





Abstract
Background Organising pneumonia (OP) has variable clinical and radiographic presentations and unstandardised treatments. Most patients with OP have favourable outcomes, but some develop respiratory insufficiency, experience recurrence or die. In this study we investigated the impact of computed tomographic (CT) patterns and extent of OP on the diagnostic and therapeutic management that patients received, and that on the therapeutic response and prognosis (particularly the risk of respiratory insufficiency and death).
Methods We retrospectively studied 156 patients with OP followed at our hospital between 2010 and 2021. The diagnosis was confirmed histologically and verified by multidisciplinary specialists. We performed Firth's logistic regression to determine the relationship between CT features and aetiologies, management and outcomes including the risk of severe disease (defined as the need for supplemental oxygen or mechanical ventilation). We conducted Kaplan–Meier analyses to assess survival differences.
Results Patients exhibiting multilobe involvement or mixed patterns, or both, were more likely to have secondary OP and receive immunosuppressants. Higher proportions of these patients experienced recurrence. Compared to patients with single-lobe involvement and single-pattern, they also had an enhanced risk of severe disease (the adjusted odds ratio for patients who simultaneously had multilobe involvement and mixed patterns was 27.64; 95% confidence interval 8.25–127.44). Besides, these patients had decreased survival probabilities.
Conclusion Different CT features of OP impact patients’ management and prognosis. When treating patients with OP exhibiting multilobe involvement or mixed patterns, or both, it is important to identify the possible causative aetiology and follow closely for adverse outcomes.
Abstract
Patients with organising pneumonia whose CT images exhibit multilobe involvement and mixed patterns have an increased risk of adverse outcomes https://bit.ly/3tjhYS8
Introduction
Organising pneumonia (OP) is a rare type of interstitial lung disease (ILD) [1–3]. It is either cryptogenic or secondary, depending on whether a causative aetiology is identified [2–5]. Common aetiologies of secondary OP include autoimmune disorder, drug reactions, inhalational injury and post-transplantation [1, 3, 5]. The histology of OP has been well described, and that helps to resolve diagnostic uncertainty. Typical histological features of OP include Masson bodies (type III collagen-rich granulation plugs) filling in the distal airspaces in a background of well-preserved alveolar architecture accompanied by a mild-to-moderate degree of interstitial infiltrate by chronic inflammatory cells [2–4, 6, 7]. Historically OP was used interchangeably with another term “BOOP” (bronchiolitis obliterans organising pneumonia), but these two terms now specify distinct entities based on histological, radiographic and spirometric differences [1–3]. The clinical presentations of OP, on the other hand, are quite nonspecific and variable. Some patients are asymptomatic or complain only of non-productive cough with or without flu-like illness, while others have manifestations that are indistinguishable from acute pyogenic pneumonia [3–8]. Still others may develop severe disease, progressively leading to hypoxaemia, respiratory insufficiency or death [3, 9–12]. Similarly, although corticosteroids are commonly used, the treatment for OP has not been standardised, and patients may exhibit variable therapeutic responses [1–3, 13–15].
Computed tomographic (CT) features of OP also vary. Alveolar consolidation is the archetypal pattern, but other CT patterns have been subsequently reported. Different patterns of OP may appear alone or in combination, involving the lung parenchyma focally or extensively [1–3, 13–18]. Radiographic differential diagnosis includes infectious pneumonia or granuloma, malignancy, vasculitis and some forms of ILDs with an alveolar component (particularly acute interstitial pneumonia, nonspecific interstitial pneumonia, eosinophilic pneumonia, hypersensitivity pneumonia and pulmonary alveolar proteinosis) [1–4]. CT findings, however, can rapidly and noninvasively provide useful information for the initial diagnosis, assessment and subsequent follow-up of OP. Previous researchers have found that certain imaging patterns, and the extent of consolidation, on CT images are associated with residual disease and recurrence of OP [14, 15, 19, 20]. Nevertheless, it remains to be determined whether patients exhibiting different CT features would undergo different management and have distinct risk of other clinically important outcomes. Therefore, in this study, we aimed to investigate the impact of CT imaging patterns and extent of OP on the modalities of diagnostic and therapeutic management that patients received, and that on the therapeutic response and prognosis, particularly the risk of respiratory insufficiency and death.
Material and methods
Study design and population
We conducted this single-centre retrospective study, analysing the clinical and CT presentations of adult patients (age≥20 years) with OP longitudinally followed at National Cheng Kung University Hospital (NCKUH, a tertiary medical centre in southern Taiwan) between 1 January 2010 and 31 December 2021. The study protocol has been approved by the Institutional Review Board of NCKUH (B-ER-111-038). The clinical and radiographic manifestations of OP are nonspecific. Therefore, to ensure diagnostic accuracy that was essential for all subsequent analysis, we required that all candidates for study inclusion must have previously undergone lung biopsy and histological study to exclude masquerading conditions (supplementary document 1).
