





Abstract
Background Phase III regulatory trials show that anti-interleukin (IL)-5 biologics efficiently reduce exacerbations and the use of maintenance oral corticosteroids (mOCS) in patients with severe eosinophilic asthma. However, patients eligible for these trials differ significantly compared with real-life severe asthma populations. Therefore, our aim was to explore efficacy in a real-life setting. The Danish Severe Asthma Register (DSAR) is a complete, nationwide register that comprises all Danish patients on biological therapy for severe asthma.
Methods This prospective study identified patients in the DSAR who were complete responders to anti-IL-5 biologics after 1 year of treatment. A complete response was defined as resolution of the parameter setting the indication, i.e. recurrent exacerbations and/or use of mOCS.
Results A total of 289 out of 502 (58%) patients were complete responders to anti-IL-5 biologics after 12 months. Complete responders had greater improvements in forced expiratory volume in 1 s and Asthma Control Questionnaire (ACQ) score compared with noncomplete responders (Δ 210 versus 30 mL; p<0.0001 and Δ −1.04 versus −0.68; p=0.016, respectively). A complete response was predicted by age at onset, less severe disease at baseline (i.e. no mOCS and lower ACQ score) and higher blood eosinophils.
Conclusions More than half of Danish patients treated with anti-IL-5 biologics for severe asthma achieve a complete response to treatment, thereby becoming free from asthma exacerbations and the need for mOCS. Complete responders also achieved superior effects on lung function and symptoms compared with noncomplete responders.
Abstract
More than half of all Danish patients with severe asthma receiving anti-IL-5 in a real-life setting achieve a complete response to treatment, i.e. they become free from exacerbations and the need for oral corticosteroids https://bit.ly/3zMMB75
Introduction
Most asthma patients have mild-to-moderate disease that remains under control on low- or medium-dose inhaled corticosteroids (ICS) with or without a second controller. However, some patients have severe disease that requires both high-dose ICS and a second controller. It is estimated that 4–8% of asthma patients have severe asthma [1, 2]. These patients have a higher burden of symptoms and exacerbations, and uncontrolled severe asthma is associated with higher healthcare costs and more frequent admissions to hospital, compared with patients with mild or moderate disease [3].
Severe asthmatic subjects with an eosinophilic phenotype are potentially candidates for treatment with anti-interleukin (IL)-5 biologics. Currently, three anti-IL-5 biologics, targeting IL-5 or its receptor, are marketed: mepolizumab, reslizumab and benralizumab. Phase III randomised controlled trials (RCTs) show that anti-IL-5 biologics efficiently reduce exacerbation rates [4–8] and the need for maintenance oral corticosteroids (mOCS) [9–11] compared with placebo. However, it is unclear if these results can be transferred to real-life patients with severe asthma. Patients included in regulatory trials are subjected to strict inclusion and exclusion criteria, and can often differ significantly from real-life patients in terms of baseline characteristics such as age, comorbidities, lung function and smoking status [12, 13]. Because of this potentially significant discrepancy, the effects of anti-IL-5 biologics should be evaluated in a real-life setting.
Data from real-life patients suggest that anti-IL-5 biologics have a similar or even superior effect to that shown in RCTs; however, these observations are mostly based on fairly small and selected populations [14–26]. Real-life experience of anti-IL-5 biologics has brought the recognition that some patients have a much better response to therapy compared with others and the term “super-responder” has emerged. There is at present no international consensus on what constitutes a “super-responder” to biological therapy in severe asthma [27], but the term has been used in several papers with varying criteria, including, but not limited to, exacerbation rate, symptom control and lung function [28–31].
In the present study, we aimed to describe the proportion of patients with severe eosinophilic asthma having received anti-IL-5 treatment for at least 12 months, who obtained a complete response in a representative nationwide cohort. A complete response was defined as a complete resolution of the clinical problems that set the indication for treatment, i.e. exacerbations and/or use of mOCS.
