





Figures
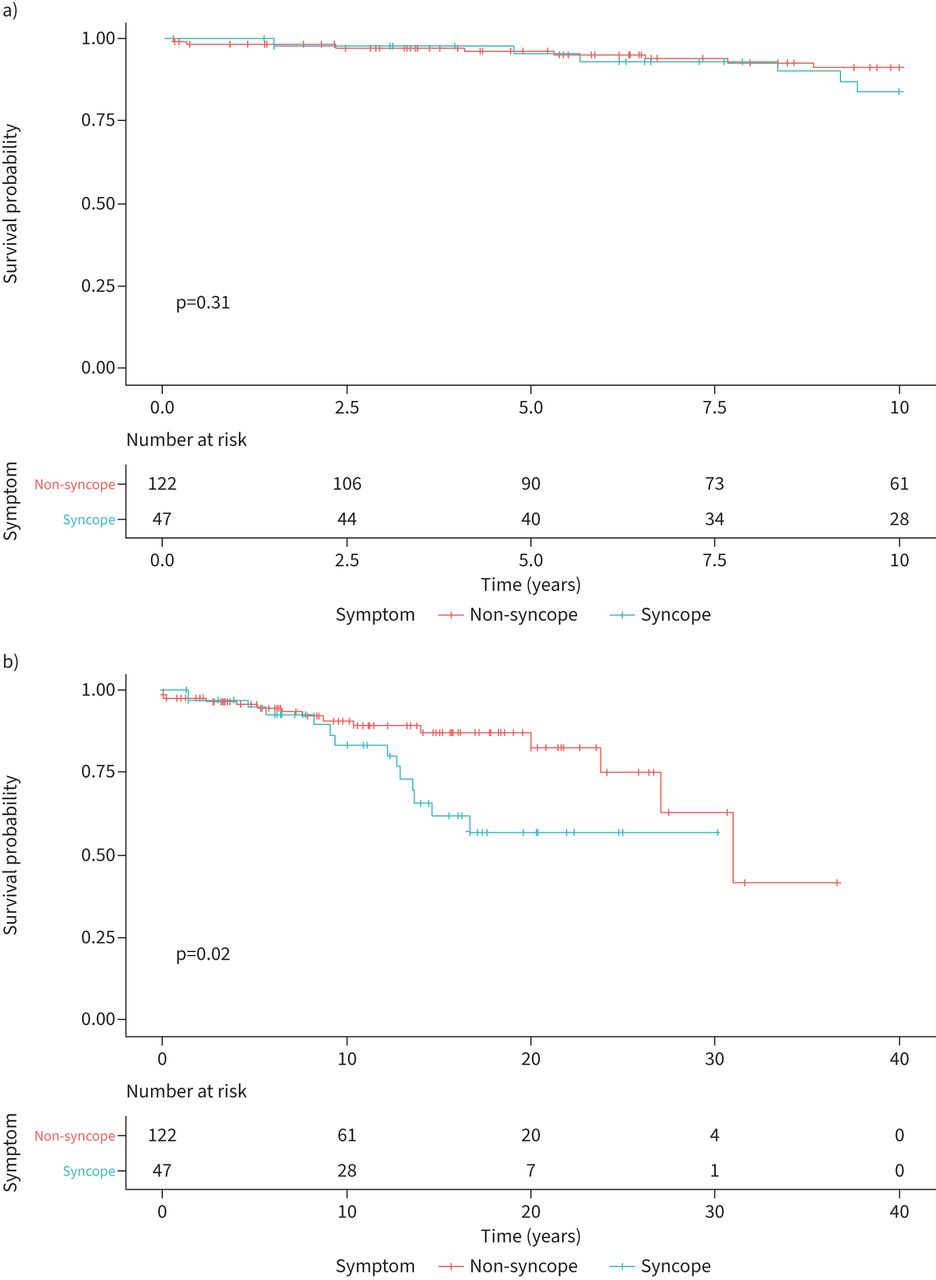
- FIGURE 1
Survival in pulmonary arterial hypertension patients with and without syncope. a) Survival probability over time (in years) showed no difference in survival at 10 years between those with syncope during their clinical course compared to those without. b) Patients with syncope had significantly worse survival over the entire follow-up period.