Review of the diagnosis and histology
For each potential candidate, the de-identified clinical and laboratory data, histological slides and reports, serial CT images and chest radiographs, and records of treatments and outcomes were carefully reviewed. The diagnosis of OP (originally made by the treating physicians) was verified jointly by the authors consisting of three pulmonologists, a pulmonary radiologist, two pathologists, a thoracic surgeon and a clinical biochemist (supplementary document 1). Consensus was reached by direct discussion. To be considered as having definite OP (either cryptogenic or secondary), a candidate must have compatible symptomology and CT images [1–4], typical histological features [1–3, 6, 7], and the absence of clinical or histological findings (initially or subsequently) suggesting alternative diagnoses (particularly evidence of ongoing infection, bronchiole-centred or bronchiole-obliterative pathology, granulomas, vasculitis, neoplasm, alveolar haemorrhage or proteinosis, and dense infiltration of neutrophils, monocytes–macrophages or eosinophils) [3].
Acquisition of CT images and the classification of CT features
Thoracic CT was acquired at NCKUH during the study period by using scanners from two different manufacturers (Siemens Healthineers, Erlangen, Germany, and General Electric Healthcare, Chicago, IL, USA). The patient's entire lung was scanned in the supine caudocranial direction with suspended full inspiration. The scanning parameters were 100 or 120 kVp, 1- or 0.6-mm collimation and a pitch of 1. Volumetric CT images at 1.0- to 1.5-mm slice thickness were reconstructed into contiguous axial images at 2.0-mm and 5.0-mm slice thickness and 5-mm intervals. High-spatial-frequency reconstruction images were reconstructed at 1 to 1.25 mm of slice thickness and 10-mm intervals. Contrast medium was administered based on clinical indications.
For each patient, the last CT scan that was nearest in time before the histological diagnosis of OP was selected as the baseline. CT images were reviewed and classified independently by a pulmonary radiologist and two pulmonologists unaware of patients’ aetiologies and outcomes, whereby a final consensus was reached by direct discussion. Radiopacity of OP was classified as alveolar consolidation, ground-glass opacity (GGO), bronchocentric opacity, nodular, mass-like, band-like, reticulo-infiltrative, crazy paving or reverse halo sign, according to previously published descriptions [1–3, 16–18, 21, 22]. Patients whose images exhibited only one of these nine patterns were considered as having “single-pattern”, whereas those exhibiting multiple patterns simultaneously were considered as having “mixed-pattern”. Patients were also classified according to the extent of involvement by OP as “single-lobe” or “multilobe”. Based on the combined assessment of patterns and extent, we further stratified the patients into three subgroups: Group 1 included patients exhibiting single-pattern and single-lobe involvement, Groups 2 single-lobe and mixed-pattern or multilobe and single-pattern, and Group 3 multilobe and mixed-pattern.
Definition of outcomes
Outcomes of all included patients were determined jointly by the authors (supplementary document 1). Briefly, “improvement” indicates the radiographic resolution of OP by >50% (with or without decrement in radiodensity) during follow-ups without re-emergence, plus symptomatic alleviation with or without de-escalation in relevant pharmacological (for example, decrement in the number and dosage of immunosuppressive and/or symptom-relieving agents) and non-pharmacological management (for example, decrement or discontinuation in oxygen supplement or mechanical ventilatory support). “Persistent disease” indicates no subsequent radiographic change or a diminishment of <50%, with the associated persistence (or limited change) in clinical symptoms and management. “Recurrence” refers to the radiographic re-emergence or enlargement of pneumonic lesions following an initial “improvement” with the associated escalation in symptoms and management, but without any alternative explanation. The radiographic opacities of OP may fluctuate and migrate with time. Depending on the timing and extent of new migratory opacities in relation to serial changes of the initial lesions and symptoms, patients can be classified as having “persistent disease” or “recurrence” based on the above definitions. “Death” specifies only those mortality events that were causally OP-related. Patients were considered to have the “need of supplemental oxygen” if they had ever breathed supplemental oxygen via any mode to correct hypoxaemia during the follow-up; by this definition elective peri-biopsy oxygen supplement was excluded. “Use of mechanical ventilation” refers specifically to the application of either noninvasive or invasive positive-pressure mechanical ventilation to treat OP-related respiratory failure, but excluding mechanical ventilation during general anaesthesia for surgical biopsy. Changes in pulmonary function tests were not included as essential criteria for the determination of outcomes because only 27 (17%) patients in our cohort had a follow-up pulmonary spirometry (at the discretion of the treating physicians). However, for those patients having follow-up tests, serial changes in forced vital capacity (FVC) were calculated and used as supporting data for outcome assignment.
Statistical analysis
Categorical data are presented as counts and percentages, and continuous data are presented as mean±SD if normally distributed, or as medians and interquartile ranges (IQR) if otherwise. No imputation was made for missing data. Variables were analysed for between-group non-random differences using the Mann–Whitney U-test or Fischer's exact test, whichever was more appropriate. Fleiss’ kappa values were calculated to assess the initial (before the final consensus) interobserver agreement among the three independent reviewers of CT features. Univariate and multivariable Firth's logistic regression models were constructed to analyse the relationship between CT features and outcomes. For multivariable analyses, we incorporated sex, age, body heights and weights, smoking status, Charlson comorbidity indices and aetiology as covariables; no multicollinearity was found among these variables. Survival difference was assessed by Kaplan–Meier methods. Sensitivity analysis was performed to determine the potential effect from unidentified confounders. A p-value <0.05 was considered to indicate statistical significance, and all tests were two-tailed. Statistical analysis was performed using the statistical packages SPSS (Version 26; SPSS Inc., Chicago, IL, USA) and R (Version 3.6.3). Graphs were plotted using MedCalc (Version 20.109; MedCalc Software Ltd., Ostend, Belgium).
