





Abstract
Background Hiatal hernia may coexist with gastro-oesophageal reflux (GOR)-related chronic cough. This study aimed to evaluate whether the presence of hiatal hernia was related to chronic cough severity and the response to antireflux therapy.
Methods This was a retrospective analysis of data on adults with GOR-related chronic cough managed in our cough centre between 2017 and 2021. Patients who had undergone chest computed tomography (CT) and in whom follow-up data were available were included. The presence and size of hiatal hernia were assessed based on thorax CT scanning. Patients were treated with modification of diet and proton pump inhibitors. The response to treatment was assessed by the change in quality of life (QOL) measured by Leicester Cough Questionnaire (LCQ) and cough severity was measured by 100-mm visual analogue scale.
Results 45 adults (28 female, 17 male) were included. Hiatal hernia was demonstrated in 12 (26.6%) patients. Patients with hiatal hernia did not differ from those without hiatal hernia in clinical characteristics, cough duration and severity and cough-related QOL. We found moderate positive correlations between maximal sagittal diameter of hiatal hernia and cough severity (ρ=0.692, p=0.013) and duration (ρ=0.720, p=0.008). Patients without hiatal hernia responded better to antireflux therapy, with significant LCQ improvement. A strong negative correlation between sagittal diameter of hiatal hernia gate and increase in LCQ (ρ= −0.764, p=0.004) was demonstrated.
Conclusion The presence of hiatal hernia identified in chest CT may impact cough severity, duration and response to antireflux treatment in patients with GOR-related chronic cough. Further prospective studies are justified to confirm significance of hiatal hernia in the management of chronic cough.
Abstract
Assessing presence and size of hiatal hernia on chest CT may help in management of adults with gastro-oesophageal reflux-related chronic cough, as it may relate to worse response to antacid treatment, and impact the severity and duration of chronic cough https://bit.ly/3DlquFx
Introduction
Gastro-oesophageal reflux (GOR) is regarded as the third most common cause of chronic cough in adults, following asthma and upper airway disorders [1–3]. The prevalence of GOR-related chronic cough ranges from 1.4% to 85.4%, with lower values reported in Asia and higher in Europe and North America [1]. The diagnosis of GOR-related chronic cough is usually based either on the coexistence of chronic cough and typical symptoms of GOR such as heartburn, regurgitation and belching, or on evidence for GOR in imaging studies and oesophageal function tests (oesophageal pH-monitoring with/without impedance and oesophageal manometry, barium swallow test or endoscopy) and alleviation of cough after antireflux therapy in a patient with chronic cough [1–4]. According to the first American College of Chest Physicians guidelines, GOR-related chronic cough may be highly suspected in the proper clinical context after exclusion of other potential causes of chronic cough [2, 5]. The therapeutic approach to GOR-related chronic cough is similar to that recommended in gastro-oesophageal reflux disease (GORD) with predominating oesophageal symptoms, and usually commences with diet modification, promotion of weight loss in obese and overweight patients, avoiding meals within 3 h before bedtime and bed elevation during rest and sleep [5]. The next treatment step in patients with typical GORD symptoms includes antacid therapy with proton pump inhibitors (PPI), H2 antagonists or alginate for at least 8–12 weeks [5]. If response to treatment is unsatisfactory, prokinetic drugs may be considered. In contrast, PPI therapy is not recommended in patients with chronic cough and suspicion of GOR who have no heartburn or regurgitation [4, 6, 7]. Antireflux surgery may be considered in highly selected symptomatic patients with confirmed acid GOR-related chronic cough, inadequate response to ≥3 months of antireflux therapy and exclusion of oesophageal dysmotility. Importantly, the risk of surgery-related complication is not negligible [7, 8]. Despite various treatment modalities, one randomised controlled trial revealed that the result of causal treatment in GOR-related chronic cough is highly unsatisfactory and leads to significant cough reduction in only in 12.5–35.8% of patients [9].
GOR is a consequence of increased relaxation of the lower oesophageal sphincter (LOS). Hiatal hernia may be a predisposing factor for GOR, as it leads to a separation of LOS and the crural diaphragm, thus decreasing their ability to cooperate as a barrier to reflux events [10, 11]. Sliding hiatal hernia >2 cm in size is considered to be a clinically important mechanism for GOR [5, 12].
