





Abstract
Background This multicentre, international, prospective cohort study evaluated whether patients with pulmonary sarcoidosis living in neighbourhoods with greater material and social disadvantage experience worse clinical outcomes.
Methods The area deprivation index and the Canadian Index of Multiple Deprivation evaluate neighbourhood-level disadvantage in the US and Canada, with higher scores reflecting greater disadvantage. Multivariable linear regression evaluated associations of disadvantage with baseline forced vital capacity (FVC) or diffusing capacity of the lung for carbon monoxide (DLCO) and linear mixed effects models for associations with rate of FVC or DLCO decline, and competing hazards models were used for survival analyses in the US cohort, evaluating competing outcomes of death or lung transplantation. Adjustments were made for age at diagnosis, sex, race and smoking history.
Results We included 477 US and 122 Canadian patients with sarcoidosis. Higher disadvantage was not associated with survival or baseline FVC. The highest disadvantage quartile was associated with lower baseline DLCO in the US cohort (β = −6.80, 95% CI −13.16 to −0.44, p=0.04), with similar findings in the Canadian cohort (β = −7.47, 95% CI −20.28 to 5.33, p=0.25); with more rapid decline in FVC and DLCO in the US cohort (FVC β = −0.40, 95% CI −0.70 to −0.11, p=0.007; DLCO β = −0.59, 95% CI −0.95 to −0.23, p=0.001); and with more rapid FVC decline in the Canadian cohort (FVC β = −0.80, 95% CI −1.37 to −0.24, p=0.003).
Conclusion Patients with sarcoidosis living in high disadvantage neighbourhoods experience worse baseline lung function and more rapid lung function decline, highlighting the need for better understanding of how neighbourhood-level factors impact individual patient outcomes.
Abstract
Greater neighbourhood disadvantage is associated with worse baseline lung function and more rapid lung function decline in patients with sarcoidosis in both US and Canadian cohorts, highlighting the impact of socioeconomic disparities in this population https://bit.ly/3R8gUuc
Introduction
Sarcoidosis is a multisystem disease characterised by granulomatous inflammation with up to 97% of patients having evidence of intrathoracic involvement [1–3]. The prevalence of sarcoidosis is estimated at 60 per 100 000 persons in the US [4] and 143 per 100 000 persons in Canada [5]. Sarcoidosis incidence, presence of extrathoracic manifestations, disease progression and mortality are most pronounced in minoritised individuals and women, especially women of Black race [6–12]. Low socioeconomic status (SES) also adversely impacts disease severity, onset of sarcoidosis-related comorbidities, health-related quality of life, disease progression, hospitalisations and mortality in patients with sarcoidosis [6, 13–15]. Furthermore, the economic burden imposed on patients with sarcoidosis can be substantial, especially for the 25–40% of patients with chronic and persistent disease, which most frequently impacts Black, female and elderly patients [16]. These factors have the potential to further entrench disparities in this vulnerable disease population.
Neighbourhood-level socioeconomic factors can be evaluated by metrics such as the area deprivation index (ADI) and the Canadian Index of Multiple Deprivation (CIMD) in the US and Canada, respectively. These indices measure neighbourhood-level disadvantage, which is associated with income, education level, residential and food security, safety and health behaviours that contribute to health disparities for low-income, racialised and other vulnerable communities [17]. Greater neighbourhood-level disadvantage is associated with adverse outcomes in several chronic respiratory diseases [18–21], but the impact of this sociodemographic measure on patients with sarcoidosis remains unknown.
We used two well-defined interstitial lung disease (ILD) registries from the US and Canada to test the hypotheses that greater neighbourhood-level disadvantage, as quantified by the ADI or CIMD, would be associated with worse baseline lung function and more rapid lung function decline in patients with sarcoidosis. Some of the results of these analyses have previously been presented in the form of an abstract.
Methods
Study subjects
US patients with pulmonary sarcoidosis were prospectively enrolled in the University of Pittsburgh Dorothy P. and Richard P. Simmons Center for Interstitial Lung Disease (ILD) Registry between 2000 and 2021. Canadian patients were prospectively enrolled in one of eight Canadian Registry for Pulmonary Fibrosis (CARE-PF) sites across the country between 2015 and 2021 [22]. A small subset of patients were enrolled in preexisting single-centre registries at participating CARE-PF sites prior to 2015. Diagnoses were made by pulmonary physicians with expertise in the diagnosis and management of sarcoidosis.