Results
Patient characteristics, treatments and outcomes
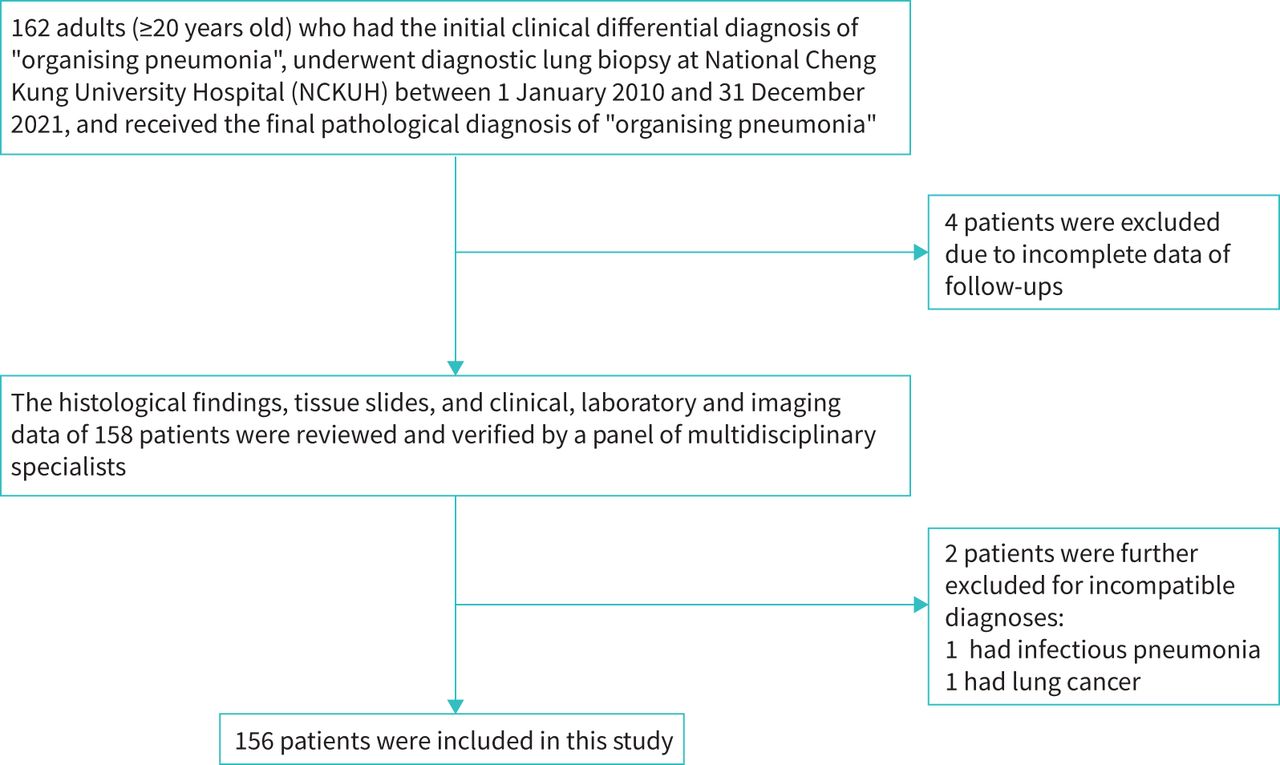
In total 156 patients were included in this study (figure 1); table 1 displays their characteristics and outcomes. Overall, the cohort was relatively male-predominant, with a median age of 61.5 (IQR 54.4–71.1) years. More than two-thirds of the patients never smoked. 91 (58%) patients underwent video-assisted thoracoscopic biopsy, 15 (10%) received transbronchial forceps biopsy, while 49 (31%) and one (1%) received percutaneous needle biopsy via CT guidance and sonography guidance, respectively. Regarding aetiology, 130 (83%) patients were classified as having cryptogenic OP. Of those 26 (17%) with secondary OP, 14 were connective tissue diseases (CTD)-related, 10 were drug-related (most frequently amiodarone) and two were post-transplantation (of peripheral-blood stem cells). Patients were followed for a median of 120.6 (IQR 31.1–269.4) weeks. 93 (60%) patients received non-pharmacological treatments, either close observation or resection (as during the initial biopsy). The remaining 63 (40%) received immunosuppressive therapies that involved corticosteroid in most cases. During the follow-ups, 41 (26%) patients developed hypoxaemia requiring supplemental oxygen, of whom 17 (11%) deteriorated to respiratory failure mandating mechanical ventilation, while the others were successfully weaned off supplemental oxygen. All patients had at least one follow-up radiographic study for comparison, wherein 101 (65%) had at least one follow-up CT scan. The median duration of radiographic follow-up was 27.5 (IQR 14.2–88.0) weeks. Overall, 129 (82%) patients exhibited improvement of the OP, 11 (7%) had persistent disease, five (3%) experienced recurrence and 11 (8%) died from OP. Follow-up pulmonary spirometry was available in 27 patients, which showed changes that were consistent with the outcome assignment (supplementary table S1).