The barium swallow test and oesophagoscopy have been the classic methods for hiatal hernia diagnosis, but thoracic and abdominal computed tomography (CT) is also considered a reliable tool for the diagnosis and evaluation of hiatal hernia [11]. Hiatal hernias are identified on noncontrast CT of the chest as a proximal displacement of the oesophagogastric junction of the diaphragm into the mediastinum through the oesophageal hiatus. Besides documenting the presence of hiatal hernia, there has been an emerging interest in the measurements of hiatus size, as it may have clinical implications in patients who require fundoplication surgery [11, 13].
As hiatal hernia is not a rare finding in thoracic CT, this study aimed to analyse whether the presence of hiatal hernia in thorax CT was related to more severe cough and worse response to antireflux therapy in adults with GOR-related chronic cough treated in our cough centre.
The study protocol was approved by the institutional review board of the Medical University of Warsaw (Warsaw, Poland; KB/101/2009) as a part of a larger project on the efficacy of chronic cough management. All patients signed an informed consent form to analyse results of their diagnostic tests and management for research purposes. The research was conducted according to the principles of the World Medical Association Declaration of Helsinki.
Methods
General study design
This study was designed as a retrospective analysis of data on selected adults with chronic cough and GOR managed in the cough centre of the Department of Internal Medicine, Pulmonary Diseases and Allergy, Medical University of Warsaw between 2017 and 2021.
Patients and definitions
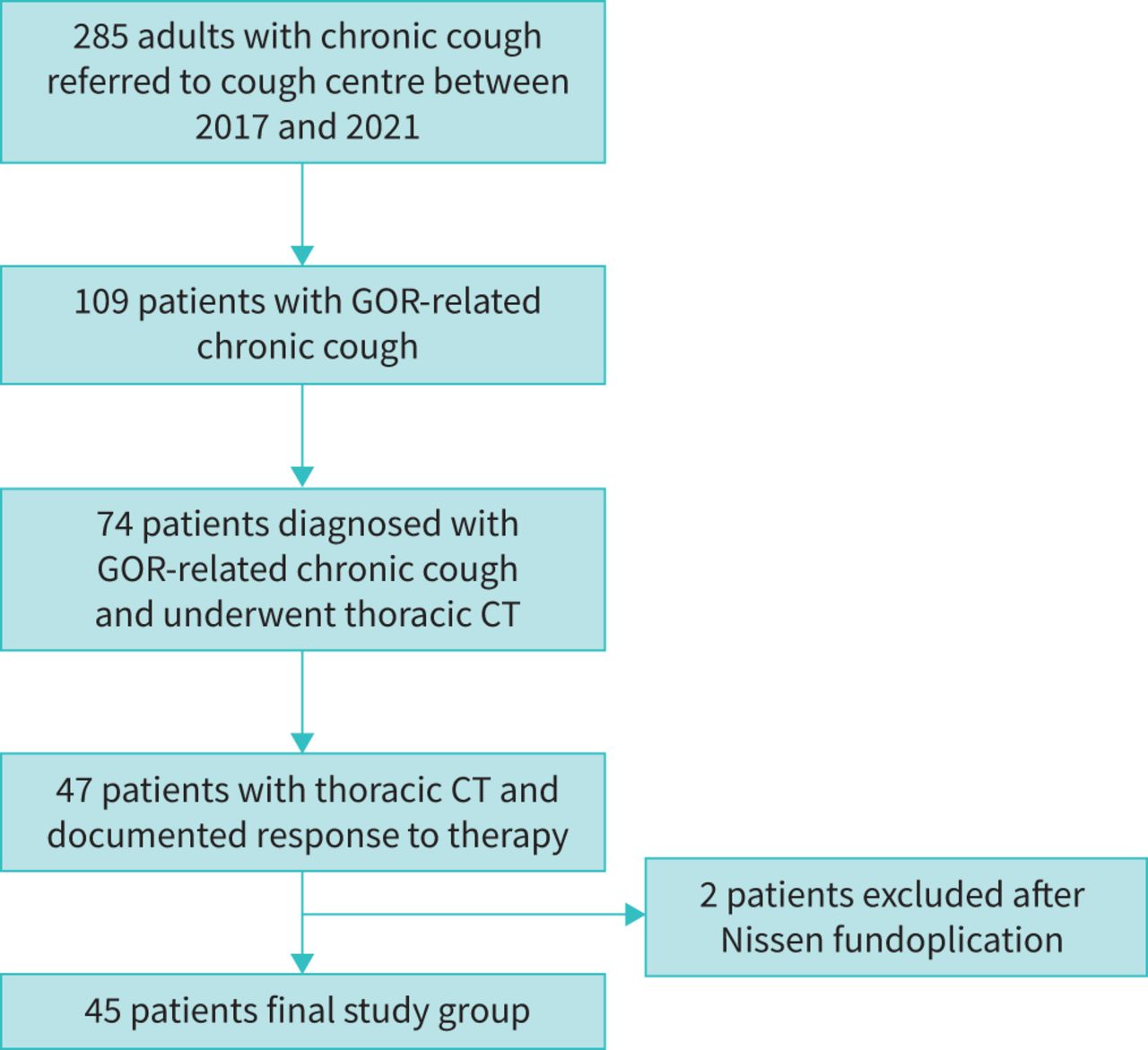
Chronic cough was defined as cough lasting for >8 weeks. The study included patients with chronic cough and GOR, in whom thoracic CT was performed as an element of integrative chronic cough diagnosis work-up and the response to antireflux treatment was documented (figure 1). Patients with other coexisting causes of cough were also included; surgical treatment for GOR was an exclusion criterion.

