





Abstract
Objective To determine whether changes in pulmonary vascular resistance (PVR) and changes in pulmonary artery compliance (Cpa) are associated with changes in exercise capacity assessed either by changes in peak oxygen consumption (V′O2) or by changes in 6-min walk distance (6MWD) in patients with chronic thromboembolic pulmonary hypertension (CTEPH) undergoing balloon pulmonary angioplasty (BPA).
Methods Invasive haemodynamic parameters, peak V′O2 and 6MWD were measured within 24 h, before and after BPA (interval 3.1±2.4 months) in 34 CTEPH patients without significant cardiac and/or pulmonary comorbidities, of whom 24 received at least one pulmonary hypertension-specific treatment. Cpa was calculated according to the pulse pressure method: Cpa=((SV/PP)/1.76+0.1), where SV is the stroke volume and PP is the pulse pressure. The resistance–compliance (RC)-time of the pulmonary circulation was calculated as the PVR and Cpa product.
Results After BPA, PVR decreased (562±234 versus 290±106 dyn·s·cm−5; p<0.001); Cpa increased (0.90±0.36 versus 1.63±0.65 mL·mmHg−1; p<0.001); but RC-time did not change (0.325±0.069 versus 0.321±0.083 s; p=0.75). There were improvements in peak V′O2 (1.11±0.35 versus 1.30±0.33 L·min−1; p<0.001) and in 6MWD (393±119 versus 432±100 m; p<0.001). After adjustment for age, height, weight and gender, changes in exercise capacity, assessed either by peak V′O2 or 6MWD, were significantly associated with changes in PVR, but not with changes in Cpa.
Conclusions Contrary to what has been reported in CTEPH patients undergoing pulmonary endarterectomy, in CTEPH patients undergoing BPA, changes in exercise capacity were not associated with changes in Cpa.
Abstract
Pulmonary arterial compliance and exercise capacity after balloon pulmonary angioplasty in CTEPH https://bit.ly/408N6SJ
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is an uncommon complication of pulmonary embolism that results from occlusion of large pulmonary arteries by persistent thrombi and from distal small-vessel vasculopathy [1]. The pulmonary vascular lesions lead to increased right ventricle (RV) afterload and, as the condition progresses, result in reduced oxygen delivery due to inadequate cardiac output that is clinically manifested by progressive limitation of exercise. Balloon pulmonary angioplasty (BPA) has recently emerged as a valuable treatment option for carefully selected CTEPH patients [2, 3]. BPA improves symptoms, exercise capacity and, in most cases, near-normalises pulmonary vascular resistance (PVR) measured at rest. Nevertheless, improvement in exercise capacity, assessed either by peak exercise oxygen consumption (V′O2) or by distance walked in 6 min (6MWD), is highly variable between patients [4–6], suggesting that factors other than changes in resting PVR may influence changes in exercise capacity.
Decrease in RV afterload is considered an important mechanism for improvement in exercise capacity after intervention on pulmonary arteries [7]. In the absence of right heart failure, the two main components of RV afterload are PVR and pulmonary artery compliance (Cpa) [8]. It has been supposed that the PVR and Cpa product (resistance–compliance (RC)-time) is unaltered in health and disease, meaning that Cpa can always be deduced from PVR. Nevertheless, the concept of unaltered RC-time in healthy and diseased subjects has been questioned [8, 9], notably in CTEPH patients undergoing pulmonary endarterectomy (PEA) whose RC-time has been found to be ∼20% lower after surgery than before [10]. It is therefore plausible that Cpa provides information that PVR does not about right heart function and exercise capacity.
In the current study, our aims were 1) to study the relationship between exercise capacity (6MWD and peak V′O2) on the one hand, and pulmonary haemodynamic parameters (PVR and Cpa) on the other, before and after BPA, and 2) to study the effects of BPA on PVR, Cpa and RC-time in order to question the concept of a “constant” RC-time in patients with CTEPH undergoing BPA.