- FIGURE 2
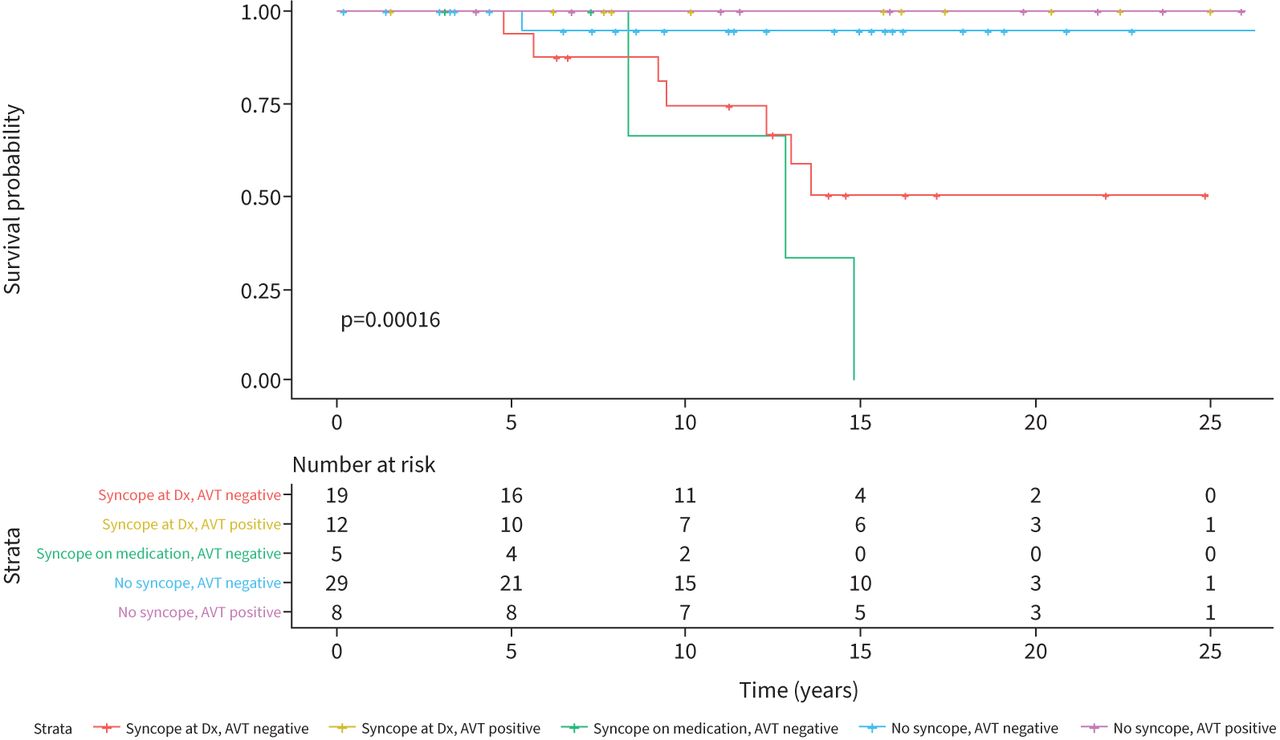
Survival in patients with Group 1 pulmonary arterial hypertension stratified by syncope and acute vasodilator testing (AVT) response. a) There was no significant difference in survival at 10 years regardless of syncope or AVT response. b) Over the entire follow-up period (range 0.17–30.2 years), those with and without syncope and positive response to AVT had 100% survival. Those with syncope and without response to acute vasodilator testing had the worst survival, with the poorest survival in patients with syncope on medications. Dx: diagnosis.
