





Abstract
Introduction Exercise limitation is frequently described among asthmatic patients and could be related to different mechanisms of the pulmonary, cardiovascular and muscular systems. Despite this, cardiopulmonary exercise testing (CPET) does not have an established role in the management of severe asthma. The aim of our study was to investigate the role of CPET and inspiratory pressure measurement in exercise capacity and muscle strength in severe asthmatic patients treated with anti-IL-5 therapy.
Methods A monocentric observational study was conducted at Hanover Medical School, Germany, from April 2018 to June 2019. Patients affected by severe asthma treated with either mepolizumab or benralizumab were included. All patients underwent CPET before the initiation of antibody therapy and after 3 months, and follow-up visits were scheduled at 3, 6 and 12 months with plethysmography, inspiratory pressure measurement and blood gas analysis.
Results 14 patients were enrolled: 10 (71.4%) females, median age 52 years (IQR 47–61). Seven patients were treated with benralizumab, seven with mepolizumab. Oxygen uptake (V′O2 peak) did not change significantly after 3 months of antibody treatment, while the mean value of the breathing reserve exhaustion reduced significantly from 78% to 60% (p=0.004). Whereas at baseline seven patients depleted the breathing reserve and two of them experienced oxygen desaturation during exercise, at 3 months no one presented any desaturation or breathing reserve exhaustion. The inspiratory pressure remained unchanged before and after the antibody therapy.
Conclusion CPET could show hints of alveolar recruitment and ventilatory efficiency in severe asthma patients treated with antibody therapy.
Abstract
14 severe asthma patients performed exercise tests before and after the initiation of monoclonal drug. After 3 months, an improvement of ventilatory efficiency was detected. Antibody drugs may improve alveolar recruitment in severe asthma. https://bit.ly/3X7bhAc
Introduction
Asthma is a chronic respiratory disease characterised by reversible airflow limitation and heterogeneous symptoms, such as wheezing, cough and dyspnoea [1]. Some patients can experience exercise limitation due to exertional dyspnoea and fatigue, and this is usually associated with worse quality of life [2, 3]. Exercise limitations can be caused by different underlying mechanisms of the pulmonary, cardiovascular and muscular systems. The pathophysiological mechanisms of exertional dyspnoea have been described in detail in COPD and interstitial lung diseases, but limited data are available about exercise limitation in asthma [4, 5]. New antibody drugs against interleukin-5 (Il-5) and its receptor (IL-5-R) approved in severe asthma demonstrated reduction of exacerbation, corticosteroid sparing and improvement of forced expiratory volume in 1 s (FEV1) and quality of life [6, 7].
A review conducted by Vermeulen et al. [8] identified different factors related to activity limitation in asthmatic patients, such as respiratory muscle weakness, deconditioning, ventilator impairment and dynamic hyperinflation. Furthermore, they reported that the administration of bronchodilation therapy prior to cardiopulmonary exercise testing (CPET) did not improve the exercise capacity. A randomised controlled trial was conducted by Van der Meer and colleagues [9] to investigate the effect of corticosteroid therapy on dynamic hyperinflation in patients with moderate-to-severe asthma. The authors found that after 2 weeks of triamcinolone therapy the degree of dynamic hyperinflation was reduced by 23.2%.
P0.1 is the pressure generated during the first 0.1 s of normal inspiratory effort against occluded airways, and it reflects the central ventilatory drive, since the occlusion time is too short to be influenced by muscle weakness or by consciousness [10]. The maximal inspiratory pressure (MIP) generated during a maximal inspiration effort against closed airways is an indicator of respiratory muscles’ strength and ventilator pump efficiency. Low MIP may be due to submaximal effort, muscular weakness, elevated functional residual capacity with hyperinflation and/or neuromuscular diseases [10]. P0.1/MIP ratio was largely studied as a prognostic factor for mechanical ventilation weaning and extubation success. This ratio denotes the balance between the ventilatory drive (respiratory demand) and the muscular strength (the ability of the respiratory system to respond) [11, 12].