We utilised data from the Danish Severe Asthma Register (DSAR), consisting of all Danish patients treated with biologics for severe asthma, and assessed the proportion of patients with a complete response after 12 months of treatment, together with the effect on other clinical outcomes and biomarkers, as well as baseline predictors of a complete response.
Methods
Study participants
The DSAR was established in 2017 and comprises all Danish patients receiving biological treatment (anti-IgE, anti-IL-5 and anti-IL-4/13) for severe asthma [32]. In the present study, we analysed data for all patients with available data after 12 months of anti-IL-5 therapy, to evaluate the effectiveness of anti-IL-5 biologics after the first 12 months of treatment, and identified predictors of a complete response. Only patients who completed 1 year of treatment are included in this article.
Informed consent was collected electronically along with patient-reported outcomes (PROs).
The DSAR has been approved by the Capital Region of Denmark (VD-2018-31) and all patients provide informed consent that their data can be used for research purposes.
Indication for biologics in the DSAR
In Denmark, the decision to start an asthma patient on biological therapy is made by an asthma specialist. Initiation of biological treatment should be preceded by a systematic assessment to differentiate severe asthma from difficult-to-treat asthma [33]. According to the Danish Medicines Council, anti-IL-5 therapy is indicated for patients with severe asthma with lack of disease control together with evidence of eosinophilic inflammation. Lack of disease control is defined as an annual rate of exacerbations, requiring rescue OCS, of ≥2 or a need for daily OCS >50% of the time. Efficacy of anti-IL 5 therapy is initially assessed by an asthma specialist after 4 months of treatment and again after 12 months. If the treatment is not efficacious or well tolerated, it is stopped.
Measurements
In the DSAR, information is collected prospectively and according to a set protocol, with all patients being evaluated thoroughly at baseline prior to commencing biological treatment. Subsequently, information is collected prospectively at 4 and 12 months after initiation of treatment. Information about lung function, exacerbations, medications, comorbidities, PROs and inflammatory markers before initiation of biological treatment was used to identify predictors of complete responders, and information at 12-month follow-up was used to evaluate the treatment efficacy. The use of mOCS is registered in the DSAR; however, the precise indication (e.g. asthma control or adrenal insufficiency) is not.
Definition of a complete response
In this study, we defined a complete response to anti-IL-5 biologics as no rescue courses of OCS for exacerbations and no use of mOCS after 12 months of treatment. These outcomes are shown to be significantly improved by anti-IL-5 biologics in several RCTs and therefore are key elements of the clinical indication for initiation of anti-IL-5: indications include either recurrent exacerbations or regular use of mOCS [34], as opposed to a high symptom score or impaired lung function which in themselves do not suffice to qualify the patient for anti-IL-5 treatment. Therefore, a complete response to treatment was defined as a resolution of the clinical parameter setting the indication, i.e. recurrent exacerbations and/or use of mOCS.
Statistical analyses
To assess the proportion of responders and their characteristics, patients were categorised into complete responder and noncomplete responder groups using the aforementioned definitions. Baseline patient characteristics of the two responder groups were compared using descriptive statistics: the Chi-squared test or Fisher's exact test where applicable for categorical variables, and the t-test and Mann–Whitney U-test for normally distributed and skewed continuous variables, respectively. To evaluate effectiveness of anti-IL-5 biologics on specific outcomes, within-group changes were evaluated by the paired t-test and signed-rank test for normally and nonnormally distributed continuous variables, respectively, whereas categorical variables were compared using McNemar's test.
To describe potential predictors of complete response to anti-IL-5 and adjust for potential confounders, patient characteristics with a p-value <0.20 in univariate analyses were furthermore tested in multivariate logistic regression models, adjusting for age and sex, with response status (complete versus noncomplete) as the dichotomous outcome.
p-values were two-sided with a threshold of p<0.05 to denote statistical significance. All analyses were performed using SAS Enterprise Guide 7.1 (SAS Institute, Cary, NC, USA).