Flow chart of inclusion and exclusion for this study.
Baseline characteristics, management and outcomes of the study cohort
CT features of the cohort
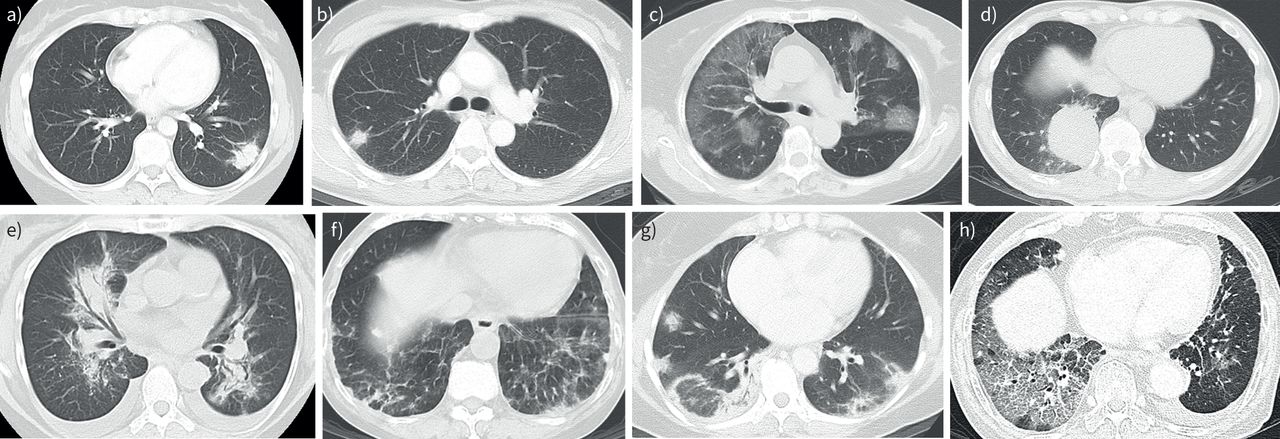
The median time between the baseline CT scan and the histological establishment of the OP diagnosis was 13 (IQR 7–30) days. Table 2 summarises the various CT features of OP observed in our cohort. The initial pre-consensus interobserver agreement was good (supplementary table S2). Comparable proportions of the cohort had single- and multilobe involvement. Regarding imaging patterns, two-thirds of the patients exhibited a single-pattern, while the other third had mixed-patterns. The most common pattern (either as single- or mixed-pattern) in the cohort was alveolar consolidation (45%), which was followed in decreasing frequencies by nodular (34%), GGO (31%), mass-like (14%) and bronchocentric opacity (13%). Less common patterns included reticulo-infiltrative (4%), reverse halo sign (4%) and crazy paving (3%). The band-like pattern was not observed. Examples of the various CT features are presented in figure 2 and supplementary figure S1.
Computed tomographic (CT) features of organising pneumonia

Representative images of the various computed tomographic patterns observed in patients of our study cohort: a) alveolar consolidation; b) nodular; c) multilobar ground-glass opacity (GGO); d) mass-like; e) bronchocentric; f) a combination of GGO and reticulo-infiltrative opacity; g) reverse halo sign in a background of mixed GGO and alveolar consolidation; and h) crazy paving pattern mixed with GGO.
CT features and outcomes
No significant difference was found in methods of biopsy and seasons of diagnosis among patients with different CT features. However, higher proportions of patients with multilobe involvement, and of patients with mixed patterns, had secondary OP and received immunosuppressive therapies. Compared to those with single-lobe and single-pattern OP, higher proportions of patients with multilobe involvement and mixed patterns developed hypoxaemia and respiratory failure. All five patients with recurrence had multilobe involvement and mixed patterns. Of those 11 patients who died, 10 exhibited multilobe and mixed-pattern OP, and one had single-pattern but multilobe involvement (supplementary table S3). When the cohort was stratified into Groups 1 to 3 as described above (supplementary table S4 shows characteristics of the three subgroups), we obtained concordant findings such that with increasing complexity and extent of pneumonic involvement from Group 1 to Group 3, we observed incremental proportions of patients who had secondary OP, received immunosuppressive therapies and developed adverse outcomes (figure 3 and supplementary table S3). Moreover, baseline pulmonary function measurements were available from 86 patients. When we further stratified these patients according to CT features and baseline FVC values using the cut-off levels of 50% and 80% of prediction, similar trends were observed such that Group 3 patients consistently had the highest frequencies of adverse outcome events regardless of what the baseline FVC strata was (supplementary table S5).
