





Abstract
There is a need and further room to strengthen airway clearance among patients with bronchiectasis in the modern era of clinical management https://bit.ly/3V5h5by
Bronchiectasis is a chronic, structural lung disease characterised by chronic productive cough or breathlessness, or decreased exercise tolerance, which are associated with recurrent airway infections and inflammation [1]. According to the international guidelines [1–4], the goals of bronchiectasis treatment consist of controlling the symptoms, reducing the number of exacerbations and improving the quality of life. Of the existing therapeutic approaches, airway clearance techniques (ACTs) are the major nonpharmaceutical interventions that have been endorsed to facilitate the clearance of sputum, improve lung function and maintain exercise endurance [5]. There are various types of ACTs, including the active cycle of breathing techniques, postural drainage and oscillatory devices (such as Acapella and Lung Flute) [6].
To date, there has been a paucity of evidence regarding the efficacy and safety of ACTs in bronchiectasis. Some limitations remain in the existing trials; for instance, the low quality of evidence due to the lack of proper controls or small sample sizes [7]. While more randomised controlled trials are needed to improve the evidence for ACT, the latest international clinical guidelines have endorsed ACTs as the fundamental treatments in adults with bronchiectasis [1, 2, 4]. A key rationale for the recommendation is that ACTs are regarded as effective in helping patients to ameliorate their respiratory symptoms and improve quality of life, which has been well recognised by most specialist clinicians and patients. To better inform clinicians on the status quo and unmet needs, multiple surveys on ACTs have been conducted [8–12]. However, these studies have focused on cystic fibrosis [8, 12] and chronic respiratory diseases other than bronchiectasis [11].
In this issue of ERJ Open Research, McLeese et al. [13] analysed the status quo of ACTs by performing online surveys among patients with bronchiectasis (consistent with the outcome data in the Bronch-UK/EMBARC Registry) and physiotherapists. The authors evaluated the feasibility of collecting ACT practice data online, the association between patient-reported ACT practice data and the outcomes in the Bronch-UK/EMBARC Registry, and the factors affecting physiotherapists’ decisions on initiating ACTs. Through this survey, the authors attempted to explore a new, comprehensive strategy to evaluate the feasibility of evaluating ACT treatment outcomes in an in-line survey between patients and physiotherapists.
In the first round of a patient-oriented survey distributed to 398 patients with bronchiectasis who were recruited from the Bronch-UK/EMBARC Registry in Northern Ireland, UK, the questionnaire was completed by 205 (52%) individuals. Although 55% (113 out of 205) of patients who were able to complete the questionnaire independently online, many patients could only complete the survey via telephone or by mailing a paper version. In the second round, of the 96 survey questionnaires that were retrieved, 94% of patients (90 out of 96) self-administered the survey online. The physiotherapist-oriented survey was distributed to 100 physiotherapists, from whom 48 questionnaires were retrieved. All physiotherapists self-administered the questionnaires independently online. However, both the manner in which the questionnaires were distributed and the proportion of effective returns should be regarded as limitations of the study. To partly mitigate this, future research may consider deploying social communication software or questionnaire survey websites for better distribution of questionnaires and more efficient retrieval of the responses (e.g. via online apps).
Notably, the adherence to ACTs in the UK population appeared to be high. Upon completion of the first survey, 86% (177 out of 205) of patients still performed ACTs, and in the second survey, 78% (70 out of 90) of patients reported performing the same type of ACT, which was markedly higher than the adherence in the US Bronchiectasis and Non-tuberculous Mycobacteria Registry, in which only a quarter adhered to ACTs at the 1-year follow-up [14]. The current findings remained more reassuring when compared with the adherence (41% of patients continuously adopted ACTs) in Northern Ireland according to the statistics reported in another study [14].
A strength of the study design was that McLeese et al. [13] quantified the dose of ACTs into three grades: low, medium and high dose. Patients performing ACTs (particularly high-dose ACTs) were more elderly and had more severe bronchiectasis (evidenced by the greater frequency of exacerbations in the previous year and lower quality of life). Moreover, younger patients were more likely to use mucoactives to aid in expectoration. These findings might be explained by the differences in clinical experience with ACT practices: patients would perform ACTs for symptomatic relief rather than for prophylactic use. The preference of physiotherapists for administering and instructing patients might also play a role in shaping the performance of ACTs.
In the current survey, 68% (140 out of 205) of patients reported that the initial ACT practice was guided by a physiotherapist during an outpatient visit and that most patients thought that visiting a physiotherapist specialising in bronchiectasis management would be crucial for guiding their initial use of ACTs. Besides, the active cycle of breathing technique (64%, 129 out of 201 patients) was the most commonly reported ACT manoeuvre, followed by huffing (41%), and exercise and/or physical activity (38%), which differed from the findings of the US Bronchiectasis and Non-tuberculous Mycobacteria Registry and an Australian ACT study among patients with cystic fibrosis [12, 14]. The use of ACT might vary globally depending on the culture and the patient's preference, and there is currently no high-quality evidence that is directly driven from head-to-head comparisons of different ACT manoeuvres [7, 16].