Methods
Subjects
All patients referred for BPA at our institution between March 2019 and November 2020 were considered for inclusion. The eligibility criteria for BPA and the techniques used have been described elsewhere [11]. Patients included in the current study underwent two evaluations (pre- and post-BPA) including right heart catheterisation, symptom-limited incremental cardiopulmonary exercise test and 6-min walk test within 24 h. To avoid factors other than BPA that may contribute to impact on exercise capacity, we excluded post-BPA evaluations performed >3 months after the last BPA session. Patients who had any change in pulmonary hypertension targeted therapy between the two evaluations were excluded from the analysis. Patients with an obstructive ventilatory disorder and/or interstitial lung disease, and/or pulmonary arterial wedge pressure (PAWP) >15 mmHg and/or with right heart failure were also excluded.
The study protocol was approved by the institutional review board (Comité de Protection des Personnes Sud-Est V, 2013-AO1036-39), and all patients were informed about the potential risks and benefits of BPA and provided written informed consent.
Study procedures
All catheterisation measurements were performed in the supine position at rest with standard techniques. Pressures were measured using a Swan–Ganz catheter (Edwards Lifesciences, Irvine, CA, USA) connected to a pressure transducer. Pressure measurements were taken at end-expiration. Cardiac output (CO) was measured by thermodilution; cardiac index was calculated as CO divided by the body surface area. PVR was calculated as (mPAP − PAWP)/CO, where mPAP the mean pulmonary artery pressure. Cpa was calculated as (SV/PP)/1.76+0.1, where SV is the stroke volume (i.e. CO divided by cardiac beat frequency) and PP is the pulse pressure (i.e. systolic pulmonary arterial pressure minus diastolic pulmonary arterial pressure) [12]. The RC-time (in seconds), which characterises the decay of pulmonary arterial pressure in diastole, was calculated as the PVR and Cpa product (PVR×Cpa).
Cardiopulmonary exercise tests were performed on an electronically braked cycle ergometer (Ergometrics 900; Ergoline, Bitz, Germany), as described previously [13], without adjunction of oxygen, even in patients with arterial oxygen desaturation. Blood samples were drawn from the arterialised earlobe to measure carbon dioxide (CO2) and oxygen at peak. Arterial carbon dioxide and arterialised CO2 were considered as equivalent, and appropriate corrections were made to estimate arterial oxygen from arterialised oxygen [14]. Oxygen consumption (V′O2), carbon dioxide output and minute ventilation were obtained breath-by-breath (Ergocard CPX; Medisoft, Sorrines, Belgium).
6-min walk tests were performed as described previously [15].
Statistical analysis
Results are presented as mean±sd and n (%) for continuous and categorical data, respectively. Comparisons of continuous parameters pre- and post-BPA were performed using the t-test for paired data. Categorical parameters were compared using the McNemar test. Univariate regression analysis was used to study the relationship between changes in peak V′O2 and 6MWD, and changes in PVR and Cpa. Multivariate regression analysis was used to adjust for the effect of age, height, weight and gender to determine whether there was any effect of changes in PVR and Cpa on changes in peak V′O2 and 6MWD. Adjustment for age, height, weight and gender were made a priori as these four parameters are known to influence 6MWD and peak V′O2 [16, 17]. The same analyses (univariate and multivariate regression analyses) were made with the SV/PP ratio instead of Cpa.
All analyses were performed using R software (version 3.6) and a p-value <0.05 was considered as significant.
Results
The selection of patients is summarised in figure 1. For the 34 patients included in the analysis, the mean±sd interval between the two evaluations was 3.1±2.4 months and the mean number of BPA sessions was 4.7±1.7. After BPA, improvements in New York Heart Association functional class, N-terminal pro-brain natriuretic peptide and haemodynamic parameters (in particular, mPAP, cardiac index and PVR) were all significant (table 1).

Flowchart of the study. BPA: balloon pulmonary angioplasty; CTEPH: chronic thromboembolic pulmonary hypertension; ILD: interstitial lung disease; LHF: left heart failure; PH: pulmonary hypertension.
Clinical characteristics and haemodynamic parameters before and after balloon pulmonary angioplasty (BPA) in the 34 included patients with chronic thromboembolic pulmonary hypertension
After BPA, Cpa increased significantly, but the RC-time did not change (table 1). Peak V′O2 and 6MWD increased significantly, by 0.19±0.20 L·min−1 and 39±60 m, respectively (table 2).
