





Abstract
Objective The aim of this study was to evaluate biomarkers to predict radiographic pneumonia among children with suspected lower respiratory tract infections (LRTI).
Methods We performed a single-centre prospective cohort study of children 3 months to 18 years evaluated in the emergency department with signs and symptoms of LRTI. We evaluated the incorporation of four biomarkers (white blood cell count, absolute neutrophil count, C-reactive protein (CRP) and procalcitonin), in isolation and in combination, with a previously developed clinical model (which included focal decreased breath sounds, age and fever duration) for an outcome of radiographic pneumonia using multivariable logistic regression. We evaluated the improvement in performance of each model with the concordance (c-) index.
Results Of 580 included children, 213 (36.7%) had radiographic pneumonia. In multivariable analysis, all biomarkers were statistically associated with radiographic pneumonia, with CRP having the greatest adjusted odds ratio of 1.79 (95% CI 1.47–2.18). As an isolated predictor, CRP at a cut-off of 3.72 mg·dL−1 demonstrated a sensitivity of 60% and a specificity of 75%. The model incorporating CRP demonstrated improved sensitivity (70.0% versus 57.7%) and similar specificity (85.3% versus 88.3%) compared to the clinical model when using a statistically derived cutpoint. In addition, the multivariable CRP model demonstrated the greatest improvement in concordance index (0.780 to 0.812) compared with a model including only clinical variables.
Conclusion A model consisting of three clinical variables and CRP demonstrated improved performance for the identification of paediatric radiographic pneumonia compared with a model with clinical variables alone.
Abstract
A model incorporating CRP with clinical variables demonstrates improved accuracy compared to a model based on clinical variables alone. Models with CRP may permit judicious use of radiographs and improve antimicrobial stewardship in paediatric pneumonia. https://bit.ly/3s3SVBX
Introduction
Lower respiratory tract infections (LRTI) are costly causes of healthcare visits and admissions in children [1, 2]. Community-acquired pneumonia (CAP) is one of the top three reasons for hospital admission from the emergency department (ED) in children 1–17 years old [3]. Given the substantial burden placed on children by pneumonia and the overlap in clinical features between pneumonia and other respiratory infections in children, accurate prediction of radiographic pneumonia in children carries practical value to minimise unnecessary chest radiography use. In addition, a well-performing prediction model may promote antimicrobial stewardship by limiting antibiotic use in those at low risk of radiographic pneumonia.
Models based on clinical predictors alone may facilitate the prediction of pneumonia among patients with suspected LRTI [4–7]. However, these clinical models are limited in their performance, particularly in the large proportion of patients classified as having intermediate risk of radiographic pneumonia. Several biomarkers, including C-reactive protein (CRP) and procalcitonin (PCT), have been proposed as an objective means to improve the diagnosis of pneumonia; however, biomarkers used in isolation also demonstrate limited performance [8]. The role of biomarkers may be of greatest value in children for whom the risk of pneumonia is in the moderate to severe range where decisions regarding chest radiography are more challenging. While professional societies do not advocate for routine chest radiography for the diagnosis and treatment of radiographic pneumonia [9, 10], the presence of radiographic pneumonia is frequently used to determine a need for antibiotics. As such, an enhanced predictive model may allow for improved antimicrobial stewardship without increasing (and possibly decreasing) the use of chest radiographs among patients at moderate risk of radiographic pneumonia. This is especially true given the recent proliferation of point-of-care biomarker assays. It is likely that combining biomarkers with clinical prediction models for radiographic pneumonia can improve the performance of either biomarkers or clinical features alone.