Adult patients with pulmonary sarcoidosis in either registry were eligible for inclusion. The presence of extrapulmonary manifestations at diagnosis was determined through manual chart review, as was any treatment with corticosteroids, steroid-sparing agents or biologics in the Canadian cohort. Baseline treatment data and some demographic data were ascertained through the University of Pittsburgh Health Record Research Request (R3) Service for the US cohort [23]. Required covariates for inclusion were age at diagnosis, sex and self-defined race. Other covariates collected included smoking history (current, former, never), baseline forced vital capacity (FVC) and diffusing capacity of the lung for carbon monoxide (DLCO). Date of diagnosis was defined as the first visit to the specialist ILD registry centre.
Ethics approval was obtained from the University of Pittsburgh (STUDY20050209) and the University of British Columbia as the coordinating site for CARE-PF (#H19-01989 and #H20-01454).
Neighbourhood-level disadvantage determination
ADI is determined by converting US residential addresses into nine-digit zip codes, which are then matched with a US nationwide ADI dataset based on 2018 American Community Survey data [17, 24]. ADI is reported as a percentile score ranging from 1 to 100, with higher scores reflecting greater neighbourhood disadvantage.
The CIMD is a similar metric to ADI that is determined by matching Canadian postal code with CIMD scores for that dissemination area, which is based on 2016 Canadian Census data [25]. CIMD is measured on a continuous scale using a factor score approach based on four domains of the index, which are residential instability, ethnocultural composition, economic dependency and situational vulnerability. In this analysis, we used the mean factor score of the four dimensions as our continuous exposure, with higher scores reflecting greater disadvantage.
Subsequent analyses were performed using continuous and quartiled ADI or CIMD. Quartiles were formed where approximately equal numbers of patients with sarcoidosis were grouped into each quartile to enable comparison of results between the US and Canadian cohorts. Quartile 1 (Q1) reflected the least disadvantage and quartile 4 (Q4) reflected the greatest disadvantage (cut-offs in supplementary table E1).
Clinical outcomes
Pulmonary function (FVC and DLCO), mortality and lung transplantation status were discerned from specialist clinic records and electronic health records. Baseline FVC and DLCO were defined as the first tests performed within 6 months of diagnosis. Rate of change in FVC and DLCO was determined using all pulmonary function test measurements obtained throughout follow-up. Differences in % pred FVC and DLCO are reported in absolute terms (i.e. an FVC decline of 10% per year would be reported if % pred FVC went from 60% to 50% in 1 year). FVC was determined using US population-referenced Hankinson equations and DLCO using Neas equations in the US cohort [26, 27]. Global Lung Function Initiative equations were used for the Canadian cohort, with variable usage of race-based adjustment [28].
Statistical analyses
Descriptive statistics evaluated demographic, neighbourhood-level disadvantage and censoring characteristics for the two cohorts. Post hoc multivariable linear regression evaluated the association between sex or race and neighbourhood-level disadvantage scores.
The association of ADI or CIMD with baseline % pred FVC and DLCO was evaluated using multivariable linear regression. The association of ADI or CIMD with rate of change in % pred FVC or DLCO was evaluated using linear mixed effects models with random intercepts. Results are reported in unadjusted models, “partially adjusted” models (adjusting for age at diagnosis and sex) and “fully adjusted” models (further adjusting for race and current, former, never or unknown smoking).
As a secondary analysis, competing hazards survival analysis was performed, considering death and transplant as competing outcomes. Survival analysis was not performed in the Canadian cohort as death only occurred in four patients, precluding sufficient power for these analyses. Survival analyses are reported in unadjusted models, “partially adjusted” models (adjusting for pre-specified covariates of age at diagnosis and sex) and “fully adjusted” models (further adjusting for race, smoking history, baseline FVC and baseline DLCO).
Covariates in all models were chosen a priori given associations with sarcoidosis morbidity and mortality [7], and potential interactions with neighbourhood disadvantage [29, 30]. Observations with missing covariates in adjusted analyses were dropped (i.e. no imputation).
Analyses were performed using R (version 4.0.2, www.r-project.org).