Cardiopulmonary exercise testing (CPET) variables obtained at peak exercise and variables measured during 6-min walk test (6MWT) before and after balloon pulmonary angioplasty (BPA)
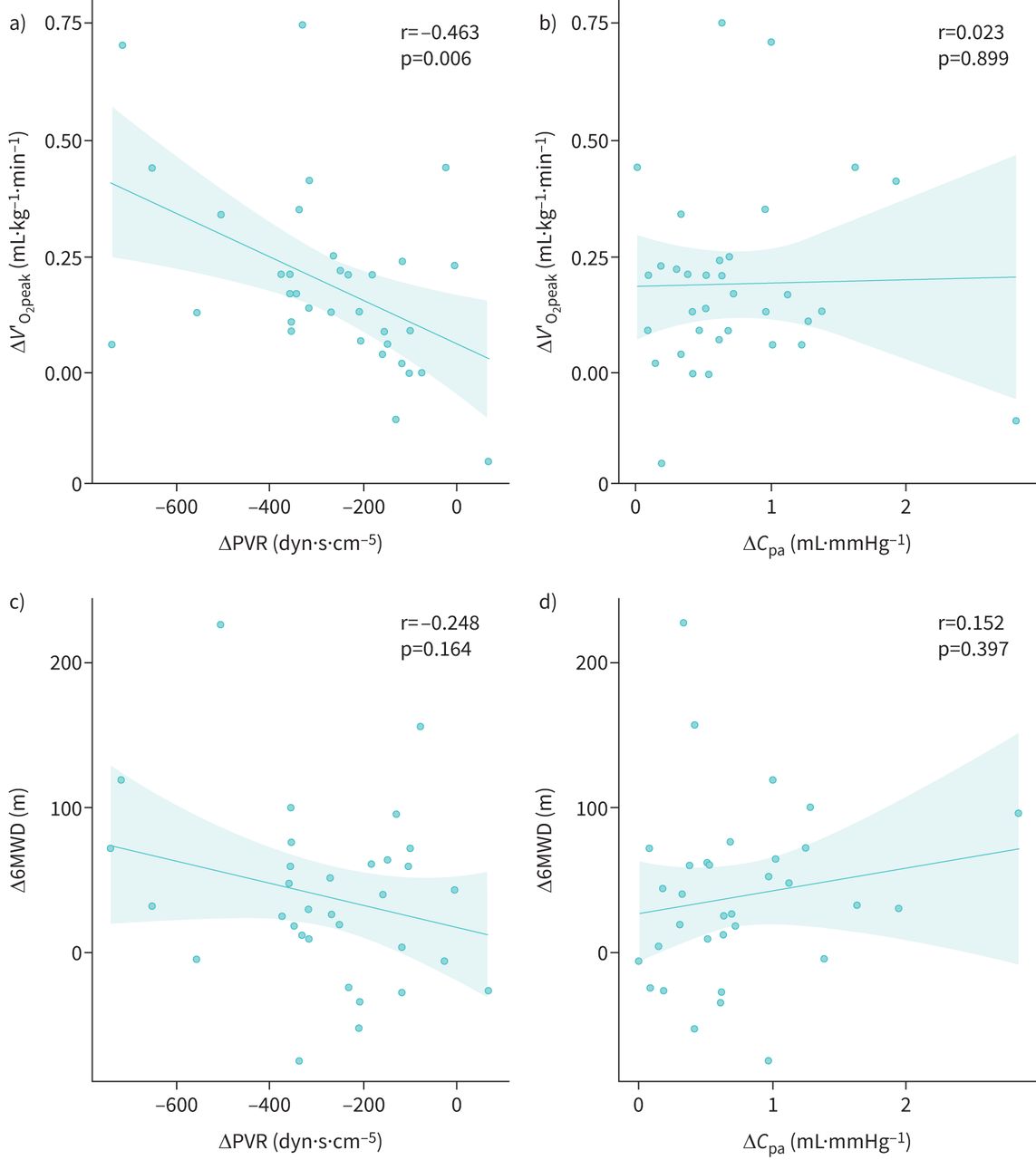
In univariate analysis, the only significant relationship was found between changes in peak V′O2 and changes in PVR (figure 2). The multivariate relationships between the two dependent exercise variables (peak V′O2 and 6MWD) adjusted for age, height, weight and gender on the one hand, and PVR and Cpa as independent variables on the other, are shown in table 3. Changes in peak V′O2 and in 6MWD both had a significant relationship with changes in PVR, but changes in exercise capacity did not have any significant relationship with changes in Cpa.