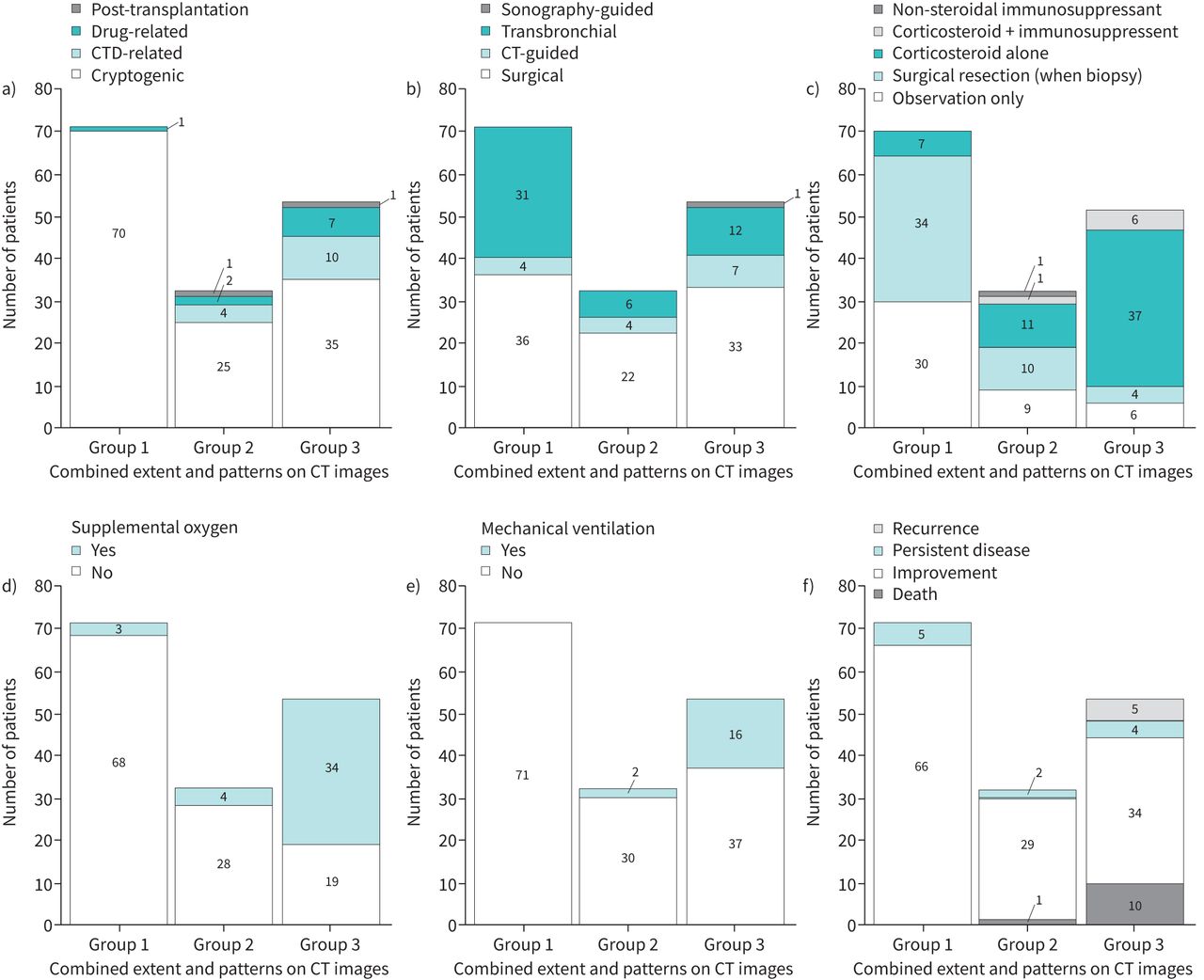
Distribution of frequencies of a) aetiologies, b) methods of tissue sampling, c) treatments, d) need of supplemental oxygen, e) use of mechanical ventilation and f) different outcomes among patients of the three subgroups based on the combined assessment of the extent and patterns of involvement on computed tomography images (Group 1: single-lobe and single-pattern; Group 2: single-lobe and mixed-pattern or multilobe and single-pattern; Group 3: multilobe and mixed-pattern). CT: computed tomography; CTD: connective tissue disease.
Because the frequencies of some adverse outcomes are very low in certain subgroups (figure 3), for subsequent analyses, “need of supplemental oxygen” and “use of mechanical ventilation” were combined into one composite outcome as “severe disease”. Univariate and multivariable Firth's logistic regression analysis showed that “multilobe” and “mixed-pattern”, when analysed separately, were each associated with secondary OP and subsequent immunosuppressive treatments: the adjusted odds ratio (aOR) of secondary OP and the aOR of immunosuppressive treatments were 6.99 (95% confidence interval (CI) 2.35–27.76) and 12.45 (95% CI 5.20–33.70) for “multilobe”, and 6.38 (95% CI 2.51–18.14) and 7.97 (95% CI 3.55–18.94) for “mixed-pattern”, respectively. “Multilobe” and “mixed-pattern” were also each associated with an enhanced risk of severe disease: the aOR was 17.84 (95% CI 5.55–79.66) for “multilobe” and 12.87 (95% CI 5.12–36.50) for “mixed-pattern”. When “multilobe” and “mixed-pattern” were analysed simultaneously within the same model, we obtained similar findings. The analysis was then performed among the three subgroups. Relative to Group 1, patients in Group 2 had significantly increased odds of secondary OP (aOR 11.77; 95% CI 2.36–115.80) and immunosuppressive treatments (aOR 3.39; 95% CI 1.11–10.67), and the odds ratios rose further in Group 3 (aORs were 19.08, 95% CI 4.46–177.80, and 19.58, 95% CI 7.28–59.81, respectively). Moreover, while patients in Group 2 exhibited a trend of increasing odds (aOR 4.24, 95% CI 0.89–22.84), patients in Group 3 had a significantly enhanced risk of severe disease (aOR 27.64, 95% CI 8.25–127.44; supplementary table S6–S8 and figure 4). Results from sensitivity analyses showed that, even in the presence of an unidentified confounder, findings derived from the above analyses remained consistent (supplementary figure S2).