Yet no data are available about the role of CPET and inspiratory pressure measurement as indicators of clinical improvement or prognostic tools in severe asthmatic patients treated with anti-eosinophil therapy. We combined the exercise test parameters plethysmography and P0.1 and MIP measurement to assess the impact of anti-IL-5 therapy on exercise capacity and respiratory muscle strength in patients affected by severe eosinophilic asthma.
Methods
Study population and treatment
This prospective observational, monocentric study was conducted in the severe asthma outpatient clinic of Hanover Medical School (Germany) from April 2018 to June 2019. Patients affected by severe asthma, as defined by American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines [13], treated with either anti-IL-5 (mepolizumab) or anti-IL-5 receptor (benralizumab) antibodies were included. All patients provided written informed consent to use their medical records with approval of the local institutional review board (9171_BO_K_2020).
Patients underwent CPET before introduction of antibody therapy and after 3 months. Clinical records were screened and the following parameters available at baseline and at follow-up visits at 3 months, 6 months and 12 months were collected: 1) clinical history and socio-demographic data; 2) functional tests such as body plethysmography with P0.1 and MIP measurement and blood gas analysis; 3) blood eosinophil count; and 4) quality of life assessment, performed with the Asthma Control Test (ACT) questionnaire (figure 1). All the pulmonary function tests and CPET parameters available were compared across the follow-up time.
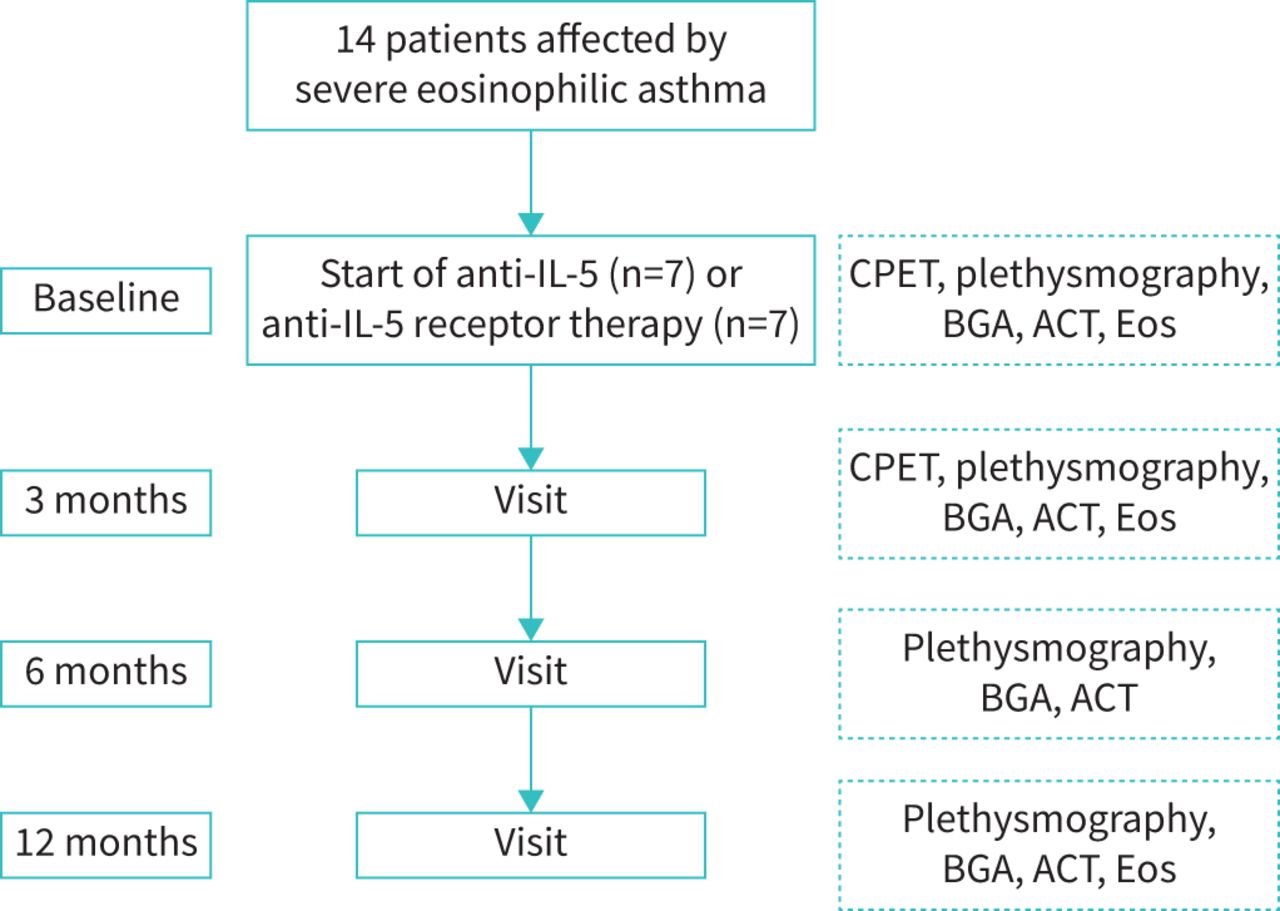
Flowchart of study design. IL-5: interleukin-5; CPET: cardiopulmonary exercise test; BGA: blood gas analysis; ACT: Asthma Control Test; Eos: eosinophils.
