline tests, potentially identifying LTBI which may benefit from treatment prior to biologic commencement.
The high NPV for T-SPOT.TB assays is reassuring, signalling that test performance is not compromised despite concerns about immunosuppression affecting IFN-γ release. Similarly reassuring is the consistency of the NPV when borderline results are assumed to be negative. In clinical practice, blanket assumptions in this manner would be unwise. Our data suggest such interpretation would change little in the performance of the test.
Given the nature of evaluating a large retrospective cohort, this study has several limitations. Data linkage was pragmatic and optimised for the datasets obtained, but several factors could not be collated and hence may introduce a risk of error. We were unable to compare TB rates directly against a nonbiologic population with matched disease groups. The delimited time period studied and the data being provided by a single laboratory may mean that some external relevant tests were not identified. An assumption in our analysis is that all IGRAs were undertaken for screening purposes, but we are unable to confirm this. We were also unable to confirm whether patients were immunosuppressed at the time of testing and we lack information on important confounding factors, such as country of birth. From the 19 patients who developed active TB, only 16 had available medical notes which guided their analysis. The pharmacy data did not contain information about the indications for the TB medications prescribed, resulting in the adoption of a cumulative dose calculation to estimate whether patients received medication for TB as an indication. QFT-G data were not included in this analysis.
Our results should be interpreted cautiously. IGRAs are not used to rule out active TB; reaching a diagnosis of active TB by imaging and microbiology remains a pragmatic “gold standard”. The high NPV would appear to reflect the low incidence of TB generally and imperfectly accounts for LTBI treatment. Borderline results remain an area of significant uncertainty, but these results suggest that they are worth repeating and that they do not indicate a need to start TB treatment.
Conclusions
We describe a large population of patients on biologics who underwent T-SPOT.TB testing. We identified instances where active TB occurred despite reasonable adherence to screening protocols. Our results reflect the established consensus that these patients are at higher risk of TB re-activation. It is important to ensure that patients who test negative are made aware of this and that they are advised to seek medical attention if they subsequently develop symptoms consistent with TB. Conversely, negative and even borderline T-SPOT.TB results in this low TB incidence population correspond to a very low risk of subsequently developing active TB.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00193-2022.SUPPLEMENT
Acknowledgements
The authors would like to acknowledge Jacqui Carless of Public Health England (London, UK) for technical support in obtaining and preparing London TB Registry data, the informatics team at North West London Pathology (London, UK) for providing key laboratory report datasets and Darragh Murphy of Imperial College Healthcare NHS Trust (London, UK) for their support in obtaining pharmacy data. K. Kumar is an Imperial 4i Clinician Scientist at Imperial College London (London, UK).
Footnotes
Provenance: Submitted article, peer reviewed.
Author contributions: J. Cafferkey: study design, dataset processing and collation, data analysis, and drafting of the manuscript; Y. Padayachee: study design, manual data collection and analysis, literature review, and drafting of the manuscript; S. Kostich: manual data collection, literature review and drafting of the manuscript; K. Kumar: study design, data interpretation and critical review of the manuscript; P. Jewell: data collection, study design and critical review of the manuscript; M. Patel: data collection, pharmacy advice and critical review of the manuscript; A. Chavda: data collection and pharmacy advice; A. Cox: data interpretation, critical review of the manuscript and lead scientist of laboratory performing assays; M. Park: study design, data interpretation, critical review of the manuscript and project supervision; G. Russell: dataset identification and critical review of the manuscript; M. Coleman: dataset identification and critical review of the manuscript; L. Martin: dataset identification, analysis advice and critical review of the manuscript; O.M. Kon: study design, data interpretation, critical review of the manuscript and project supervision.
Conflict of interest: J. Cafferkey reports the following relationships outside the submitted work: grants or contracts from Royal College of Emergency Medicine, NHS Lothian and University of Edinburgh; support for attending meetings and/or travel from Edinburgh Anaesthesia Research and Education Fund; current member of the Regional Ethics Committee, South East Scotland. K. Kumar received support for the present manuscript from the National Institute for Health Research Imperial Biomedical Research Centre (funding for clinical PhD and salary at Imperial College London), Lee Family endowment to the Faculty of Medicine at Imperial College London (funding for clinical PhD and salary at Imperial College London). M. Patel reports the following relationships outside the submitted work: consulting fees received from Takeda and Jansen; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Jansen – Guidelines in Practice; support for attending meetings and/or travel from Jansen; and participation on a Data Safety Monitoring Board or Advisory Board for Takeda, Pfizer, Jansen, Celltrion and Mylan. A. Chavda has received an honorarium for a manuscript from Shiongi for a case report on Cefidericol. M. Park received support for the present manuscript from the National Institute for Health Research Imperial Biomedical Research Centre. M. Coleman has received payment from Gilead as support for educational lecture talks. The remaining authors have nothing to disclose.
Support statement: K. Kumar, M. Patel and O.M. Kon are supported by the National Institute for Health Research (NIHR) Imperial Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. K. Kumar is also supported by the Lee Family endowment to the Faculty of Medicine at Imperial College London.
- Received April 26, 2022.
- Accepted August 18, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org