{kind=link}
{kind=link}
Correlations between the changes of the two physiological parameters used to quantify exercise capacity: a, b) peak oxygen consumption (V′O2) and c, d) 6-min walk distance (6MWD) and the changes (Δ) in a, c) pulmonary vascular resistance (PVR) and b, d) pulmonary artery compliance (Cpa) in chronic thromboembolic pulmonary hypertension patients before and after balloon pulmonary angioplasty.
Relationships between changes in peak oxygen consumption (V′O2) and in 6-min walk distance (6MWD) as dependent variables, and changes in pulmonary vascular resistance (PVR) and pulmonary artery compliance (Cpa; calculated according to the pulse-pressure method)
Similar results were found when Cpa was replaced by the SV/PP ratio (data not shown).
Discussion
In this study, we report that in CTEPH patients who have undergone BPA, changes in exercise capacity assessed either by peak oxygen consumption (V′O2) or 6MWD were significantly associated with changes in resting PVR, but not with changes in Cpa. In addition, in these patients, PVR significantly decreased and Cpa significantly increased, but the PVR×Cpa product (RC-time) did not change.
The association between improvements in pulmonary resistance and improvements in exercise capacity in CTEPH patients receiving BPA has been sparsely studied, and results depend on the test used to quantify exercise capacity [6]. In a group of 25 patients receiving BPA, Fukui et al. [18] reported that changes in peak V′O2 (but not changes in 6MWD) significantly correlated with changes in total pulmonary resistance. Kikuchi et al. [19] found that peak V′O2 was negatively correlated with the mPAP–CO slope (measured during exercise testing) in a large group of 249 CTEPH patients receiving BPA. Umemoto et al. [20] failed to find a significant correlation between changes in PVR and changes in 6MWD in a group of 70 CTEPH patients receiving BPA. In accordance with all these findings, before adjustment for age, gender, height and weight, we found a significant relationship between improvement in PVR and improvement in peak V′O2, but not between improvement in PVR and improvement in 6MWD. This suggests that relationships between changes in exercise capacity and changes in haemodynamic parameters depend at least in part on the test used to quantify exercise capacity [6, 21].
In our study, we did not find any significant association (either in univariate or in multivariate analyses) between changes in Cpa (and in SV/PP ratio) and changes in exercise capacity measured either with peak V′O2 or with 6MWD. Our results are consistent with the recent study by Umemoto et al. [20] in which the correlation coefficient between improvement in 6MWD and changes in Cpa was only 0.14 (p=0.26) in CTEPH patients who had not received any BPA at baseline. In this latter study, changes in Cpa were however significantly and positively correlated with changes in 6MWD only in the very particular subgroup of CTEPH patients who had achieved a mPAP <30 mmHg after having been treated previously with BPA and who underwent additional BPA procedures [20]. This suggests that the relationship between changes in exercise capacity and changes in Cpa (and PVR) are likely to be due, at least in part, to patients’ haemodynamic characteristics. Indeed, as the PVR and Cpa product is constant (see later), the relationship between PVR and Cpa is hyperbolic. Therefore, patients with low baseline PVR are likely to have higher relative changes in Cpa than those with high baseline PVR.
In a study involving 26 patients, Akaslan et al. [22] reported that the percentage change in Cpa after BPA accounted for 22% of the explained variability in the change in 6MWD after BPA [22]. Nevertheless, it should be noted that the pre- and post-BPA characteristics of these 26 patients were rather unusual, as improvement in 6MWD was major (median values from 320 to 450 m) despite a rather modest and incomplete haemodynamic improvement (mPAP: from 47 to 37 mmHg; PVR: from 739 to 408 dyn·s·cm−5).
In CTEPH patients, the finding of a stable RC-time after BPA, which has already been observed by others [20, 23], differs from findings established after PEA [10]. Indeed, after PEA, RC-time has been shown to decrease, suggesting that the drop in PVR was not accompanied by a “proportional” increase in Cpa. One possible explanation for the differences between patients undergoing BPA and PEA in terms of RC-time could arise from structural changes in the pulmonary artery wall that occur after PEA and not after BPA [24].