Results
We identified 502 patients who had completed at least 1 year of anti-IL-5 treatment, and for whom information about exacerbations and use of mOCS was available (figure 1 and table 1). Of these, 289 patients (58%) were classified as complete responders with no exacerbations and no use of mOCS after the first year of treatment, and 213 patients (42%) were noncomplete responders, with either use of mOCS and/or exacerbations requiring rescue courses of OCS after the first year of treatment (figure 2). Of the 213 noncomplete responders, 123 (58%) did not fulfil the definition for complete response due to still being on mOCS, while the remaining 90 (42%) still had exacerbations after 12 months of treatment.
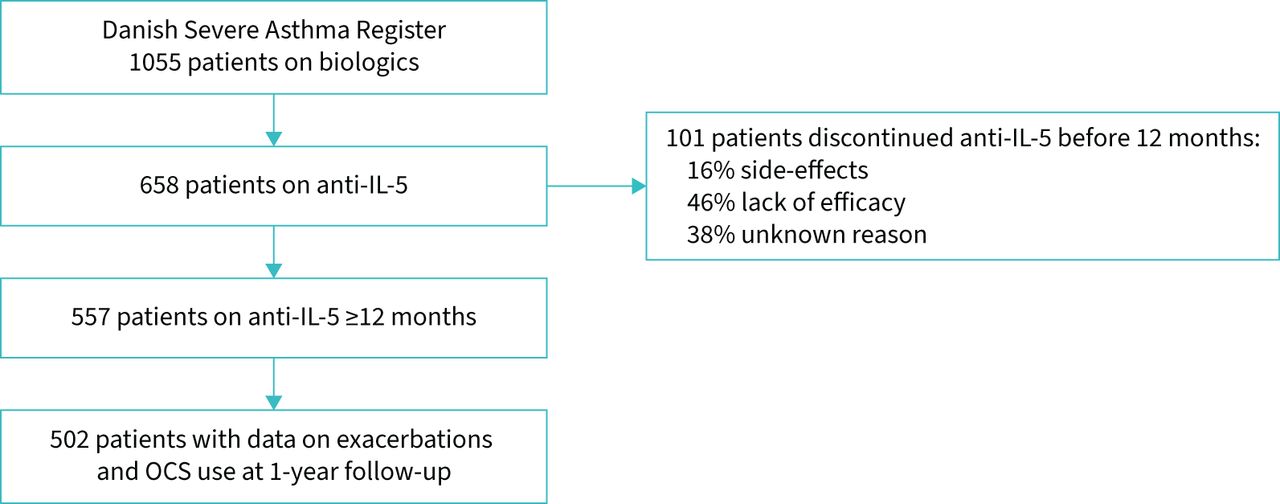
Flowchart of patients from the Danish Severe Asthma Register categorised as complete responders and noncomplete responders. IL: interleukin; OCS: oral corticosteroids.
Patient characteristics at baseline

Proportion of patients who were complete responders after 12 months of anti-interleukin-5 treatment.
Effects of anti-IL-5 in the entire population
Overall, we saw a significant reduction of 80% in exacerbations and the proportion of patients on mOCS was reduced from 37% at baseline to 25% at 1 year (p<0.0001) (table 2). Asthma Control Questionnaire (ACQ) score was also significantly reduced, from 2.49±1.31 to 1.61±1.21 (p<0.0001) at follow-up, with the reduction reaching the minimal clinically important difference of 0.5 [35]. After 1 year of treatment, 55% of patients had well-controlled asthma (ACQ ≤1.5) versus only 28% at baseline (p<0.0001).
Outcomes after 1 year of treatment with anti-interleukin-5 biologics for severe asthma
Overall, FEV1 significantly improved, from a mean±sd of 2.25±0.8 L and 69% predicted at baseline to 2.37±0.88 L and 74% predicted at 12-month follow-up (p<0.0001).