- FIGURE 3
Survival of idiopathic pulmonary arterial hypertension patients stratified by syncope and acute vasodilator testing (AVT) response. All patients with idiopathic pulmonary arterial hypertension who responded to AVT had 100% survival regardless of syncope. Those with syncope and without response to acute vasodilator testing had the worst survival. Dx: diagnosis.


{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Patient characteristics
Syncope Non-syncope p-value Subjects n 47 122 Sex, female 29 (62) 66 (54) 0.40 Median age years 7.9 (0.4–19) 3.0 (0–18.4) 0.002 Symptoms Dyspnoea on exertion 43 (91) 118 (97) 0.08 Chest pain 20 (43) 30 (25) 0.022 Failure to thrive 9 (19) 40 (33) 0.075 Fatigue 34 (72) 57 (47) 0.003 PAH classification Idiopathic PAH 36 (76) 37 (30) <0.00001 Heritable PAH 3 (6) 2 (2) 0.13 APAH-CHD 10 (21) 79 (65) <0.00001 Repaired 5 (50) 53 (67) 0.29 Unrepaired 5 (50) 26 (33) APAH-CTD 1 (2) 4 (3) 1 APAH–portal hypertension 0 2 (1) 1 Data are expressed as median (range) or n (%) unless indicated otherwise. Bold p-values represent statistically significant differences. PAH: pulmonary arterial hypertension; APAH: associated pulmonary hypertension; APAH-CHD: PAH associated with congenital heart disease; APAH-CTD: PAH associated with connective tissue disease.
- TABLE 2
Cardiac catheterisation data at presentation
n Syncope at diagnosis# n Syncope on medication¶,+ n Non-syncope§ p-value Baseline Mean RAP mmHg 7 (5–10) 7 (6–10) 7 (6–9) 0.86 Mean PAP mmHg 53 (37–65) 66.5 (51.8–72) 48.5 (36–64) 0.18 sPAP/sSAP 0.80 (0.50–0.99) 0.83 (0.76–1.10) 66 0.75 (0.50–0.95) 0.47 PVRi WU·m2 13.7 (8.8–22.0) 20.1 (9.2–25.1) 66 9.05 (5.3–14.5) 0.04 Rp/Rs 30 0.7 (0.5–1) 5 0.7 (0.3–1.5) 59 0.6 (0.33–0.94) 0.42 CI L·min−1·m−2 3.0 (2.2–3.8) 2.8 (2.5–3.2) 66 3.5 (2.5–4.2) 0.19 AVT with iNO 5 64 Mean RAP mmHg 25 6 (4–8.5) 3 7 (2–8) 44 7 (6–8.5) Mean PAP mmHg 35 38 (27–60) 63 (53–66.5) 37.5 (28–56.5) 0.15 sPAP/sSAP 34 0.60 (0.40–0.92) 0.77 (0.67–1.16) 59 0.65 (0.46–0.89) 0.30 PVRi WU·m2 33 9.3 (5.1–17.3) 15.1 (11.9–19.5) 61 6.5 (3.7–11) 0.02 Rp/Rs 21 0.46 (0.29–0.72) N/A 33 0.45 (0.21–0.83) 0.99 CI L·min−1·m−2 33 3.2 (2.4–3.8) 3.1 (2.7–3.8) 58 3.6 (2.6–4.6) 0.18 AVT responders (Barst) 14 (40) 0 15 (22) 0.047 AVT responders (Sitbon) 8 (23) 0 9 (13) 0.27 Data are expressed as median (interquartile range) or n (%). Bold p-values represent statistically significant differences. n: number of patients; RAP: right atrial pressure; PAP: pulmonary artery pressure; sPAP/sSAP: ratio of pulmonary artery/systemic arterial systolic pressure; PVRi: indexed pulmonary vascular resistance; Rp/Rs: ratio of pulmonary vascular resistance/systemic vascular resistance; CI: cardiac index; AVT: acute vasodilator testing; iNO: inhaled nitric oxide. #: n=36; ¶: n=6; +: one patient with syncope on medication did not have a catheterisation available from the time of diagnosis; §: n=67.