Results
Baseline patient characteristics
The US and Canadian cohorts included 477 and 122 patients, respectively. Table 1 displays baseline demographics, extrapulmonary manifestations, treatments, neighbourhood-level disadvantage, follow-up duration and censoring outcomes (broken down by quartile in supplementary table E1). Details regarding baseline immunosuppressant treatments are shown in supplementary table E2 and state or province of residence in supplementary table E3. In the US cohort, patients had a median follow-up duration of 8.3 (interquartile range (IQR) 4.6 to 12.3) years, with death in 51 patients (11%) and lung transplantation in 15 (3%). In the Canadian cohort, patients had a median follow-up duration of 4.1 (IQR 2.6 to 7.4) years, with death in four patients (3%) and lung transplantation in none. Non-White race was reported by 26% of the US cohort and 8% of the Canadian cohort. At the time of initial ILD clinic visit, extrapulmonary manifestations were present in 50% and 41% of US and Canadian patients, respectively, and immunosuppressant treatment had previously been received by 47% and 59%, respectively.
Patient demographics by US or Canadian cohort
In the US cohort, individuals of Black race were over-represented in the lowest quartile of ADI (quartile 4, Q4), making up 49% of patients in Q4 and 17% of patients in quartile 1 (Q1) (supplementary table E1). Similar trends were not noted in the Canadian cohort, but this was limited by the presence of only 10 non-White patients. Post hoc analyses adjusted for age at diagnosis, sex and smoking in US patients with sarcoidosis indicated that individuals with self-reported Black or dichotomised non-White race had higher ADI scores (Black β = 13.1, 95% CI 8.3 to 17.9, p<0.001; non-White β = 12.2, 95% CI 7.6 to 16.8, p<0.001). These data indicate that a patient of Black self-reported race has a 13-point higher neighbourhood-disadvantage score (range 1–100) compared to White patients. In Canadian patients with sarcoidosis, there was no association of self-reported Black or non-White race with CIMD in fully adjusted models (Black β = −0.16, 95% CI −0.81 to 0.49, p=0.63; non-White β = 0.02, 95% CI −0.34 to 0.39, p=0.89).
Association of neighbourhood disadvantage with baseline lung function
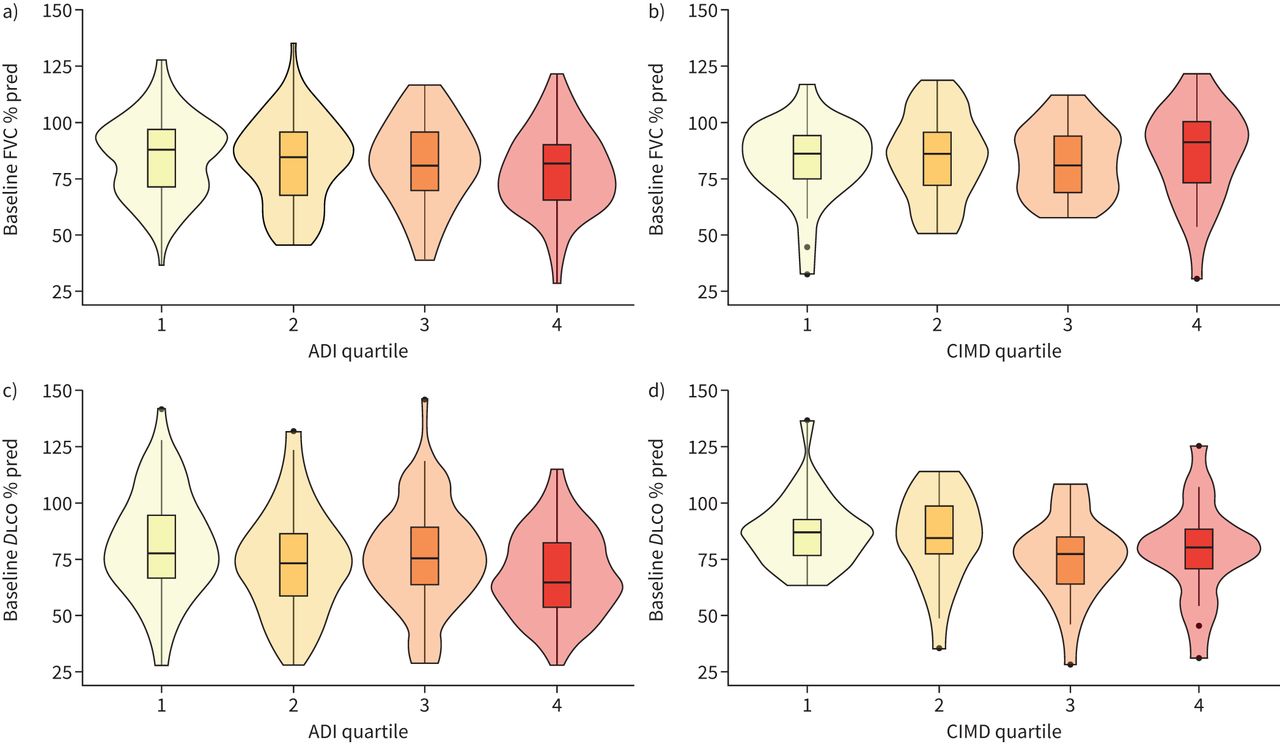
389 (82%) US and 102 (84%) Canadian patients had baseline FVC measurements, with supplementary table E4 demonstrating the characteristics of patients with and without baseline FVCs. Higher continuous ADI was associated with lower baseline % pred FVC in unadjusted and partially adjusted models in the US cohort (unadjusted β = −0.13, 95% CI −0.21 to −0.05, p=0.002; partially adjusted β = −0.14, 95% CI −0.22 to −0.05, p=0.001) (supplementary table E5), but this finding was not preserved in fully adjusted models (table 2). The