All patients were treated according to the current guidelines for severe asthma [1, 13, 14].
All patients included in the study were older than 18 years and naive from any monoclonal drug for severe asthma for at least 6 months. All patients signed an informed written consent. All patients were able to perform CPET and had no history of heart failure or neuromuscular disorders.
Exercise testing and inspiratory work
Exercise testing was performed using a bicycle ergometer by MGC Diagnostics™ (Saint Paul, MN, USA) with a GE™ eBike (Boston, MA, USA). According to patients’ fitness status, an optimised ramp was used and equally maintained for the baseline and follow-up test. All patients were encouraged to reach maximal exhaustion until symptom-limitation (e.g. dyspnoea or fatigue) if no other termination criterion was reached before, and we used the BORG dyspnoea questionnaire immediately after test-ending. All tests were performed according to current guidelines for CPET [15] with continuous monitoring of 12-lead electrocardiogram, blood pressure and oxygen saturation.
Blood gas analysis was performed through earlobe sting and collection of capillary blood [16].
Plethysmography was performed following the current German recommendations [17] and ERS guidelines [18]. All parameters were recorded, in particular P0.1, which represents the negative airway pressure generated during the first 100 ms of an occluded normal inspiration, and MIP, the MIP pressure generated during maximal breathing effort. These values and their index are markers of respiratory muscle strength.
Definitions
Definitions and reference values are settled according to ATS statement 2003 and ERS statement 2019 and reported as percentage of the predicted value (%) [15, 19]. The acronyms used replicated the ERS and ATS/American College of Chest Physicians (ACCP) statement glossaries: oxygen uptake at peak exercise (V′O2 peak), carbon dioxide output at peak exercise (V′CO2 peak), anaerobic threshold (AT), ventilation (VE), maximum voluntary ventilation (MVV), inspiratory capacity (IC), ventilatory equivalent for carbon dioxide (VE/V′CO2), respiratory rate (RR), tidal volume (VT), end-expiratory lung volume (EELV), arterial oxygen saturation as indicated by pulse oximetry (SpO2), partial pressure of oxygen (PO2) and partial pressure of carbon dioxide (PCO2). The consumption of oxygen (V′O2) was always considered corrected for body weight (mL·kg·min−1).
Normal values were settled as V′O2 peak (mL·kg·min−1) ≥85%, O2 pulse (mL/bpm) ≥80%, breathing reserve (BR, VE peak/MVV) <85%, VE/V′CO2 slope <35 and VT/IC >0.75. MVV was extrapolated from the FEV1 (35×FEV1). Desaturation was defined as either a reduction of at least 5% of SpO2 during exercise or capillary PO2 <60 mmHg at blood gas analysis.
Deconditioning was defined as low V′O2 peak with normal or low O2 pulse, no desaturation and normal breathing reserve. Cardiovascular limitation was distinguished by low V′O2 peak and low O2 pulse, normal breathing reserve and no sign of desaturation. Respiratory limitation was characterised by low V′O2 peak, desaturation and/or breathing reserve depletion [20, 21].