It has been shown in pigs and dogs that Cpa determined using the pulse-pressure method applied to a two-element windkessel model was the best approximation of true Cpa, both at baseline and after pulmonary embolisation [12]; conversely, Cpa determined using a three-element windkessel model (i.e. including characteristic impedance) and SV/PP both overestimated true compliance [12]. As Cpa determined using the pulse-pressure method has been shown to correlate well with SV/PP [12], we chose to estimate true Cpa using the following equation: Cpa=((SV/PP)/1.76+0.1).
Reported RC-times in the literature have consistently demonstrated significant scatter around the mean, suggesting that it is not appropriate to state that Cpa can always been calculated from PVR (and vice versa) [9]. In our study, we found rather low standard deviations of RC-time, with coefficient of variation (100×sd/mean) of 21% before BPA and 25% after BPA, which are among the lowest of those previously reported in CTEPH [9, 10]. In addition, we calculated values of RC-time that were up to two-fold lower than values reported by others in CTEPH patients [20, 25]. Assuming that by definition, the RC-time represents the time necessary for pressure to decrease in value to ∼37% from pulmonary arterial notch pressure to end-diastolic pulmonary arterial pressure, theoretically it takes three RC-times to complete 95% of this pressure change [9]. Therefore, the values of RC-time found in our study, resulting in estimated diastolic time of ∼1 s, are physiologically realistic.
Our study has several strengths. Firstly, we did not include patients with cofounding factors with respect to exercise capacity such as left heart failure, chronic airway obstruction or interstitial lung disease. Secondly, we studied V′O2 as a rough value after adjustment for selected confounding factors (age, height, weight and gender) and not as a percentage of a predicted value. We believe it is a strength because predicted values for peak V′O2 are poorly reliable for older people, i.e. for the age of our studied population [17]. In addition, these factors (age, height, weight and gender) are also recognised to be independently associated with Cpa [26].
Limitations exist in our study. It is a monocentric study involving a small population. Moreover, Cpa is only an estimation of the true compliance, especially because the dynamic nature of the pulsatile pulmonary arterial flow may induce a nonuniformly distributed compliance [26]. It is possible that other methods that take into account the characteristic impedance of the proximal pulmonary artery, such as the “energy balance method”, may be more appropriate [27].
Conclusion
Our report shows that contrary to what has been reported in CTEPH patients receiving PEA, improvements in PVR, but not in Cpa, are associated with improvements in exercise capacity in CTEPH patients receiving BPA. As our patients are representative of CTEPH patients receiving BPA in centres with recognised experience of BPA [3], our results suggest that improvement in PVR should remain a therapeutic goal in most CTEPH patients receiving BPA. Nevertheless, it remains to be determined whether Cpa should be a relevant end-point in CTEPH patients with near-normal baseline haemodynamic parameters and/or in patients with chronic thromboembolic disease without resting pulmonary hypertension.
Acknowledgement
The authors thank the staff of the department of cardiology (Centre Hospitalier Universitaire Grenoble Alpes, Grenoble, France) for their help in conducting this study.
Footnotes
Provenance: Submitted article, peer reviewed.
Ethics statement: This study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki and was approved by the French ethics committee CPP Sud-Est V (2013-AO1036-39). All patients gave written informed consent.
Author contributions: B. Degano made substantial contributions to the conception and design of the work. B. Degano, H. Bouvaist and N. Piliero supervised the implementation of the study. R. Sermet, N. Piliero, S. Madoun, F. Thony, E. Vautrin, H. Bouvaist and B. Degano carried out the evaluations. A. Guillien and B. Degano made substantial contributions to the analysis. B. Degano wrote the article. H. Bouvaist and S. Doutreleau scientifically advised the study and revised the manuscript. All authors approved the final version to be published and agreed to be accountable for all aspects of the work.
Conflict of interest: The authors do not have any conflict of interest to declare relative to the present study. The results of the present study are presented clearly, honestly, and without fabrication, falsification or inappropriate data manipulation.
- Received September 1, 2022.
- Accepted November 27, 2022.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