- TABLE 3
Catheterisation data with acute vasodilator testing (AVT) for syncope patient responders versus non-responders using Barst criteria
n AVT responders# n AVT negative with syncope at diagnosis¶ n AVT negative with syncope on medications+ p-value Room air Mean RAP mmHg 6.5 (3–11) 7 (5–9) 9 (8–10) 0.36 Mean PAP mmHg 49 (32–66) 57 (43–70) 67 (61–81) 0.12 PVRi WU·m2 11.1 (8.6–22) 16.3 (8.7–26) 6 20.0 (7.8–26.3) 0.80 Rp/Rs 11 0.7 (0.4–1) 20 0.9 (0.7–1) 6 1.3 (0.7–2.4) 0.14 CI L·min−1·m−2 2.8 (2.3–3.9) 20 2.98 (1.9–3.6) 3.8 (2.2–4.4) 0.45 AVT with iNO Mean RAP mmHg 9 6 (4–7) 15 8 (5–9) 6 9.5 (7.3–10.3) 0.07 Mean PAP mmHg 28 (20–31)§ 58 (41–77) 64 (61–82) 0.0003 PVRi WU·m2 12 5.1 (3.8–8.0)§ 16.5 (9.3–22.7) 5 22.5 (7.5–26.9) 0.002 Rp/Rs 7 0.2 (0.2–0.4)§ 13 0.7 (0.5–1.1) 5 1.1 (0.5–2.3) 0.0015 CI L·min−1·m−2 3.3 (2.6–3.9) 20 3.3 (2.2–3.8) 3.4 (2.4–4.2) 0.72 Data are expressed as median (interquartile range). Bold p-values represent statistically significant differences between AVT responders and AVT negative. One patient who responded to AVT on her initial catheterisation (included in that category in table 1) lost AVT response by time of syncope as reflected in her later catheterisation used here. RAP: right atrial pressure; PAP: pulmonary artery pressure; PVRi: indexed pulmonary vascular resistance; Rp/Rs: ratio of pulmonary vascular resistance/systemic vascular resistance; CI: cardiac index; iNO: inhaled nitric oxide. #: n=14; ¶: n=21; +: n=7; §: represents statistically significant differences on room air compared to AVT.
- TABLE 4
Catheterisation data with acute vasodilator testing (AVT) for syncope patient responders versus non-responders using Sitbon criteria
n AVT responders# n AVT negative with syncope at diagnosis¶ n AVT negative with syncope on medications+ p-value Room air Mean RAP mmHg 8 (1–16) 7 (5–9) 9 (8–10) 0.33 Mean PAP mmHg 52 (41–66) 54.5 (32–69.8) 67 (61–81) 0.15 PVRi WU·m2 19.5 (11.8–23.7) 14.2 (8.2–24.5) 6 20.0 (7.8–26.3) 0.67 Rp/Rs 6 0.7 (0.6–0.8) 25 0.9 (0.5–1) 6 1.3 (0.7–2.4) 0.22 CI L·min−1·m−2 2.3 (1.8–3.2) 27 3.1 (2.3–3.8) 3.8 (2.2–4.4) 0.15 AVT with iNO Mean RAP mmHg 4 6 (3–9) 20 6.5 (5–8.8) 6 9.5 (7.3–10.3) 0.13 Mean PAP mmHg 29 (28–31) 52.5 (26.3–74.8) 64 (61–82) 0.01 PVRi WU·m2 5 7.9 (6–8) 13.2 (4.7–20.9) 5 22.5 (7.5–26.9) 0.22 Rp/Rs 3 0.4 (0.2–0.4) 17 0.7 (0.3–1) 5 1.1 (0.5–2.3) CI L·min−1·m−2 3.1 (2.6–4.4) 27 3.4 (2.3–3.8) 3.4 (2.4–4.2) 0.73 Data are expressed as median (interquartile range). Bold p-value represents statistically significant difference between AVT responders and AVT negative by Sitbon criteria. RAP: right atrial pressure; PAP: pulmonary artery pressure; PVRi: indexed pulmonary vascular resistance; Rp/Rs: ratio of pulmonary vascular resistance/systemic vascular resistance; CI: cardiac index; iNO: inhaled nitric oxide. #: n=7; ¶: n=28; +: n=7.