Difference in baseline characteristics between complete responders and noncomplete responders
Complete responders and noncomplete responders were similar in age, body mass index and lung function at baseline (table 3). Fewer women were complete responders (45% versus 54% female noncomplete responders; p=0.038). Complete responders had fewer exacerbations prior to initiation of biologics (2.8 versus 3.43; p=0.049) and a smaller proportion were on mOCS at baseline (18% versus 63%; p<0.0001). Complete responders were generally older at asthma onset (38 versus 32 years; p=0.02) and a larger proportion had late onset >40 years (48% versus 40%; p=0.13). Moreover, complete responders also had shorter duration of disease (20 versus 24 years; p=0.04).
Complete responder versus noncomplete responder characteristics at baseline
Allergic rhinitis, chronic rhinosinusitis and aspirin sensitivity tended to be more prevalent among complete responders, whereas diabetes and obstructive sleep apnoea were more prevalent among noncomplete responders. However, there were no statistically significant differences in comorbidities between the two groups.
Inflammatory markers were similar in complete responders and noncomplete responders with respect to baseline exhaled nitric oxide fraction (FENO) and IgE, whereas complete responders had higher blood eosinophils at baseline (0.40 versus 0.23×109 L−1; p=0.0002).
Type of anti-IL-5 biologic did not differ significantly between the two groups (p=0.125). In the complete responder group 72%, 25% and 3% were on mepolizumab, benralizumab and reslizumab, respectively, whereas among noncomplete responders the distribution was 69%, 23% and 8%, respectively. There was also a similar proportion of switchers in the two groups (23% versus 29%; p=0.08). Smoking status and accumulated lifetime tobacco exposure in ever-smokers did not differ between complete responders and noncomplete responders.
Differences in outcomes between complete responders and noncomplete responders
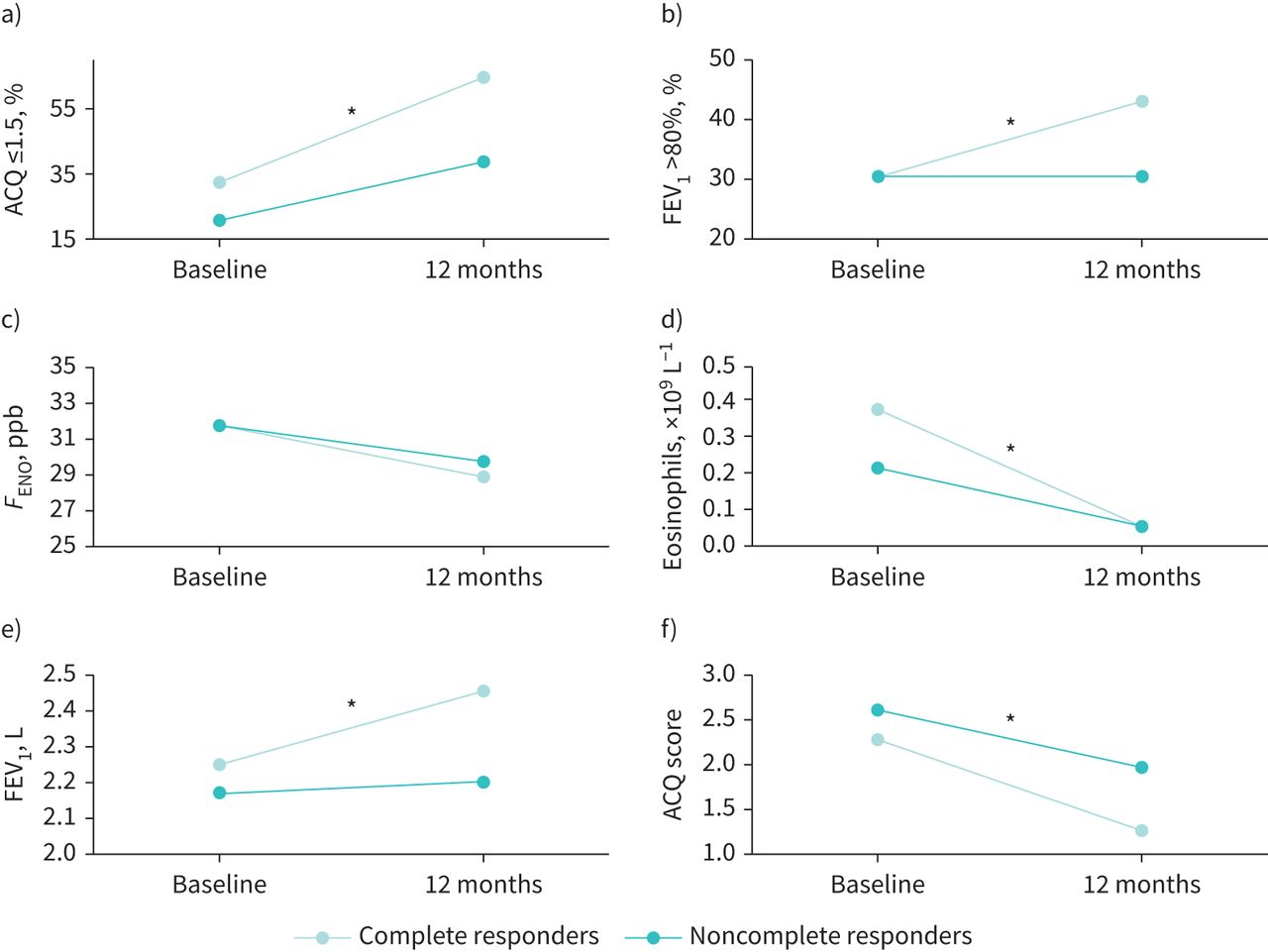
Outcomes other than those that defined a complete response varied significantly between complete responders and noncomplete responders (table 4). Complete responders had better outcomes with regard to lung function, with FEV1 2.47 L (76% predicted) versus 2.21 L (70% predicted) for noncomplete responders (p<0.0001) (figure 3). Complete responders also had better symptom control after 1 year of treatment, with an ACQ score of 1.28 versus 1.99 for noncomplete responders (p=0.016), and a significantly larger proportion of complete responders had ACQ ≤1.5 (67% versus 40%; p<0.0001) (figure 3).
Outcomes for complete versus noncomplete responders after 1 year of treatment with anti-interleukin-5 biologics
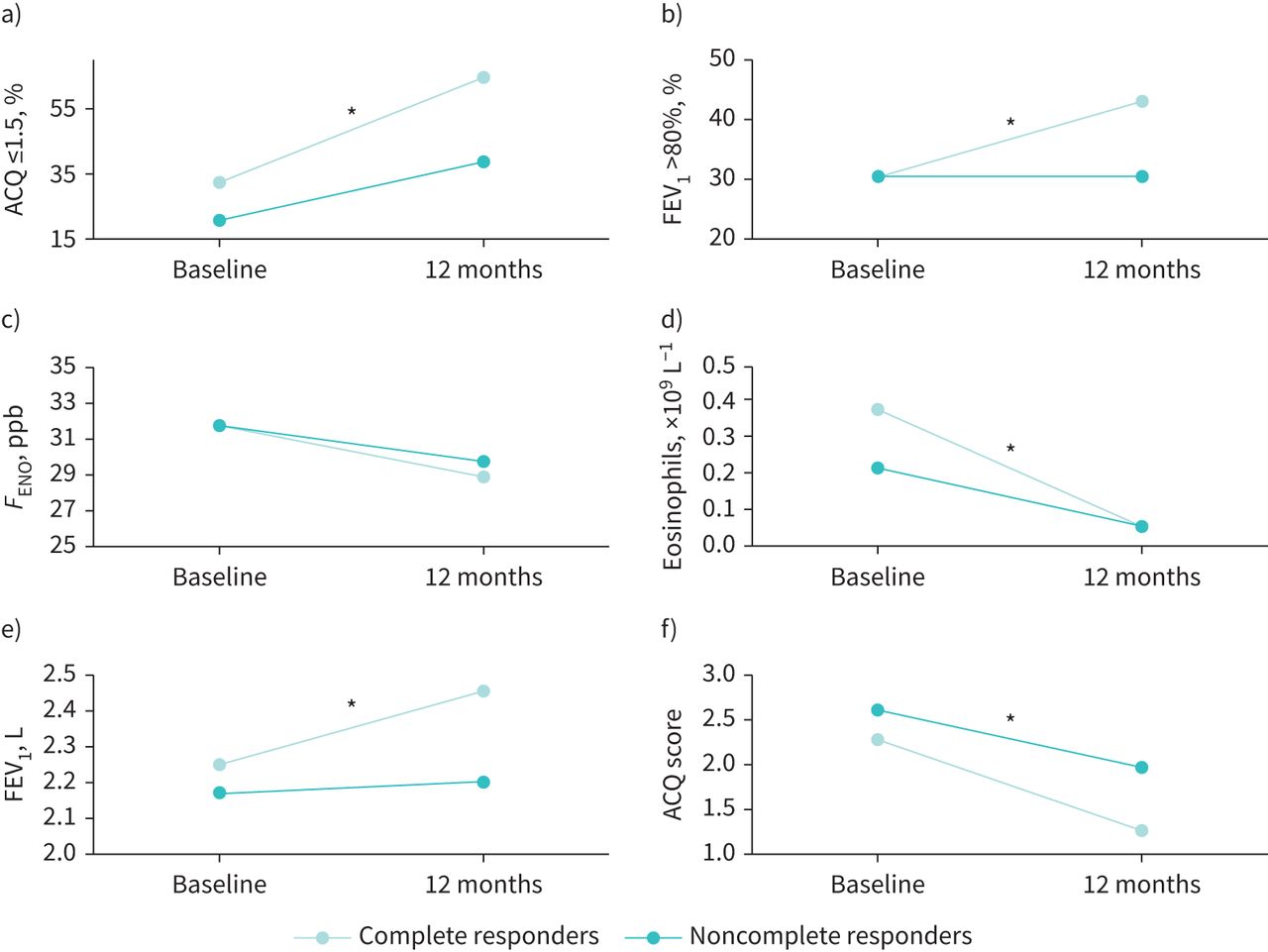