Dynamic hyperinflation was defined as elevation of EELV ≥0.250 L during exercise and decrease of IC >0.2 L [10, 20]. Dynamic hyperinflation was also ruled out observing the flow-volume loops during the exercise [10, 20, 22].
Outcomes
At baseline and at every follow-up visit, lung function test, ACT questionnaire and clinical assessment were recorded. At least two of the following criteria defined a positive response to monoclonal therapy as defined by Drick et al. (2018) [23]: 1) self-reported clinical improvement in terms of quality of life, physical performance and symptoms control; 2) rise of the predicted value of the FEV1 % of at least 12% or 200 mL; and 3) eosinophil count reduction to <150 µL−1 or to <20% of the baseline value. At 12 months, two groups of patients were identified, those who achieved two or more goals (responders) and those who did not (non-responders).
Finally, P0.1 value was compared across two groups: patients who at baseline were under chronic oral corticosteroid therapy (chronic OCS) versus patients who were not (OCS-free).
Statistical analysis
The software IBM SPSS Statistics 27.0 (IBM Corp, Armonk, NY, USA) was used to analyse the data. Non-parametric continuous variables were presented as median (interquartile range, IQR), normal continuous variables as mean±sd and categorical variables as n (%).
For comparisons of time points, a paired t-test or Wilcoxon test, linear model for repeated measures and t-test or Mann–Whitney test were used as appropriate. All reported p-values are two-sided. p-values below 0.05 were considered statistically significant.
Results
A total of 14 patients were enrolled; baseline characteristics are shown in table 1.
Baseline characteristics of the study population (n=14)
Results from CPET showed no significant changes over 3 months in maximum load, V′O2 peak, ventilatory efficiency, respiratory rate, tidal volume or arterial blood pressure. Dynamic hyperinflation could not be found in patients either before or after antibody treatment.
Although the mean capillary pO2 value did not differ between the two timepoints, desaturation during exercise was observed in two patients at baseline. After 3 months of therapy, both these subjects experienced a marked improvement in lung function and gas exchanges (FEV1 raised by 33% and 38% and capillary pO2 at rest raised by 9 mmHg and 6 mmHg, respectively) and desaturation was no longer detected.
The mean value of the breathing reserve exhaustion reduced significantly from 78% to 60% (p=0.004). At baseline seven (50%) patients showed depleted breathing reserve, and after 3 months, all of them improved.
Furthermore, the mean±SD of the ventilation per minute at rest reduced significantly from 17±3 L·min−1 at baseline to 15±3 L·min−1 after 3 months (p=0.035). Details are given in the supplementary material.
The lung function tests improved after the initiation of antibody therapy; data across the 12 months of follow-up are presented in table 2.
Functional parameters before and under antibody treatment
The inspiratory work and the ventilatory drive (P0.1, MIP and P0.1/MIP ratio) remained unchanged before and after antibody therapy. As a response to anti-eosinophilic therapy, the mean number of circulating eosinophils dropped significantly from 905·µL−1 to 35·µL−1 (p=0.001).
Outcome
After 6 months non-response to antibody therapy was diagnosed in one patient, after 12 months non-response was found in two (14.3%) patients. The first patient showed significant decrease of circulating eosinophil granulocytes but still suffered from exacerbations, FEV1 remained unchanged and OCS were still needed. The other patient maintained clinical stability until 6 months, then he experienced several exacerbations and FEV1 dropped. After 12 months, both patients were switched to dupilumab therapy.
Among the overall population, at baseline 10 (71.4%) patients reported at least two exacerbations per year, while at 12 months only four (28.6%) patients experienced two or more exacerbations. One patient withdrew from OCS therapy.