Biomarkers are not universally obtained in all patients with suspected pneumonia, due to challenges with acquisition and cost. Oostenbrink et al. [11] reported a prediction model that used CRP, in addition to physical examination findings. This study did not compare biomarkers with each other, or their use in combination. Other published prediction models that incorporated biomarkers used a composite outcome for serious bacterial infections, in which pneumonia was one of several different types of infections included. This composite outcome may limit the model's clinical utility to evaluate pneumonia alone [12, 13]. As objective measures, the incorporation of biomarkers may improve the diagnosis of pneumonia beyond clinical models alone, leading to reduced need for radiography and improved antimicrobial stewardship in patients at low risk.
In this study, we evaluated the role of biomarkers in improving the diagnostic accuracy of a clinical prediction model for radiographic pneumonia.
Methods
This study is a secondary analysis of a prospective cohort study (Catalysing Ambulatory Research in Pneumonia Aetiology and Diagnostic Innovations in Emergency Medicine (CARPE DIEM)) of children 3 months to 18 years of age who presented to the ED with signs and symptoms of LRTI and who had chest radiography performed for clinical suspicion of CAP. The current study builds upon our previously published prediction model for radiographic pneumonia [7]. Ethics approval for this study was obtained by the Cincinnati Children's Hospital Medical Center Institutional Review Board (IRB #2012-4959) and the Ann and Robert H Lurie Children's Hospital of Chicago Institutional Review Board (IRB #2018-2056).
Patients with a recent hospitalisation, history of aspiration or with medical conditions that predispose to severe or recurrent pneumonia (e.g., immunodeficiency, neuromuscular disorders impacting respiration) were excluded. After obtaining informed consent from parents and assent from patients >11 years of age, demographic, historical and physical examination data were collected from all participants. A subset of children were consented for the collection of blood biomarkers, including a complete blood cell count, CRP and PCT. Radiograph interpretations were based on consensus of two board-certified radiologists who independently reviewed all radiographs and categorised as: no atelectasis/infiltrate, definitive atelectasis, atelectasis versus pneumonia or definitive pneumonia. Our outcome of radiographic pneumonia was defined as radiologist consensus of atelectasis versus pneumonia or definitive pneumonia [7].
We compared clinical and historical factors of included and excluded patients using Fisher's exact and Wilcoxon rank-sum tests, correcting for multiple comparisons using the Benjamini–Hochberg method. For the current study, we evaluated the incorporation of four biomarkers, individually and in combination, to our previously published clinical model [7] to predict radiographic pneumonia: white blood cell (WBC) count, absolute neutrophil count (ANC), CRP and PCT. We included patients with at least one blood biomarker obtained. Within this subset, we performed multiple imputation with chained equations for patients with missing data [14]. We elected to perform multiple imputation instead of complete case analysis for models, as prior work has suggested that limiting models to those with complete cases can result in biased model performance [15]. However, as a sensitivity analysis, we assessed the performance of these models on the subsets of patients with complete data for each individual biomarker. We evaluated collinearity between biomarkers in pairwise groupings. The association of each biomarker with radiographic pneumonia was evaluated using univariable logistic regression and as part of a multivariable model when incorporated into the published clinical model. Hypothesising that there may be an additive effect of including both CRP and PCT, we evaluated a model limited to CRP and PCT, and another that included clinical variables, CRP and PCT.
For each model, we report the concordance index (c-index), both as a raw c-index and as an optimism-corrected measure, which adjusts for potential overfitting. We report metrics of diagnostic accuracy at an optimally derived cut point using the Euclidean distance method [16]. We constructed calibration curves to inspect the performance of the models, comparing the predicted risk to the observed pneumonia prevalence [17, 18]. As we performed multiple imputation to develop models, we assessed the performance of each when limited to complete cases for each individual biomarker (without imputation). We evaluated if any biomarkers would be retained in backwards stepwise selection bootstrapped over 1000 iterations to obtain a reduced model selected based on the lowest Akaike Information Criterion. Analyses were performed in R v4.0.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Of the 1142 patients enrolled in the parent study, 580 patients consented to and provided blood samples, 213 (36.7%) of whom had a diagnosis of radiographic pneumonia. Within this group, 423 (73%) patients had all four biomarkers, 32 (6%) had three biomarkers, 117 (20%) had two biomarkers and eight (1%) had one biomarker assessed. Compared to excluded patients, patients who had biomarkers performed were more frequently younger, had a prolonged duration of illness and less frequently had rhinorrhoea and wheeze. Included patients had a higher proportion of radiographic pneumonia (37%) relative to excluded patients (7%; supplementary table S1). The median age was 4 years (interquartile range (IQR) 1.6–8.2) and 301 (52%) were boys (table 1). The WBC, ANC and PCT were similar between patients with and without radiographic pneumonia (table 2). The median CRP among patients with radiographic pneumonia (4.7 mg·dL−1, IQR 2.1–11.4 mg·dL−1) was higher than in patients without radiographic pneumonia (1.7 mg·dL−1, IQR 0.7–3.7 mg·dL−1).