Flow chart presenting patient selection for the study. GOR: gastro-oesophageal reflux; CT: computed tomography.
GOR was diagnosed in adults with chronic cough and either typical symptoms of GOR or the results of oesophageal impedance/pH-monitoring or gastroscopy suggesting GOR. Hiatal hernia was diagnosed based on the assessment of thorax CT scans. The initial treatment of GOR included modification of diet, lifestyle and PPI (either omeprazole 40 mg twice daily or pantoprazole 40 mg twice daily for 4–6 weeks). If the patient did not respond to the initial antireflux therapy, the treatment was enhanced by adding prokinetic drugs.
Cough severity and its impact on quality of life were measured using a 100-mm visual analogue scale and cough-related quality of life was assessed using the Leicester Cough Questionnaire (LCQ) [4, 14]. Response to GOR therapy was measured by comparison of cough severity and quality of life before and after 4–6 weeks of treatment. Improvement in LCQ of >1.3 points was used as the criterion to distinguish responders and nonresponders to therapy [14].
Thorax CT acquisition and assessment
All thorax CT scans were performed at peak inspiration using spiral mode of 64-row multidetector CT scanner (Optima CT660; GE HealthCare, Chicago, IL, USA). The CT data of patients with GOR-related chronic cough were analysed by one radiologist (J. Żuchowska) blinded to the details of patients’ clinical characteristics. Multiplanar reconstruction of each CT was performed using AW Server (GE HealthCare). Axial images of 1.25 mm thickness in the soft tissue algorithm were loaded into a standard multiplanar reformat package, showing images in three orthogonal planes (axial, coronal and sagittal). In the oblique sagittal reformatted reconstruction, an image through the oesophageal hiatus was identified. Small adjustments in angle and position were performed to maximally demonstrate the margins of the hiatus and hernia. At this level, the distance between anterior and posterior margins of the oesophageal hiatus (gate of the hernia; figure 2a) and maximal anterior and posterior dimension of the hernia sac (maximal sagittal dimension) were measured (figure 2b). The maximal hernia length (gastric folds extending above the diaphragm) was measured by drawing a perpendicular line up to the superior margin of the hernia (figure 2a). In the coronal oblique reformatted reconstruction, after adjustment to show maximal coronal dimensions of the oesophageal hiatus and hernia, the distance between right and left margins was measured (figure 3a and 3b) [11, 15–17].

Measurement of hiatal hernia in thoracic computed tomography (sagittal oblique reformatted reconstruction). a) Measurement of gate (maximal distance between anterior and posterior margins of the oesophageal hiatus) and length (gastric folds extending above the diaphragm) of hiatal hernia; b) measurement of maximal sagittal dimension of hiatal hernia (maximal anterior and posterior distance).

{kind=link}
{kind=link}
{kind=link}
Measurement of hiatal hernia in thoracic computed tomography (coronal reformatted reconstruction). a) Measurement of maximal coronal dimension (maximal distance between right and left margins) of hiatal hernia; b) measurement of gate of hernia (distance between right and left margins of the oesophageal hiatus).
Statistical analysis
Descriptive statistics (median and interquartile range (IQR)) were used to present patient demographics. Due to non-normal distribution of data, nonparametric tests were used for analysis. The differences between cough severity and quality of life before and after treatment were tested using the Wilcoxon test. Various characteristics of responders and nonresponders were compared using the Chi-squared test for categorical variables and the Mann–Whitney U-test for continuous variables. Spearman coefficient was used for correlation analysis. p<0.05 was considered statistically significant.