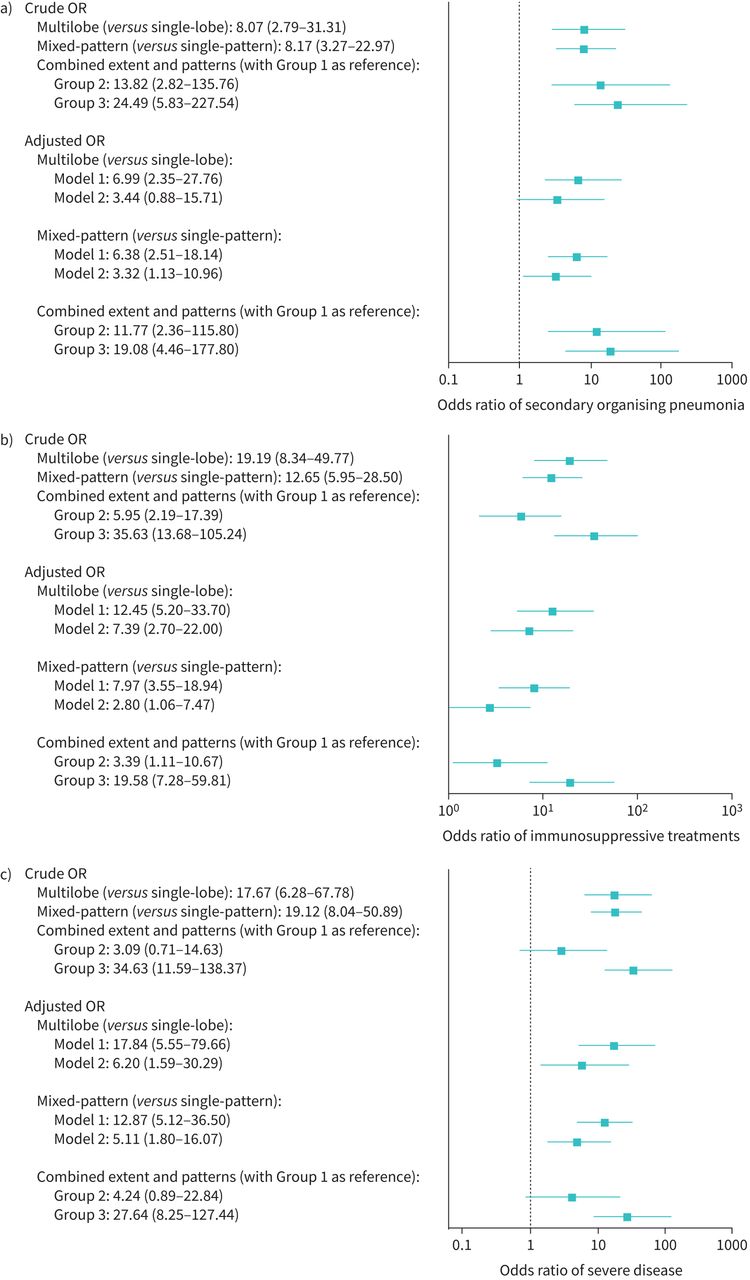
Forest plots showing a) crude and adjusted odds ratios of secondary organising pneumonia b) crude and adjusted odds ratios of immunosuppressive treatments, and c) crude and adjusted odds ratios of severe disease, for patients with different radiographic features. Note: Groups are based on the combined assessment of the extent and patterns of involvement on computed tomographic images: Group 1: single-lobe and single-pattern; Group 2: single-lobe and mixed-pattern or multilobe and single-pattern; Group 3: multilobe and mixed-pattern. OR: odds ratio.