Change in secondary outcomes in complete responders and noncomplete responders after 12 months of anti-interleukin-5 treatment: a) Asthma Control Questionnaire (ACQ) ≤1.5, b) forced expiratory volume in 1 s (FEV1) >80% predicted, c) exhaled nitric oxide fraction (FENO), d) blood eosinophils, e) FEV1 and f) ACQ score. *: significant difference (p<0.05) in change from baseline to 12 months between complete responders and noncomplete responders.
Significant predictors of complete response
In a logistic regression model, younger age at onset of asthma, concomitant diabetes and use of mOCS at baseline predicted not achieving a complete response to anti-IL 5 biologics (figure 4). Furthermore, allergic rhinitis, lower ACQ at baseline and blood eosinophils ≥0.3×109 L−1 predicted a complete response to therapy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Baseline predictors of complete response to anti-interleukin-5 treatment after 12 months. mOCS: maintenance oral corticosteroids; ACQ: Asthma Control Questionnaire; OSA: obstructive sleep apnoea.
Discussion
In this nationwide prospective real-life cohort of all Danish severe asthma patients treated with anti-IL-5 biologics, 58% were complete responders after 12 months, with abrogation of exacerbations and cessation of mOCS. Complete responders also experienced superior improvements in lung function and symptom control compared with noncomplete responders. Complete responders to therapy had less severe disease at baseline (i.e. less use of mOCS, fewer exacerbations and lower ACQ), higher blood eosinophils and later onset of disease.