unadjusted analysis indicates that for each 10-point increase in ADI, the baseline FVC decreased by 1.3%. Quartiled analysis demonstrated association between quartile 4 (Q4) of ADI and lower baseline FVC in unadjusted and partially adjusted, but not fully adjusted analyses (figure 1a). In the Canadian cohort, there was no association of continuous or quartiled CIMD with baseline FVC (table 2, supplementary table E5, figure 1b).
Fully adjusted linear regression models evaluating the association between ADI or CIMD and baseline FVC or DLCO

Baseline lung function by neighbourhood disadvantage quartile. Baseline % pred FVC by neighbourhood disadvantage quartile in a) US and b) Canadian cohort, and DLCO by neighbourhood disadvantage quartile in c) US and d) Canadian cohort. ADI: area deprivation index; CIMD: Canadian Index of Multiple Deprivation; DLCO: diffusing capacity of the lung for carbon monoxide; FVC: forced vital capacity.
375 (79%) US and 87 (71%) Canadian patients had baseline DLCO measurements. Higher continuous ADI and Q4 of ADI were both associated with lower baseline % pred DLCO in all models in the US cohort (fully adjusted continuous β = −0.10, 95% CI −0.19 to −0.0004, p=0.049; fully adjusted Q4 β = −6.80, 95% CI −13.16 to −0.44, p=0.04) (table 2, supplementary table E5, figure 1c). In all models in the Canadian cohort, higher continuous or quartiled CIMD had the same direction of effect on baseline DLCO (figure 1d).
Association of neighbourhood disadvantage with longitudinal lung function
The median change in FVC % pred per year in the US cohort was 0.45 (IQR −0.86 to 1.41, n=389) and in the Canadian cohort was 0.04 (IQR −1.36 to 1.11, n=102). A negative rate of change in FVC was seen in 132 (34%) US and 41 (40%) Canadian patients, with only 29 (7%) and 3 (3%) patients experiencing >5% predicted decline in FVC per year over the study period. In the US cohort, higher continuous ADI and Q4 of ADI had negative interactions with time in all unadjusted and adjusted models of FVC decline, indicating that greater disadvantage is associated with more rapid FVC decline (fully adjusted continuous ADI*time β = −0.005, 95% CI −0.009 to −0.0003, p=0.04; fully adjusted Q4*time β = −0.36, 95% CI −0.63 to −0.11, p=0.007) (table 3, supplementary table E6, figure 2a). This indicates that compared to quartile 1 (Q1), patients living in Q4 of ADI experience an additional 0.36% decline in FVC per year. Similarly, higher continuous and quartiled CIMD both had significant negative interactions with time (fully adjusted continuous ADI*time β = −0.47, 95% CI −0.84 to −0.10, p=0.01; fully adjusted Q4*time β = −0.80, 95% CI −1.37 to −0.24, p=0.006), indicating that patients living in neighbourhoods with greater disadvantage in Canada also experience more rapid declines in FVC (table 3, supplementary table E6, figure 2b).