- TABLE 5
Treatment at last follow-up
Syncope AVT+ AVT– Non-syncope AVT+ AVT– p-value (syncope versus non-syncope) Subjects n 42 14 28 67 14 53 CCB for vasoresponsiveness 10 (24) 10# 0 6 (6) 6# 0 0.03 CCB monotherapy 3 (6) 3¶ 0 3 (3) 3¶ 0 0.67 Single PAH therapy 6 (14) 4 2 18 (27) 5 13 0.12 Dual PAH therapy 13 (31) 3 10 11 (16) 1 10 0.07 Triple PAH therapy 18 (43) 3¶ 15 23(34) 3 21 0.37 No medication 2 (4) 1 1 12 (18) 2 10 0.046 IV/SQ prostanoid 20 (48) 1 (7) 19+ (68) 15 (22) 1 (7) 14 (26) 0.006 Data are expressed as n or n (%). Bold p-values represent statistically significant differences between patients with and without syncope. AVT: acute vasodilator testing; CCB: calcium channel blocker; PAH: pulmonary arterial hypertension; IV: intravenous; SQ: subcutaneous. #: p for AVT+ versus AVT– <0.00001; ¶: p for AVT+ versus AVT– <0.05 (for syncope CCB only, p=0.03; for syncope triple PAH therapy, p=0.047; for non-syncope CCB only, p=0.007); +: p for AVT+ versus AVT– =0.0002.
- TABLE 6
Cardiac catheterisation data with acute vasodilator testing for idiopathic pulmonary arterial hypertension patients
n Syncope# n Non-syncope¶ p-value Baseline Mean RAP mmHg 7 (5–10) 6 (5–8) 0.45 Mean PAP mmHg 54 (40–69) 52 (37–76) 0.90 sPAP/sSAP 0.81 (0.58–1.00) 0.84 (0.55–1.10) 0.74 PVRi WU·m2 16.7 (9.3–24.8) 11.0 (5.5–20.2) 0.10 Rp/Rs 28 0.75 (0.60–1.00) 31 0.7 (0.40–1.10) 0.51 CI L·min−1·m−2 2.7 (2.0–3.4) 34 3.55 (2.8–4.6) 0.0047 AVT with iNO 34 Mean RAP mmHg 24 7 (4.5–8.5) 27 6 (5–8) 0.72 Mean PAP mmHg 44 (27–64) 41 (31–57) 0.88 sPAP/sSAP 33 0.70 (0.40–0.93) 33 0.70 (0.46–0.91) 0.63 PVRi WU·m2 32 13.2 (5.7–18.9) 33 8.1 (3.6–12.2) 0.037 Rp/Rs 18 0.50 (0.30–0.72) 19 0.45 (0.25–0.90) 0.93 CI L·min−1·m−2 33 3.3 (2.5–3.7) 33 3.8 (2.7–5.3) 0.013 AVT responders (Barst) 12 (35) 8 (23) 0.19 AVT responders (Sitbon) 6 (18) 5 (14) 0.70 Data are expressed as median (interquartile range) or n (%). Bold p-values represent statistically significant differences. n: number of patients; RAP: right atrial pressure; PAP: pulmonary artery pressure; sPAP/sSAP: ratio of pulmonary artery/systemic arterial systolic pressure; PVRi: indexed pulmonary vascular resistance; Rp/Rs: ratio of pulmonary vascular resistance/systemic vascular resistance; CI: cardiac index; AVT: acute vasodilator testing; iNO: inhaled nitric oxide. #: n=34; ¶: n=35.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00223-2022.SUPPLEMENT