A British group recently published real-life data from relatively large cohorts of patients on mepolizumab [29] and benralizumab [28] (n=99 and n=130, respectively). In these studies, the term “super-responder” matched our definition of a complete responder. However, the proportions of complete responders in these cohorts were much smaller. Only 28% of patients on mepolizumab and 39% of patients on benralizumab were complete responders compared with 58% in our combined cohort. Noticeably, requirements for initiation of anti-IL-5 are stricter in the UK than in Denmark. Three or four exacerbations, depending on levels of blood eosinophils, are mandatory in the UK if patients are not on mOCS; however, only two are required in Denmark, with the latter criteria of two exacerbations being similar to eligibility criteria in the regulatory RCTs. This difference in response pattern between the cohorts indicates that patients with more severe disease upon commencement of anti-IL-5 treatment are less likely to achieve a complete response to treatment. The British cohorts’ data also revealed that being on mOCS at baseline is a negative predictor of a complete response to anti-IL-5 biologics, just as our data show. A negative influence of mOCS on response to treatment is also reported in other real-life studies of anti-IL-5 biologics [28–30, 36]. This further supports that severity of disease upon commencement of treatment could be a key factor for response, but potentially also longer duration of disease. Additionally, in patients with long-term use of OCS, weaning completely off OCS may be more difficult due to adrenal insufficiency, thereby rendering these patients less likely to achieve a complete response that is defined by cessation of use of mOCS. Additional studies are needed to understand whether initiating biological treatment earlier would lead to improved treatment outcomes, with more patients achieving complete control of their asthma. In our study, we saw a reduction in exacerbations far superior to those shown in the regulatory trials. This superior reduction has also been reported from other larger real-life cohorts [28, 30, 37–39]. This is perhaps to a certain degree due to a placebo effect that is not corrected by a control group receiving placebo. However, it is also likely that real-life patients undergo a systematic assessment of factors contributing to a lack of asthma control prior to commencement of biological treatment. An individual assessment is not easily replaced by a predefined set of inclusion and exclusion criteria that controls which patients are eligible for RCTs, and real-life clinicians may be better at selecting patients who will benefit from treatment.
We also found that higher blood eosinophils predicted a complete response to anti-IL-5 biologics. This is in line with several other studies based on both real-life data [28, 30, 39] and data from RCTs [40, 41].
This study offers, to the best of our knowledge, the largest, complete nationwide anti-IL-5 cohort to date. The cohort is unique in being both nationwide and with prospectively collected data, from prior to initiating treatment and at set time-points. The group is furthermore clearly defined as there are set and agreed indications for initiation of biological treatment for patients in the cohort and they undergo systematic evaluation of other factors driving poor asthma control, e.g. comorbidities, adherence to ICS, etc. However, there are also limitations. Data are reported by healthcare personnel in the clinics providing the treatment and therefore it is not always complete. Furthermore, the decision to initiate biological treatment is up to the clinician and therefore it is possible that some patients do not meet formal requirements for treatment. The effects from treatment that we report, which are mostly superior to results in phase III trials, might be biased by the lack of blinding and placebo control that constitutes real-life data. Poor adherence to ICS may affect the outcome of treatment with biologics negatively [42]. Information on adherence to ICS was not available in the present study, but adherence is routinely checked, at each consultation in all patients on biologics, by assessing redemption of prescriptions for asthma medications in the online Danish medication registry. Hence, we believe that nonadherence to ICS is unlikely to be a major contributor to noncomplete response. Furthermore, our analyses do not include patients who discontinued anti-IL-5 before 12 months of treatment (figure 1). It is also important to note that this study is not appropriate as a head-to-head comparison of the anti-IL-5 biologics because our data include switchers that may have changed from one anti-IL-5 to another for various reasons, including availability, nonresponse or convenience.
Our data suggest that perhaps, in particular, a phenotype of late-onset disease, short duration and with higher blood eosinophils benefits from anti-IL-5 treatment. It may be speculated that this phenotype is associated with a clearer IL-5 drive, as opposed to others, e.g. early-onset, allergic asthma, that perhaps activate more pathways of type 2 inflammation. Our data further suggest that severity of disease (i.e. need for mOCS, number of exacerbations and ACQ) is a key factor in determining response to anti-IL-5 treatment. Very severe asthma (i.e. need for mOCS, an increasing number of exacerbations and high symptom score) was associated with a poorer response to treatment, suggesting that there is a window of severity between qualifying for anti-IL-5 treatment and needing mOCS where patients have optimised effects from treatment. We also found that presence of diabetes predicts a noncomplete response, which could be interpreted as a surrogate marker of severity as it is a well-known side-effect of prolonged OCS use. More severe disease and mOCS were associated with noncomplete response to anti-IL-5, which could be linked to a switch from an eosinophilic drive to an autoimmune drive [36].