Fully adjusted linear mixed effects models with random intercept evaluating the association between ADI or CIMD and rate of change in FVC or DLCO

{kind=link}
{kind=link}
Rate of lung function decline by neighbourhood disadvantage quartile. Trajectory of FVC for all patients with sarcoidosis and superimposed line of best fit (loess method) by neighbourhood disadvantage quartile in a) US and b) Canadian cohort, and trajectory of DLCO by neighbourhood disadvantage quartile in c) US and d) Canadian cohort. DLCO: diffusing capacity of the lung for carbon monoxide; FVC: forced vital capacity; PFT: pulmonary function test.
The median change in DLCO % pred per year in the US cohort was −0.22 (IQR −1.71 to 1.12, n=375) and in the Canadian cohort was −0.72 (IQR −2.00 to 1.24, n=85). A negative rate of change in DLCO was seen in 165 (44%) US and 38 (45%) Canadian patients, with only 35 (9%) and 9 (11%) patients experiencing >5% predicted decline in DLCO per year over the study period. In the US cohort, higher ADI was associated with a significant negative interaction with time in all unadjusted and adjusted models of DLCO decline (fully adjusted β = −0.008, 95% CI −0.01 to −0.003, p=0.002) (table 3, supplementary table E6). Quartiled analyses in the US cohort indicate that living in any quartile above Q1 is associated with accelerated DLCO decline (fully adjusted Q4*time β = −0.54, 95% CI −0.87 to −0.21, p=0.001) (figure 2c). This fully adjusted β indicates that compared to Q1, patients living in Q4 of ADI experience an additional 0.54% decline in DLCO per year. In unadjusted and partially adjusted models in the Canadian cohort, higher continuous CIMD had a significant negative interaction with time. The fully adjusted and quartiled models did not demonstrate a significant effect, but the direction of effect was consistent with the US cohort (table 3, supplementary table E6, figure 2d).
Association of neighbourhood disadvantage with survival
Secondary survival analyses demonstrated no association of higher continuous or quartiled ADI with mortality (supplementary table E8), and due to too few events, this outcome was not evaluated in the Canadian cohort. Although not the pre-specified variable of interest in this study, it was noted in fully adjusted models that individuals of non-White race had significantly lower hazard ratio (HR) for lung transplant (HR = 0.15, 95% CI 0.03–0.74, p=0.02), but no difference in HR for death (HR = 0.79, 95% CI 0.35–1.81, p=0.58).
Discussion
This study, which is the first evaluation of neighbourhood-level disadvantage as a social determinant of health in sarcoidosis, demonstrated that patients who live in neighbourhoods with greater disadvantage experience more severe pulmonary disease at presentation (as indicated by lower baseline FVC and DLCO) and more rapid lung function decline. Furthermore, we demonstrated that US Black or non-White patients more frequently lived in disadvantaged neighbourhoods, highlighting how neighbourhood-level inequities may intersect with racial disparities to contribute to adverse outcomes in this population. This work highlights the need for further studies to investigate the interactions between neighbourhood-level factors and individual barriers to care, delayed specialist referral, and accelerated disease progression in patients with sarcoidosis and other chronic diseases.
Living in neighbourhoods with high disadvantage places additional burdens on patients with chronic diseases, beyond individual factors such as SES or race [20, 31, 32]. Data on neighbourhood-level disadvantage are also often more readily available for clinical cohorts of patients, which often fail to capture individual SES data. Factors such as dilapidated housing, lack of residential green space, public safety hazards, lack of access to healthcare, medications or groceries, and limited nearby job opportunities all contribute compounding insults to individuals living in impoverished areas. US individuals living in more disadvantaged neighbourhoods also experience increased air pollution-attributable mortality, related in part to closer proximity to major roadways and industrial pollution [33]. Although the impact of air pollution on patients with sarcoidosis has not been thoroughly explored, it is plausible that harmful environmental exposures in disadvantaged neighbourhoods may contribute to adverse outcomes in patients with sarcoidosis. Furthermore, racial disparities in residential environment or occupational exposures may increase the risk of sarcoidosis development and progression [12, 33]. Neighbourhood-related factors may also limit access to specialist care, which has been identified as a critical treatment issue for patients with sarcoidosis [34]. Such delays are likely to contribute to patients presenting with worse baseline pulmonary function. Identification of neighbourhood-level disparities in chronic disease populations provides opportunities for policy-based interventions to mitigate environmental injustice, housing, transportation, employment and educational inequities that may contribute to these adverse outcomes.