Inspiratory pressure and corticosteroid therapy
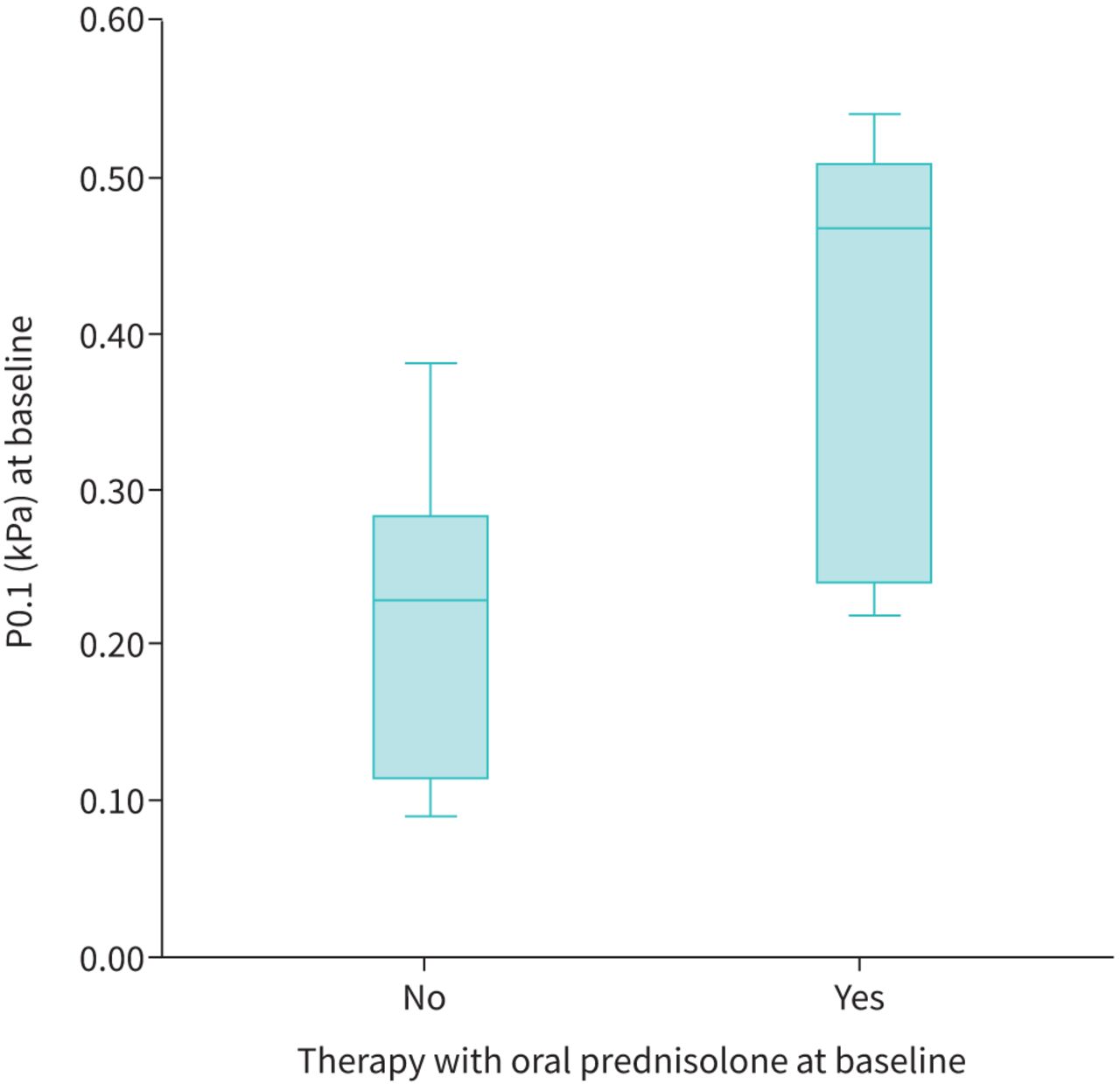
P0.1 was compared between patients with chronic oral corticosteroid therapy (chronic OCS) at baseline and patients without OCS treatment (OCS-free). Both groups were composed of seven subjects. P0.1 was higher in the chronic OCS group, although this difference was not significant (p=0.106). MIP was similar between the two groups (see table 3 and figure 2).