Results
GOR was diagnosed in 109 (38.2%) out of 285 adult patients referred to our cough centre due to chronic cough between 2017 and 2021. Among them, chest CT was performed in 74 patients as a component of routine diagnostic procedure. In 47 patients in this subgroup (29 female, 18 male), response to therapy was documented. Two patients who had undergone surgical treatment for hiatal hernia (laparoscopic Nissen fundoplication) were excluded. Thus, 45 patients were included in the final analysis (figure 1). Among them, GOR was diagnosed based on the presence of typical reflux symptoms (n=35), the results of 24-h impedance and pH monitoring (n=8) and on the results of endoscopy (n=2).
Hiatal hernia was demonstrated in thorax CT scans of 12 (26.6%) patients; sliding hiatal hernia (type I) being present in all cases. The median coronal and sagittal hiatus diameters were 21.5 mm and 20.5 mm, respectively. The median coronal and sagittal hernia diameters were 27.5 mm and 29.0 mm, respectively, and the median hernia length was 29.5 mm. Patients with GOR and hiatal hernia did not differ from other GOR patients in terms of clinical characteristics, cough severity or duration, cough-related quality of life or efficacy of antireflux treatment with modification of diet and PPI (table 1).
Comparison of chronic cough patients with and without hiatal hernia.
In both groups, antireflux therapy was associated with reduced cough severity, but only in patients without hiatal hernia was significant improvement in LCQ observed (table 2).
Detailed data on the response to therapy in patients with and without hiatal hernia
Among patients with chronic cough due to GOR and hiatal hernia, strong positive correlations between the maximal coronal diameter of hiatal hernia and baseline cough severity (ρ=0.692, p=0.0126) and baseline cough duration (ρ=0.720, p=0.008) were observed. Moreover, a strong negative correlation was found between the hiatus gate diameter and increase in LCQ following therapy with diet modification and PPIs (ρ= −0.737, p=0.009).
Discussion
The results of our study suggest that the presence of hiatal hernia may be related to worse response to antacid treatment in patients with GOR-related chronic cough, and that the size of hiatal hernia impacts the severity and duration of GOR-related chronic cough. According to our knowledge, there are very few studies concerning the impact of hiatal hernia on GOR-related chronic cough. Thus, this observation may be valuable in the context of limited efficacy of antireflux therapy in patients with GOR-related chronic cough, pointing to those patients who may benefit from more intense antireflux therapy.
Numerous earlier studies have demonstrated a relationship between the exposure of the distal part of the oesophagus to nonacidic or acidic content and the prevalence of chronic cough [18–21]. Initially, researchers postulated that cough might be initiated by oesophageal irritation by acidic refluxate; then, an airway reflux hypothesis was proposed, based on proximal reflux and microaspiration [22]. The airway reflux describes gaseous or liquid, weakly acidic or nonacidic refluxate, which ascends through the oesophagus to the upper airways, resulting in airway epithelium damage and stimulation of the cough reflex [22]. Oesophageal dysmotility is increasingly frequently recognised in chronic cough patients and it is regarded as an important contributor to the pathophysiology of airway reflux and cough hypersensitivity [4]. Hiatal hernia has been shown to be closely related to reflux symptoms, reflux oesophagitis, Barrett's oesophagus and oesophageal adenocarcinoma [12]. Higher prevalence of oesophageal dysmotility in patients with hiatal hernia compared to subjects without hiatal hernia has been described [23, 24]. The potential pathomechanism of oesophageal dysmotility is related to the decreased pressure of the gastro-oesophageal junction due to displacement of lower oesophageal sphincter and the diaphragmatic crura [25]. However, to our knowledge, the influence of hiatal hernia on chronic cough has not been widely assessed before. In study by Schlottmann et al. [26], patients with GOR and larger hiatal hernia presented with more frequent episodes of coughing and wheezing. Similarly, the results of our study documented positive correlations between maximal coronal diameter of hiatal hernia and cough severity and duration. However, the median hiatal hernia length in our study was 29.5 mm (IQR 25–32 mm), which suggests that the hiatal hernias detected in our investigated patients were rather small. Despite its small size, the presence of hiatal hernia may impact the severity and duration of chronic cough, as well as response to chronic cough treatment. The increasing use of thoracic CT in the diagnostic work-up of adults with difficult-to-treat chronic cough enables the assessment of the presence and size of hiatal hernia. In our recent study, hiatal hernia was the most common abnormality potentially related to cough found in thoracic CT in patients with no evident abnormality on plain chest radiography (eight (4.2%) out of 189) [27].