Our study demonstrated that patients living in neighbourhoods with higher disadvantage experience worse baseline DLCO and more rapid decline in FVC and DLCO. Further research is needed to define what reflects a clinically significant decline in FVC or DLCO in this population; however given the small rates of change in pulmonary function over the course of patient follow-up found in this study, these statistically significant differences in lung function decline may also reflect clinically meaningful differences. For example, patients living in the highest quartile of disadvantage (Q4) experienced ∼2.5-times more DLCO decline than the median decline in the US cohort (−0.54%/year versus −0.22%/year). It remains unclear whether this accelerated pulmonary progression translates to increased healthcare utilisation or pulmonary-specific mortality, but established associations of progressive pulmonary sarcoidosis with high morbidity and increased mortality support that this may be the case [35]. Careful evaluation of patient socioeconomic status and neighbourhood-level resources may support clinician identification of patients at increased risk of progressive pulmonary sarcoidosis. Patients with increased neighbourhood deprivation are also at greater risk for development of sarcoidosis, as demonstrated by a Swedish population-based study [36]. Systemic interventions to mitigate intersectional racial and socioeconomic disparities may be of particular benefit to patients with sarcoidosis, given the robust body of evidence linking these factors to adverse clinical outcomes in this population [6–9, 13, 14, 16].
Although race was not the primary variable of interest in our study, this research builds upon the previous evidence base identifying substantial racial and ethnic disparities in patients with sarcoidosis, especially in the US [6–9]. Patients of Black or the broader “non-White” self-reported race had higher neighbourhood disadvantage scores, which may translate to increased risk of disadvantage-associated morbidity in the form of reduced lung function. Furthermore, US patients of non-White race had substantially lower likelihood of receiving a lung transplant, highlighting potential access to care issues. While all Canadian patients in this study had universal healthcare coverage, we were unable to capture insurance status for our US cohort. Previous research has demonstrated that individual SES, lack of insurance coverage and African American race contribute to more severe disease at presentation [6, 11]. Future work should explore the interactions between these factors and neighbourhood disadvantage, to help disentangle the intersectional relationships between these factors, especially given our increasing understanding of how implicit biases in healthcare can lead to compounding disparities in racialised individuals [10]. Efforts to mitigate the harmful impacts of neighbourhood disadvantage must also co-address racial inequities that contribute to harm in this vulnerable patient population.
This study was limited by a lack of access to several variables that may impact disease severity and progression in patients with sarcoidosis, including occupational exposure history, individual SES, insurance status (for US patients only) and non-sarcoidosis-related comorbidities. While we did capture data on baseline treatments and extrapulmonary manifestations, we were unable to access reliable medication and manifestation details on patients throughout the course of their registry enrolment, and as such we were unable to control for these factors in our analyses. Included patients all had specialist-confirmed diagnoses of sarcoidosis, but we were unable to access biopsy data on all patients to externally validate these diagnoses. Racial diversity was limited, especially in our Canadian cohort, which limits our ability to draw further conclusions about the intersectional impacts of neighbourhood disadvantage and racial disparities. Lastly, the ADI and CIMD are different scores for neighbourhood disadvantage that may capture slightly different aspects of material and social disadvantage between the two countries studied. As such, quartiled analyses aided in the comparability of these metrics between our two cohorts.