Comparison of inspiratory pressure values at baseline between patients under OCS versus patients without OCS treatment
{kind=link}
{kind=link}
Comparison of P0.1 values at baseline between patients under oral corticosteroid (OCS) versus patients without OCS treatment.
Discussion
This is the first study evaluating anti-IL-5/-R antibodies using CPET and respiratory work tests. Our results demonstrate the subjective improvement along with gain in lung function and gas exchanges after the initiation of anti-eosinophilic therapy, in line with previous studies on mepolizumab and benralizumab [6, 7]. In addition, despite the small number of participants, we found hints that OCS does influence the inspiratory muscle strength.
Treatment with anti-eosinophilic antibodies did not improve the exercise performance in terms of V′O2 peak or workload. This finding is in contrast with the study by Schäper and colleagues [24], who compared a cohort of severe asthmatic patients that underwent omalizumab therapy to severe asthma patients not treated with antibodies. This difference could depend on the deconditioned performance status of the antibody treatment group, which showed a baseline V′O2 peak of 13.8 that increased to 16.8 mL kg−1·min−1 (p<0.05). The control group had a median V′O2 peak of 19.4 and 18.8 mL kg−1·min−1 at follow-up. These values were comparable to those in our patients before antibody initiation. The relatively high oxygen uptake of the control group or our patients left no room for further improvement. In our cohort, the mean± sd V′O2 peak was 19±4.7 mL kg−1·min−1, indicative of quite fit patients. In line with Schäper et al., our results supported the argument that there is improvement of gas exchanges after antibody therapy. At baseline two patients presented with desaturation during exercise, but after the initiation of anti-IL-5 therapy both of them improved and showed no more desaturation at follow-up CPET. Consistent with this, both of them experienced symptom improvement, gain of FEV1 and raise of capillary pO2 at rest and during exercise. Furthermore, seven patients depleted their breathing reserve during baseline exercise, and all of them restored it to normal values after 3 months of anti-IL-5 therapy.
Other indicators of improvement in ventilatory efficiency were the reduction of respiratory rate at the peak of exercise (from 36·min−1 to 31·min−1, p=0.058) and gain of capillary pO2 at rest (from 72 to 80 mmHg, p=0.004). No differences were detected in terms of tidal volume during exercise.
To our knowledge, no previous studies have analysed gas exchanges and exercise capacity through CPET before and after the initiation of anti-IL-5 therapy in severe asthma patients. A recent review by Boutou et al. [21] reported data about ventilation/perfusion inequality induced by physical exercise in asthmatic patients. The uneven ventilation and the ventilation/perfusion inequality could be explained by bronchoconstriction and airways inflammation, since arterial pO2 and the alveolar to arterial oxygen pressure difference (A-aDO2) were negatively correlated to the increase in histamine concentration in sputum, as demonstrated by Haverkamp and colleagues [25]. Since gas exchanges and airflow limitation depend on the airways calibre and benralizumab and mepolizumab have an anti-inflammatory effect on the respiratory tract and contribute to the increase in FEV1, it is plausible that IL-5 antibodies improve the ventilatory homogeneity and the respiratory efficiency [26, 27]. In fact, in a recent analysis by Abdo et al. [28], exercise limitation and poor symptoms control were strongly correlated and have been associated with small airway dysfunction in asthmatic patients.
The benefits of anti-inflammatory therapy on exercise capacity were previously described by Van der Meer et al. [9], who analysed the response to corticosteroid treatment in a cohort of moderate-to-severe asthmatic patients. In their study, dynamic hyperinflation was significantly reduced by systemic glucocorticoid therapy, suggesting that anti-inflammatory treatment could improve exercise capacity and quality of life. Although in our population the dynamic hyperinflation was not detected in any patient in CPET, we found a reduction of residual volume (RV) from 139% to 124% (p=0.030) and RV/total lung capacity from 47% to 41% (p=0.013) in 12 months after antibody initiation. In addition, as specific airway resistance dropped (127% to 87%; p=0.004) and FEV1 and forced vital capacity increased, we believe that mepolizumab and benralizumab decreased oedema and inflammatory cell infiltration in the respiratory tract, resulting in enhanced airway calibre, control of small airways disfunction and alveolar recruitment [28–30].