Demographics of included patient cohort
Summary statistics for included biomarkers
In univariable analyses, the ANC (odds ratio (OR) 1.38, 95% CI 1.08–1.76) and CRP (OR 1.94, 95% CI 1.63–2.32) was associated with radiographic pneumonia. When adding biomarkers individually into multivariable models that included the three clinical variables in our original model, WBC (adjusted odds ratio (aOR) 1.58, 95% CI 1.07–2.32), ANC (aOR 1.44, 95% CI 1.06–1.96), CRP (aOR 1.79, 95% CI 1.47–2.18) and PCT (aOR 1.30, 95% CI 1.13–1.49) were all statistically associated with radiographic pneumonia (table 3).
Model performance on the addition of individual biomarkers to the clinical model
The clinical feature-only model demonstrated a c-index of 0.79 and an optimism-corrected c-index of 0.78 in the sample of 580 children evaluated in this study. At the optimal cut-off for predicted probability of radiographic pneumonia statistically derived from the receiver operating characteristic (ROC) curve of 50.7%, the clinical model had a sensitivity of 57.7% and a specificity of 88.3%. When evaluating the change in model performance with the addition of biomarkers to the clinical model, the greatest improvement was found incorporating CRP, increasing the c-index to 0.83 and the optimism-correct c-index to 0.81. The CRP model had improved sensitivity (70%) and similar specificity (85%) compared with the clinical model. When assessing model performance on the subset of patients with complete data, there was a small increase in performance for each biomarker (supplementary table S2). Calibration curves for the model applied to the full subset and to the cohort with complete cases are presented in supplementary figure S1.
Models which included these biomarkers in combination, with or without clinical variables, did not demonstrate improved performance compared to the model incorporating CRP and clinical variables. Modelling with CRP and PCT in addition to clinical variables, for example, demonstrated similar performance to the model which only contained CRP with clinical variables (raw c-index 0.83; optimism-corrected 0.81). Modelling with CRP and PCT without clinical factors demonstrated a lower c-index compared with the model incorporating CRP and clinical variables (raw c-index 0.74; optimism-corrected 0.72). Applying bootstrapping of all clinical and biomarker variables, three remained: age, duration of fever and CRP (raw c-index 0.83; optimism-corrected 0.81).