Conclusions
This study provides a novel evaluation of the impact of neighbourhood-level disadvantage from two cohorts of patients with sarcoidosis from the US and Canada, demonstrating that greater disadvantage is associated with worse baseline lung function and more rapid lung function decline. High disadvantage was most common in individuals of non-White race, indicating how racial disparities can add to socioeconomic disparities to lead to worse outcomes in minoritised individuals with sarcoidosis. Further work is needed to understand how policies aimed at reducing neighbourhood-level inequities may mitigate these outcome disparities in patients with sarcoidosis and other chronic diseases.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00357-2022.SUPPLEMENT
Acknowledgements
We would like to thank the patients with sarcoidosis from the Dorothy P. and Richard P. Simmons Center for Interstitial Lung Disease and each of the CARE-PF registry sites for their time and commitment to clinical research. We would also like to thank all other contributors to CARE-PF who are not listed as authors on this manuscript, including Alyson W. Wong (Division of Respiratory Medicine, University of British Columbia), Mohsen Sadatsafavi (Division of Respiratory Medicine, University of British Columbia), Julie Morisset (Département Pneumonologie, Centre Hospitalier de l'Université de Montréal (CHUM)), Shane Shapera (Division of Respirology, University of Toronto), Charlene D. Fell (Division of Respiratory Medicine, University of Calgary), Gerard Cox (Department of Medicine, Firestone Institute for Respiratory Health, McMaster University), Teresa To (Divisions of Epidemiology and Biostatistics, Dalla Lana School of Public Health, University of Toronto), Andrea S. Gershon (Division of Respirology, University of Toronto), Nathan Hambly (Department of Medicine, Firestone Institute for Respiratory Health, McMaster University), Andrew J. Halayko (Department of Physiology and Pathophysiology, University of Manitoba), and Pearce G. Wilcox (Division of Respiratory Medicine, University of British Columbia).
Footnotes
Provenance: Submitted article, peer reviewed.
Author contributions: All authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors. G.C. Goobie, K.O. Lindell and S.M. Nouraie were responsible for study development, analysis and initial manuscript production. E. Schikowski provided code and raw data for analysis of outcomes in the US cohort. S. Keil performed patient chart reviews for the US cohort. C.J. Ryerson, K.A. Johannson, K.F. Gibson, Y. Zhang, D.J. Kass, N. Khalil, V. Marcoux, D. Assayag, H. Manganas, J.H. Fisher and M.R.J. Kolb contributed to the development of the clinical cohorts, performed chart reviews for the Canadian cohorts, and provided critical commentary and review of the manuscript. S.M. Nouraie provided insight on biostatistical and epidemiological methods. All authors had full access to the data analysed in this study and accept responsibility for publication.
Conflict of interest: G.C. Goobie receives research funding and support through the Pulmonary Fibrosis Foundation Scholars Award Program and the University of British Columbia Clinician Investigator Program. C.J. Ryerson, D. Assayag and M.R.J. Kolb report personal fees and grants from Boehringer Ingelheim and Hoffman La Roche outside the submitted work. K.A. Johannson reports personal fees, nonfinancial support and other support from Boehringer Ingelheim and the Three Lakes Foundation, personal fees from Hoffman-La Roche Ltd, and grants from the University Hospital Foundation, the University of Calgary Cumming School of Medicine, and the Pulmonary Fibrosis Society of Calgary. V. Marcoux reports grants and personal fees from Boehringer Ingelheim Canada, Hoffman La-Roche Ltd and AstraZeneca, and grants from the University of Saskatchewan and the Royal University Hospital Foundation. M.R.J. Kolb also reports personal fees and grants from GSK, Gilead, Actelion, Respivert, Genoa, Alkermes, Pharmaxis, Prometric, Indalo and Third Pole. H. Manganas reports grants from Hoffman-La Roche Ltd, Galapagos and BMS, and personal fees and research grants from Boehringer Ingelheim. D. Assayag also reports personal fees and grants from Novartis. J.H. Fisher reports grants from the Canadian Pulmonary Fibrosis Foundation, and personal fees from Boehringer Ingelheim and AstraZeneca, outside of the submitted work. D.J. Kass is supported in part by AR060780, HL133232, UL1 TR001857 and AR076024 (NIH grants), Boehringer Ingelheim grants, and receives collaborative research funding from Regeneron Pharmaceuticals, outside of the submitted work. Y. Zhang is supported in part by AR076024 (NIH grant). S. Keil, E. Schikowski, N. Khalil, X. Chen, K.F. Gibson and K.O. Lindell report no competing interests. S.M. Nouraie receives grant support from Boehringer Ingelheim USA.
Support statement: This was an independent, investigator-initiated study supported by Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). BIPI had no role in the design, analysis or interpretation of the results in this study; BIPI was given the opportunity to review the manuscript for medical and scientific accuracy as it relates to BIPI substances, as well as intellectual property considerations. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received July 18, 2022.
- Accepted August 18, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