CT features and survival difference
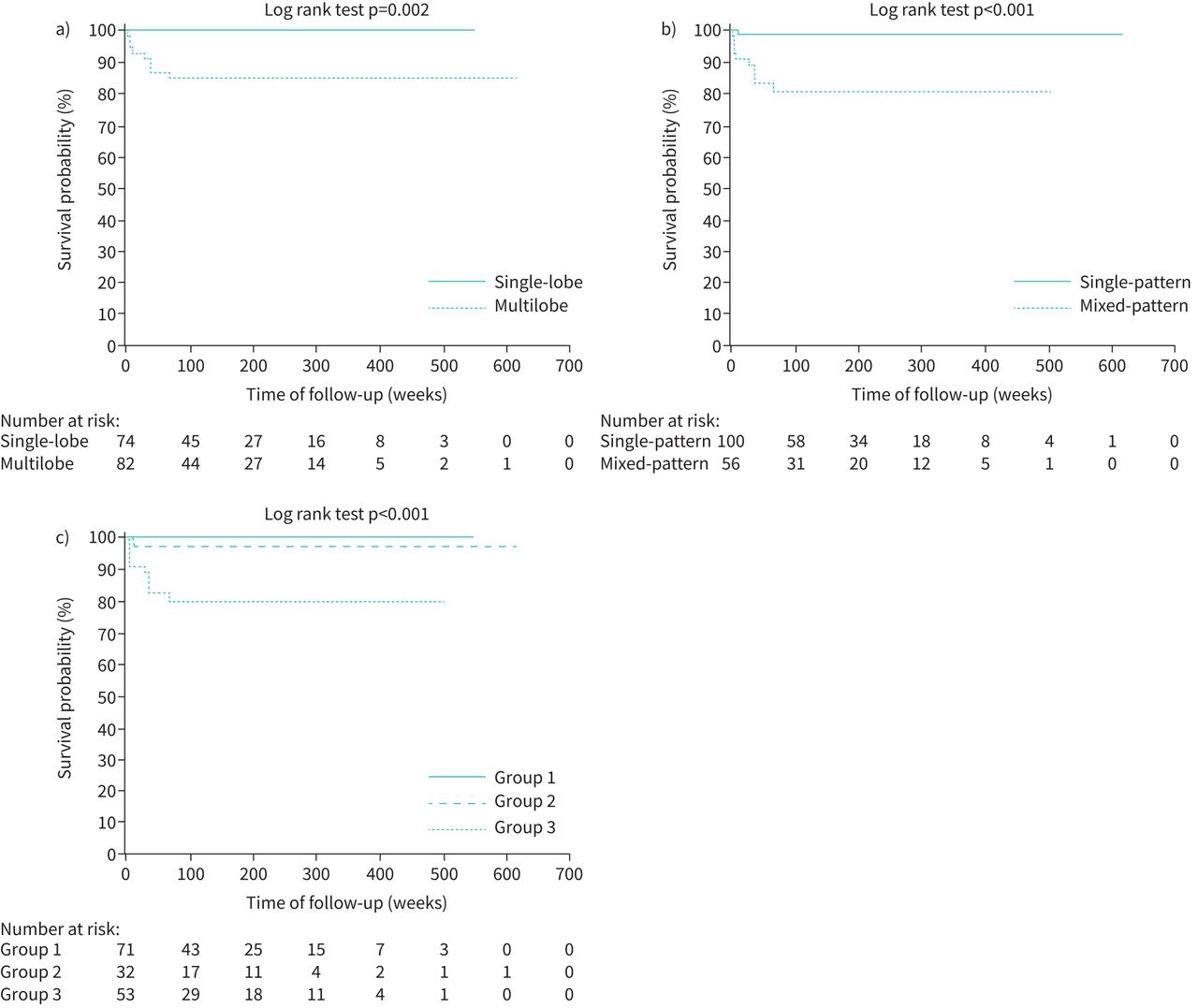
The overall prognosis of OP was good, but Kaplan–Meier analyses detected significant differences in survival probabilities among patients with different CT features. Compared to “single-lobe” and “single-pattern”, patients having multilobe involvement and those exhibiting mixed patterns had decreased survival probabilities. Similarly, the survival probabilities differed among the three subgroups, with Group 3 exhibiting the worst survival (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival analyses a) between “single-lobe” and “multilobe” groups, b) between “single-pattern” and “mixed-pattern” groups and c) among Groups 1, 2 and 3. Note: Groups are based on the combined assessment of the extent and patterns of involvement on computed tomographic images: Group 1: single-lobe and single-pattern; Group 2: single-lobe and mixed-pattern or multilobe and single-pattern; Group 3: multilobe and mixed-pattern.
Discussion
In this study, we found that CT features of OP had an impact on important clinical aspects. Specifically, patients whose OP exhibited multilobe involvement, or mixed CT patterns, or both, were more likely to have an identifiable causative aetiology and receive immunosuppressive therapies. These patients also had an enhanced risk of severe disease and lower probabilities of survival. Higher proportions of these patients also experienced recurrence. Pathophysiologically our findings appear reasonable. Aetiologies of secondary OP are generally systemic processes and would therefore affect the lungs extensively. This explains the higher odds of secondary OP in patients with multi-focal and mixed-pattern lesions. Moreover, increasing extent and complexity of the parenchymal involvement by OP is likely to increasingly impair the pulmonary function (this was supported by the significant decrement in FVC and total lung capacity from Group 1 to Group 3; supplementary table S4). This subsequently leads to an enhanced disease severity and thereby the escalation of therapeutic actions. Furthermore, CT features provide prognostic prediction beyond the revelation of structural and physiological impairment.
Previous researchers have investigated potential predictors of treatment response and recurrence of OP [14, 15, 19, 20, 23–26]. The study by Barroso et al. [19] found that higher proportions of patients with recurrence had multi-focal opacities on chest radiographs. Saito et al. [20] also identified certain CT features as possible predictors of recurrence in univariate analyses. By analysing serial CT images in a cohort of Korean patient with cryptogenic OP, Chung et al. [14] reported that the extent of consolidation on CT images is associated with residual disease. Recently, Cho et al. [15] also found that the presence of bronchiectasis and >10% of consolidation on CT images were associated with recurrence. Our study is consistent with these previous works in demonstrating a significantly higher frequency of recurrence among patients with multilobe (more extensive) OP. On the other hand, we identified “mixed-pattern” as still another feature associated with recurrence. In addition to recurrence, we further addressed the risk prediction of other clinically important outcomes. The methods by which we stratified CT features and grouped the patients are straightforward, avoiding the complexity of radiopacity quantification and allowing for convenient application in real-world clinical settings.