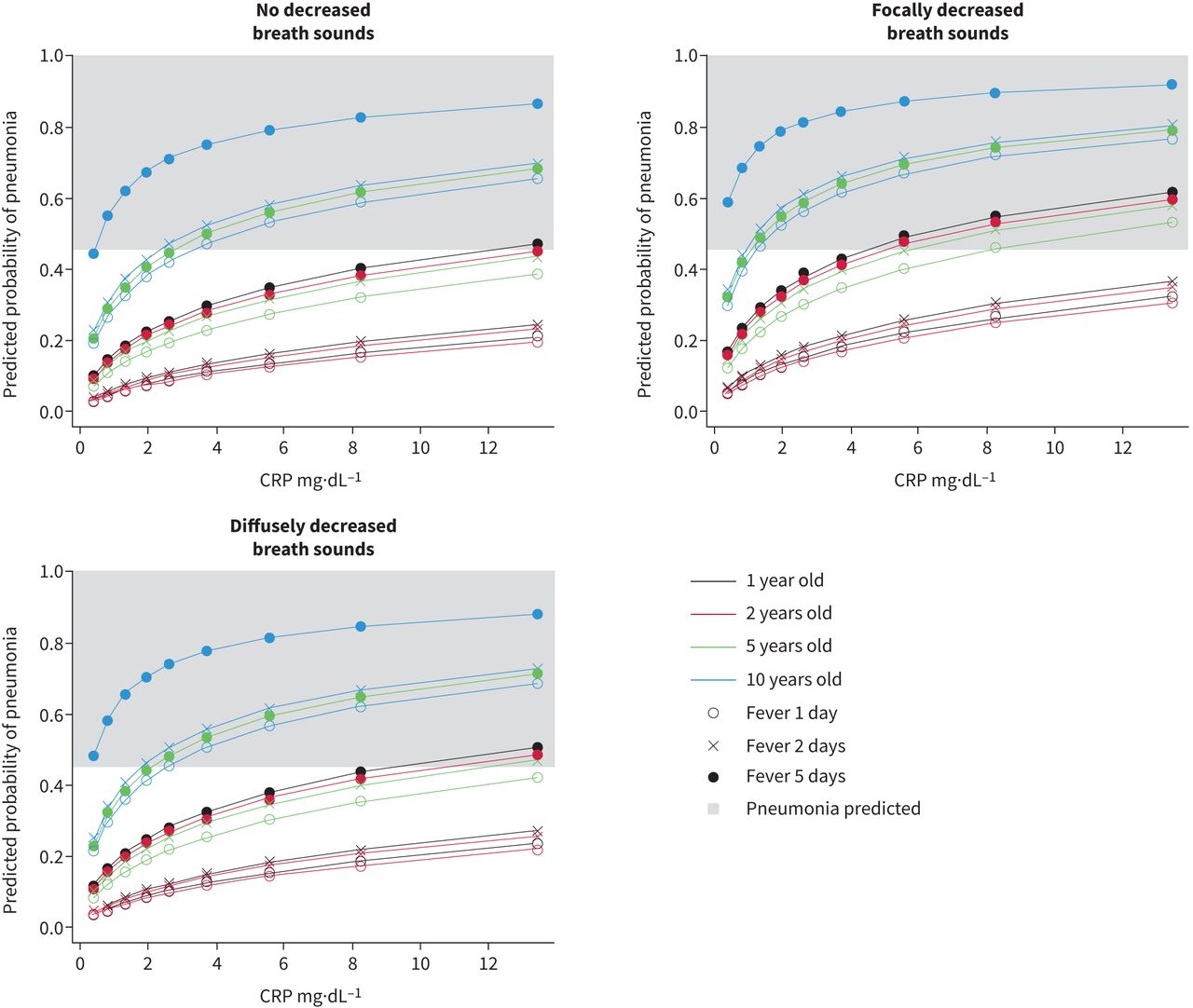
We further evaluated the role of CRP, the strongest associated biomarker, to identify patients with radiographic pneumonia. When evaluating CRP as an individual predictor, the area under the ROC curve was 0.72. In ROC analysis, a CRP of 3.72 mg·dL−1 was the optimal threshold and demonstrated a sensitivity of 60% and a specificity of 75%, though there remained substantial overlap between cases and non-cases (supplementary figure S2). Figure 1 illustrates the role of differing values of CRP when arbitrarily fixing the clinical predictors in a multivariable model.
{kind=link}
Role of C-reactive protein (CRP) in risk prediction of radiographic pneumonia in a prediction model containing clinical factors (focal decreased breath sounds, duration of fever and age) and CRP, when keeping the clinical variables fixed.