Our study shows that complete responders to anti-IL-5 not only achieve remission of outcomes related to the indication for treatment, but they also have superior improvements of symptom score and lung function, which emphasises the importance of identifying patients who will benefit from this treatment. These patients may furthermore potentially fulfil criteria for remission of asthma [43] and describing their long-term prognosis will be an important future research goal. A further important question is obviously whether these patients would be able to stop or down-titrate their biological treatment [44] and studies examining this question are urgently needed. These results also highlight the possible importance of timely intervention with biologics in severe asthma in appropriate candidates and further research is needed to consolidate whether earlier initiation of biologics improves the overall prognosis. Finally, our study shows that blood eosinophils are, for now, the best biomarker to identify patients who particularly benefit from anti-IL-5 biologics, whereas FENO and IgE are not helpful.
Conclusions
More than half of Danish patients on anti-IL-5 were complete responders to treatment, and this group of patients also experienced superior improvements in lung function and symptoms. Complete response is predicted by high blood eosinophils and less severe disease at baseline.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: M.B. Soendergaard has received lecture fees from GlaxoSmithKline, outside the submitted work.
Conflict of interest: S. Hansen has nothing to disclose.
Conflict of interest: A.S. Bjerrum has received lecture fees from AstraZeneca and GlaxoSmithKline, outside the submitted work.
Conflict of interest: O. Hilberg has nothing to disclose.
Conflict of interest: S. Lock-Johansson has nothing to disclose.
Conflict of interest: K.E.J. Håkansson has received unrestricted research grants, paid to his institution, from AstraZeneca and Sanofi Genzyme, outside the submitted work; and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from AstraZeneca, Teva, GlaxoSmithKline and Sanofi Genzyme, outside the submitted work.
Conflict of interest: T.S. Ingebrigtsen has nothing to disclose.
Conflict of interest: C.R. Johnsen has nothing to disclose.
Conflict of interest: L.M. Rasmussen has received payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from AstraZeneca, GlaxoSmithKline, Teva and ALK, outside the submitted work; support for attending meetings and/or travel received from AstraZeneca and Chiesi, outside the submitted work; and participation on data safety monitoring or advisory boards for AstraZeneca, GlaxoSmithKline, Teva and Sanofi, outside the submitted work.
Conflict of interest: A. von Bülow has done consultancy work for Novartis DK, outside the submitted work; lectures and speakers fees received from AstraZeneca, Novartis and GlaxoSmithKline, outside the submitted work; and advisory boards for AstraZeneca and Novartis, outside the submitted work.
Conflict of interest: K.D. Assing has nothing to disclose.
Conflict of interest: J.M. Schmid has nothing to disclose.
Conflict of interest: C.S. Ulrik received payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from AstraZeneca, GlaxoSmithKline, Teva, Sanofi, Orion Pharma, Novartis and Chiesi, outside the submitted work.
Conflict of interest: C. Porsbjerg has received grants or contracts from AstraZeneca, GlaxoSmithKline, Novartis, Teva, Sanofi, Chiesi and ALK, outside the submitted work; consulting fees from AstraZeneca, GlaxoSmithKline, Novartis, Teva, Sanofi, Chiesi and ALK, outside the submitted work; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events, received from AstraZeneca, GlaxoSmithKline, Novartis, Teva, Sanofi, Chiesi and ALK, outside the submitted work; and participation on data safety monitoring or advisory boards for AstraZeneca, Novartis, Teva, Sanofi and ALK, outside the submitted work.
- Received May 16, 2022.
- Accepted June 15, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