The heterogeneity between cryptogenic and secondary OP (particularly CTD-related) might be a confounding factor [5, 15, 27, 28]. Cho et al. [15] reported that CTD-related OP was also associated with a higher risk of residual disease and recurrence. In our cohort, patients with secondary OP indeed had a lower median body weight, lower spirometric volumes, a higher median Charlson comorbidity index and higher frequencies of adverse outcomes (supplementary table 9). However, when analyses were performed solely in patients with cryptogenic OP, we obtained consistent findings (supplementary table S10 and supplementary figure S3a). Lower survival probabilities were also observed in patients with cryptogenic OP exhibiting multilobe involvement and mixed patterns (supplementary figure S3b–d). Therefore, the findings of our study were not biased towards the contribution from patients with secondary OP.
There are possible limitations to our study. We included only patients whose OP had been confirmed histologically, though OP can also be diagnosed clinically. Nevertheless, the clinical and radiographic characteristics of OP are nonspecific and even indistinguishable from bacterial pneumonia and some ILDs. Had we included patients based on clinical diagnoses only, we might have included other mimicking conditions than true OP. We might have also missed out those patients exhibiting unusual radiographic features (such as mass-like and reticulo-infiltrative patterns) whereby histology would be necessary for the definite diagnosis. Histological confirmation, in our opinion, was important to ensure diagnostic accuracy and the validity of our conclusions. Besides, the retrospective design was inherently susceptible to potentially unidentified confounders, despite that great effort has been made for the comprehensiveness of data collection and statistical control of confounders, and that the findings were supported by results of sensitivity analyses. A prospective cohort is preferable, but patient recruitment would be practically difficult due to the rarity of OP. Thirdly, not all patients had follow-up CT scans; for those 55 (35%) patients without subsequent CT scans, assessment of radiographic changes in outcome determination was performed using serial plain chest radiographs. In our opinion, this should not have compromised the accuracy of our assignment of patient outcomes. The definitions for the radiographic domain of different outcomes were also applicable to the assessment using plain radiographs. In addition to the radiographic domain, when determining outcomes we also considered the clinical domain, incorporating changes in patients’ symptoms, treatments, demand of supplemental oxygen and need of mechanical ventilation over time. Furthermore, we included only patients from a tertiary medical centre in Taiwan. We also did not include cases of post-COVID-19 OP, because it was not until late 2021 that SARS-CoV-2 became pandemic in Taiwan [29, 30]. Future studies involving patients with OP of more diverse ethnicity and aetiologies would be helpful to broaden the generalisation of our findings.
Conclusions
In this study involving patients with histologically confirmed OP, we found that patterns and extent of OP on CT images had impact on patients’ management and outcomes. Patients with multilobe mixed-pattern CT features were more likely to have secondary OP, receive immunosuppressive treatments and experience a recurrence. These patients also had an enhanced risk of severe disease and a worse survival. Therefore, when treating patients exhibiting these CT imaging features, clinicians need to be vigilant to identify any underlying aetiology, and closely follow for the timely detection and management of clinical deterioration.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00505-2022.SUPPLEMENT
Acknowledgements
We thank all the patients enrolled in this study for their contribution. We are thankful to rheumatologists from the Department of Internal Medicine of National Cheng Kung University Hospital for providing professional consultation and assistance on the diagnosis and verification of connective tissue disease-related organising pneumonia. We are thankful to Wan-Ni Chen, a statistician from the Biostatistics Consulting Center of National Cheng Kung University Hospital, for providing statistical consultation and assistance.
Footnotes
Provenance: Submitted article, peer reviewed.
Ethics approval: The study protocol has been approved by the Institutional Review Board of National Cheng Kung University Hospital (B-ER-111-038).
Availability of data and materials: The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author contributions: T-H. Huang and S-H. Wei contributed equally to this manuscript; T-H. Huang and C-L. Wu contributed to the conception and design; T-H. Huang, S-H. Wei and H-P. Er contributed to the data collection and curation; T-H. Huang, S-H. Wei, H-P. Er, Y-L. Tseng and C-L. Wu contributed to the review of medical records and clinical data; L-T. Huang, T-H. Huang, S-H. Wei and H-P. Er contributed to the review of radiographic images and reports; T-H. Huang, Y-T. Yu, C-T. Lee and Y-L. Tseng contributed to the review of surgical records and histological reports and slides; T-H. Huang, S-H. Wei and C-L. Wu contributed to the statistical analysis; T-H. Huang, S-H. Wei, H-P. Er, L-T. Huang and Y-T. Yu contributed to the drafting of the manuscript; T-H. Huang, S-H. Wei, C-L. Wu and Y-L. Tseng contributed to the critical review of the manuscript.
Conflict of interest: The authors have nothing to disclose.
- Received September 28, 2022.
- Accepted November 1, 2022.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