Discussion
We evaluated the role of biomarkers in the prediction of radiographic pneumonia in children from a prospective cohort study, individually and in combination, with a previously derived clinical model. WBC, ANC, CRP and PCT demonstrated a statistically significant association with radiographic pneumonia in multivariable models which included a single biomarker in combination with clinical variables. CRP demonstrated the strongest increase in the discriminatory performance of the clinical model from a c-index of 0.780 to 0.812. There was a modest improvement incorporating WBC, ANC and PCT into a multivariable model. Modelling that included both CRP and PCT did not improve performance beyond a model with CRP as the sole biomarker.
The addition of CRP resulted in the strongest improvement of the clinical model, demonstrated by the largest improvements in c-index. We identified improved sensitivity (from 57.7% to 70.0%) with similar specificity (from 74.1% to 73.4%) with the model of CRP plus clinical variables compared to clinical variables alone. However, despite this improvement in the model performance, a single cut-off demonstrates limited utility when used as a one-way rule for the identification of patients at low risk of radiographic pneumonia. Instead, this model may be of greater value when clinicians are provided with continuous predictive probability of pneumonia (from 0 to 100%). Patients at low risk of radiographic pneumonia may not require a chest radiograph to rule out the disease, and those at very high risk may similarly not require a chest radiograph for confirmation. CRP may therefore be most advantageous for patients with an intermediate or equivocal risk when using a clinical rule in order to reduce the number of patients who fall into this category.
Our findings compare to a prior study which used both clinical data and biomarkers to identify patients with radiographic pneumonia. Oostenbrink et al. [11] constructed a multivariable clinical prediction model using backwards stepwise regression to predict radiographic pneumonia in 1290 children, of whom 12.6% had radiographic pneumonia. Ill appearance, tachypnoea and an oxygen saturation <94% were retained in the final multivariable model. The authors suggested that CRP may be of particular benefit in patients within the mid-range of model probabilities (i.e., when only a single clinical criterion is met). Our findings corroborate the improved predictive performance of a model which contains clinical data in addition to CRP.
Point-of-care CRP assays allow for in-office measurement, have comparable accuracy to laboratory assays [19] and are useful in decision-making by primary care providers in determining the need for antibiotics in adults with pneumonia [20]. Furthermore, in-office point-of-care CRP instruments may be more easily accessible to primary care clinicians and less costly compared with chest radiography, which often requires patients to travel to an additional site-of-care to have radiography performed and are more costly. Biomarker-based predictive models which demonstrate generalisability through external validation could help improve diagnostic accuracy of children deemed at moderate risk of pneumonia using clinical variables or CRP alone. Children who are at low risk for radiographic pneumonia based on the predictive model may be candidates for observation without antibiotics after shared decision-making.
PCT was associated with radiographic pneumonia in univariable and multivariable models; however the association was more modest compared to CRP. PCT has previously demonstrated modest predictive value for disease severity both among children with suspected CAP in the ED (from the CARPE DIEM cohort) [21] and in children hospitalised with CAP, with its strongest prognostic effect in differentiating those who develop the most severe outcomes from other less severe cases [22]. This association of PCT with disease severity is likely related to the ability of PCT to predict bacterial illness, whereas PCT is not as strong a predictor of radiographic pneumonia, as this may be caused by either viral or bacterial aetiologies. In one meta-analysis which evaluated the role of PCT in the diagnosis of bacterial pneumonia, PCT demonstrated an area under the curve of 0.70; however the outcome of bacterial pneumonia included radiographic findings and microbiological evidence of bacterial aetiology, different from the present study focused on radiographic findings alone [8].
We found no additional benefit of including PCT in multivariable models for the prediction of radiographic CAP over models with clinical findings and CRP. This has been corroborated among prospective studies among adults with suspected CAP [23]. Radiographic pneumonia may be viral or bacterial in aetiology with CRP, a general marker for inflammation regardless of aetiology. PCT elevation is more correlated with bacterial aetiology. In one prospective study evaluating the role of CRP in the pre-pneumococcal vaccine era, for example, no difference was identified in CRP among patients with pneumococcal (n=57), atypical (n=43) or viral (n=29) pneumonia [24].