Although the efficacy of therapy with PPI in patients with chronic cough is regarded as low, we started treatment with diet modification and a short trial period of PPIs, as the majority of our patients presented typical reflux symptoms. We found that coexistence of hiatal hernia and GOR-related chronic cough may be associated with a worse outcome of such treatment. In an earlier study, Dickman et al. [28] also found that hiatal hernia was more common in patients who failed to respond to PPIs. Conversely, Xu et al. [29] documented that PPIs did not improve oesophageal dysmotility. As hiatal hernia may favour oesophageal dysmotility, we suppose that patients with hiatal hernia and chronic cough may benefit more from nonpharmacological methods and prokinetic drugs than PPIs. Recent guidelines emphasise different phenotypes and personalisation in the management of GOR, and may also refer to the presence of hiatal hernia [5, 30, 31]. If typical symptoms of GOR and known hiatal hernia coexist, nonpharmacological therapies (reduction of supine GOR by elevating the head of the bed and avoiding meals within 3 h of bedtime), alginates (to neutralise the acid pocket in hiatal hernia) and considering surgical treatment seem justified [30, 31]. We might assume that this also applies to the presence of hiatal hernia in patients with GOR-related chronic cough, but further prospective studies are necessary to demonstrate whether personalisation of GOR treatment leads to reduction of chronic cough.
In the diagnosis of hiatal hernia, upper gastrointestinal endoscopy, barium-swallow radiography and oesophageal manometry are gold-standard investigations [12]. However, thoracic CT may also be considered as the one of the additional tests in diagnosis and measurement of hiatal hernia [11, 32]. Studies have revealed presence of hiatal hernia in thoracic CT scans in 40–53% of patients with idiopathic pulmonary fibrosis (IPF) [17, 33], and 59% of patients with scleroderma and pulmonary fibrosis. Moreover, hiatal hernia was shown to be related to progression and mortality in IPF [17, 34]. Worse airway disease severity was also documented in patients with non-cystic fibrosis bronchiectasis with coexisting hiatal hernia [35].
The results of this study indicate that further research assessing the possible impact of hiatal hernia on chronic cough is justified.
We are aware of some limitations of our study. First, it was a retrospective study which included a limited number of patients burdened with risk of selection bias. Therefore, our results need to be verified in a larger prospective cohort study. Second, we only analysed patients with GOR-related chronic cough and hiatal hernia, so the significance of hiatal hernia in other patients with chronic cough needs further analysis. Third, we only analysed effectiveness of lifestyle and diet modification and antacid treatment, so further steps of antireflux therapies (prokinetic drugs, surgical treatment) still need precise evaluation. Furthermore, the analysis was performed in adults treated in our cough centre, where mainly patients with difficult-to-treat chronic cough are managed. Assessment of the treatment efficacy of GOR-related chronic cough was based on patient-related outcomes without objective measurements such as cough monitors, which are not routinely used in our cough centre. Finally, many of our patients with GOR-related chronic cough also had other causes of cough, which might have influenced treatment efficacy. Despite these limitations, we believe that this real-life observation gives arguments for detailed assessment of hiatal hernia in thoracic CT scans performed in patients with chronic cough and justifies further prospective studies on the significance of hiatal hernia in treatment of chronic cough.
In conclusion, analysis of presence and size of hiatal hernia in thoracic CT may be useful in patients with GOR-related chronic cough, as hiatal hernia might be related to longer, more severe GOR-related chronic cough and worse response to antacid treatment in these patients. Further prospective studies to confirm the findings of this study seem justified.
Acknowledgements
The authors would like to thank Marta Maskey-Warzęchowska (Medical University of Warsaw, Warsaw, Poland) for her editorial assistance and manuscript review.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: We declare that M. Dąbrowska has received fees from Merck for consultations and lectures on chronic cough, outside the submitted work. E.M. Grabczak has received honoraria for lectures on chronic cough from Merck and Polpharma, outside the submitted work. A. Rybka-Frączek has received fee from Polpharma for attendance of the ERS International Congress (2019), outside the submitted work. R. Krenke has received honoraria for lectures from Chiesi, AstraZeneca and Polpharma, outside the submitted work; Boehringer Ingelheim, Chiesi and AstraZeneca have covered his fee and travel expenses for ERS International Congresses (2018 and 2019) and ATS Conferences (2018 and 2019), outside the submitted work.
Conflict of interest: O. Truba, J. Żuchowska and K. Białek-Gosk declare no conflict of interest.
Conflict of interest: The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the study apart from those disclosed.
- Received December 2, 2022.
- Accepted January 24, 2023.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