MIP is an indicator of the strength of respiratory muscle, which depends on the mechanical characteristics of the lungs, emphysema, hyperinflation and long-term steroid therapy [31–33]. We did not find changes from baseline to follow-up measurement in severe asthma patients under antibody therapy. Similarly, no differences were observed for P0.1 or P0.1/MIP values.
However, contrasting data are available about the impairment of muscular strength in asthmatic patients. A study by Ferreira Pereira and colleagues [34] evaluated the 6-min walk test, spirometry and measurement of respiratory muscle strength in 25 subjects with severe uncontrolled asthma and found no changes even if oral corticosteroid use was taken into account. In contrast, De Bruin et al. [35] demonstrated reduced MIP and greater diaphragm thickness in asthmatic patients compared to healthy controls, while no differences were detected in the strength of limb muscles. However, a significant improvement of respiratory muscle efficiency was demonstrated by Weiner and colleagues [36] after administration of bronchodilator therapy. These contradictions could be explained by the heterogeneous nature of asthma.
As oral corticosteroids could lead to muscular weakness and hypotrophy [37, 38] we compared patients who were under steroid therapy at baseline with OCS-free patients. The MIP value was similar between the two groups, but patients treated with long-term OCS therapy had P0.1 values higher than patients without OCS treatment (median values 0.47 versus 0.23 kPa respectively, p=0.106; see table 3 and figure 2). This difference was not significant, but a trend was observed, and this finding is likely to be significant considering a larger sample size. Unfortunately, we could not conduct an analysis comparing P0.1 and MIP with different OCS dosage because of the small sample size, but it could be an interesting field for further studies.
Limitations
The major limitations of our study are the small sample size of the studied population and its monocentric nature. Therefore, it is not possible to compare different subgroups, and there is no parallel or control group. For this reason, the proposed work could be considered as a feasibility study or a pilot study.
In addition, in a real life setting, asthmatic patients have several comorbidities, which may influence the response to physical exertion [1, 3, 39].
Another limitation was related to the correlation between breathing reserve and FEV1. As MVV was derived from FEV1 (35×FEV1), breathing reserve improvement could be partly related to the increase in FEV1.
Our study could be enhanced by adding a control group composed of severe asthma patients not treated with antibody therapy and performing CPET again at 6 and/or 12 months, to verify the effects of re-training and limb muscle strength and endurance.
CPET is very useful for analysing the pathophysiological mechanism of dyspnoea and exercise limitation, but requires expensive instruments, time and staff. Severe asthma clinics may not have the time and resources to perform CPET in every patient on a regular basis.
Conclusion
This is the first study to evaluate CPET and respiratory muscle function after antibody therapy. These data give more insight into functional changes and help clinicians to understand the pathophysiological changes and improvements under therapy, although its added value in everyday clinical practice remains questionable. The anti-inflammatory effect of anti-IL-5 antibodies decreased oedema and inflammatory cell infiltration in the respiratory tract, resulting in enhanced airway calibre and alveolar recruitment and improved ventilatory efficiency. For OCS long-term therapy, we found some changes in P0.1, but its role and clinical value remain unclear.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00341-2022.SUPPLEMENT
Footnotes
Provenance: Submitted article, peer reviewed
Ethics approval and consent to participate: All patients provided written informed consent to use their medical data and all retrospective analyses were performed with approval of the local institutional review board (9171_BO_K_2020).
Availability of data and materials: the datasets generated during and/or analysed during the current study are available from the corresponding author upon individual and specific request. The use of individual data of patients outside specific personal consultation will not be permitted.
Author contributions: Conceptualisation, project administration: H. Suhling, N. Drick and T. Welte. Data collection: H. Suhling, E. Franceschi and B. Fischer. Methodology and data analysis: E. Franceschi and J. Fuge. All authors discussed the results, and contributed to writing, review and editing. All authors read and approved the final manuscript.
Conflict of interest: None declared.
- Received July 10, 2022.
- Accepted November 9, 2022.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