Our results support the premise of prior studies that WBC and ANC are of low utility in the identification of patients with radiographic pneumonia [11]. When compared with clinical models, their additive predictive power over a clinical model without biomarkers was low. Although complete blood counts are frequently obtained among children with suspected pneumonia in the ED [25], our findings are consistent with prior literature suggesting that these measures have poor discrimination between pneumonia of viral and bacterial aetiology [8] and disease severity [21, 26]. This finding also corroborates the prior model reported by Oostenbrink et al. [11], which noted that the addition of WBC did not improve the predictive capability of an underlying model that included clinical predictors with CRP [11].
Our findings are subject to limitations. Biomarkers were only available for a subset of patients of the overall study sample, potentially leading to ascertainment bias. Our comparison of children who did and did not receive testing for biomarkers suggested that those who had testing were of higher acuity (based on duration of symptoms, presence of oxygen desaturation and physical examination findings of respiratory distress). A more generalisable study would include all children suspected of pneumonia, regardless of disease acuity. However, as venepuncture is not otherwise clinically required for children with low acuity disease, there may be concerns with the feasibility of such an approach. Nevertheless, the population studied in the present investigation is also the one that will be most likely to benefit from the incorporation of biomarkers in clinical decision-making. Not all biomarkers were measured among the included patients and missing data appeared to not be randomly absent with respect to our primary outcome. However, our multiple imputation models converged in our analysis, and models demonstrated similar performance when limited to patients with complete data. As with all predictive models, external validation is a requisite step prior to clinical implementation. While our outcome of interest was based on chest radiographs performed during the ED encounter, concern might exist regarding potentially missed cases of pneumonia during the initial presentation of illness or in children who are dehydrated [27]. Recent data in children, however, suggest that the negative predictive value for chest radiograph is high for pneumonia (98.8%), with few children with normal chest radiographs subsequently being diagnosed with pneumonia, suggesting that this phenomenon may not occur as frequently as previously thought [28]. Despite these limitations, our findings provide useful data on the additive role of biomarkers in the predictive modelling of patients with radiographic pneumonia.
In this prospective study, adding CRP to a parsimonious three-variable clinical prediction model may have moderate utility in predicting radiographic CAP in children with LRTI. With external validation, particularly with a focus on including children that might be of lower acuity, CRP may improve discrimination of patients with pneumonia and thereby reduce utilisation of chest radiography, primarily driven by improved sensitivity. These results suggest that for patients with higher acuity disease similar to the population studied in this investigation, use of a clinical prediction model combined with CRP could be a viable solution in settings where chest radiography may be difficult to obtain, including primary care, urgent care and potentially low resource emergency settings to guide chest imaging and antimicrobial decisions.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Figure S1 00339-2022.figureS1
Figure S2 00339-2022.figureS2
Table S1 00339-2022.tableS1
Table S2 00339-2022.tableS2
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: The authors have nothing to disclose.
Support statement: This study was supported by the National Institutes of Health (NIH)/National Institute of Allergy and Infectious Diseases (K23AI121325 and R03AI147112 to T.A. Florin and K01AI125413 to L. Ambroggio), the Gerber Foundation (to T.A. Florin), and NIH/NCRR and Cincinnati Center for Clinical and Translational Science and Training (5KL2TR000078 to T.A. Florin). The funders did not have any role in study design, data collection, statistical analysis or manuscript preparation. S. Ramgopal was sponsored by PEDSnet (Department of Pediatrics, Ann and Robert H. Lurie Children's Hospital of Chicago). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received July 8, 2022.
- Accepted October 12, 2022.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions@ersnet.org
References