The current study also conducted a survey among physiotherapist to better understand their perspective on ACT therapy. Physiotherapist rated the patient's symptoms as the most important factor affecting the choice of ACT, followed by the stability of the patient's clinical status. Both patients and physiotherapists addressed the importance of the receipt of ACTs under professional guidance, which is consistent with the recommendations in the published guidelines [1–4]. Previously, most published studies have not systematically assessed the quality and effectiveness of ACT treatment. Meanwhile, the prescription of ACTs could be influenced by personal experience, healthcare resources, the time available and the cost-effectiveness of these interventions [11, 17]. Hence, the current survey provides greater insights into promoting the application of ACTs and maximising their clinical benefits.
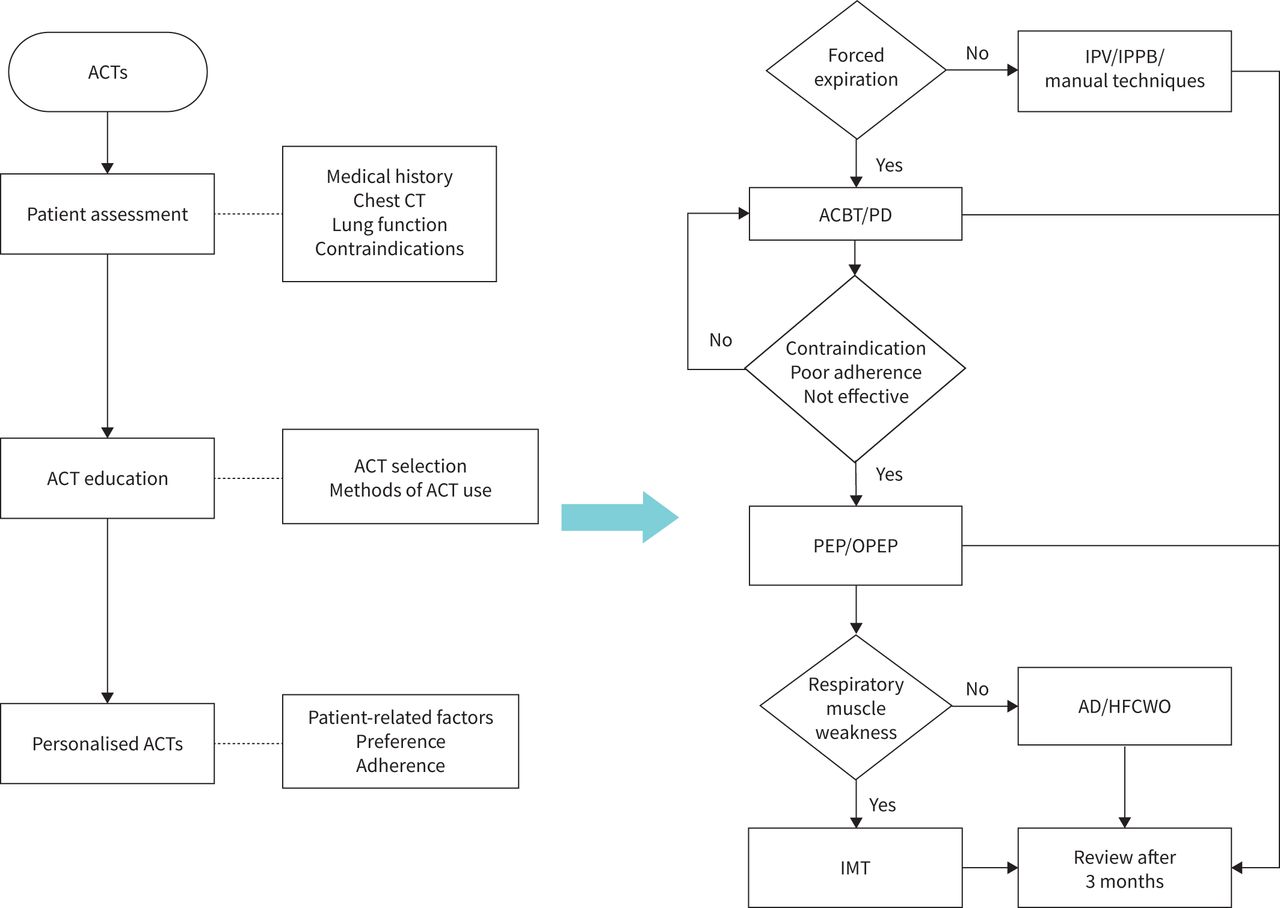
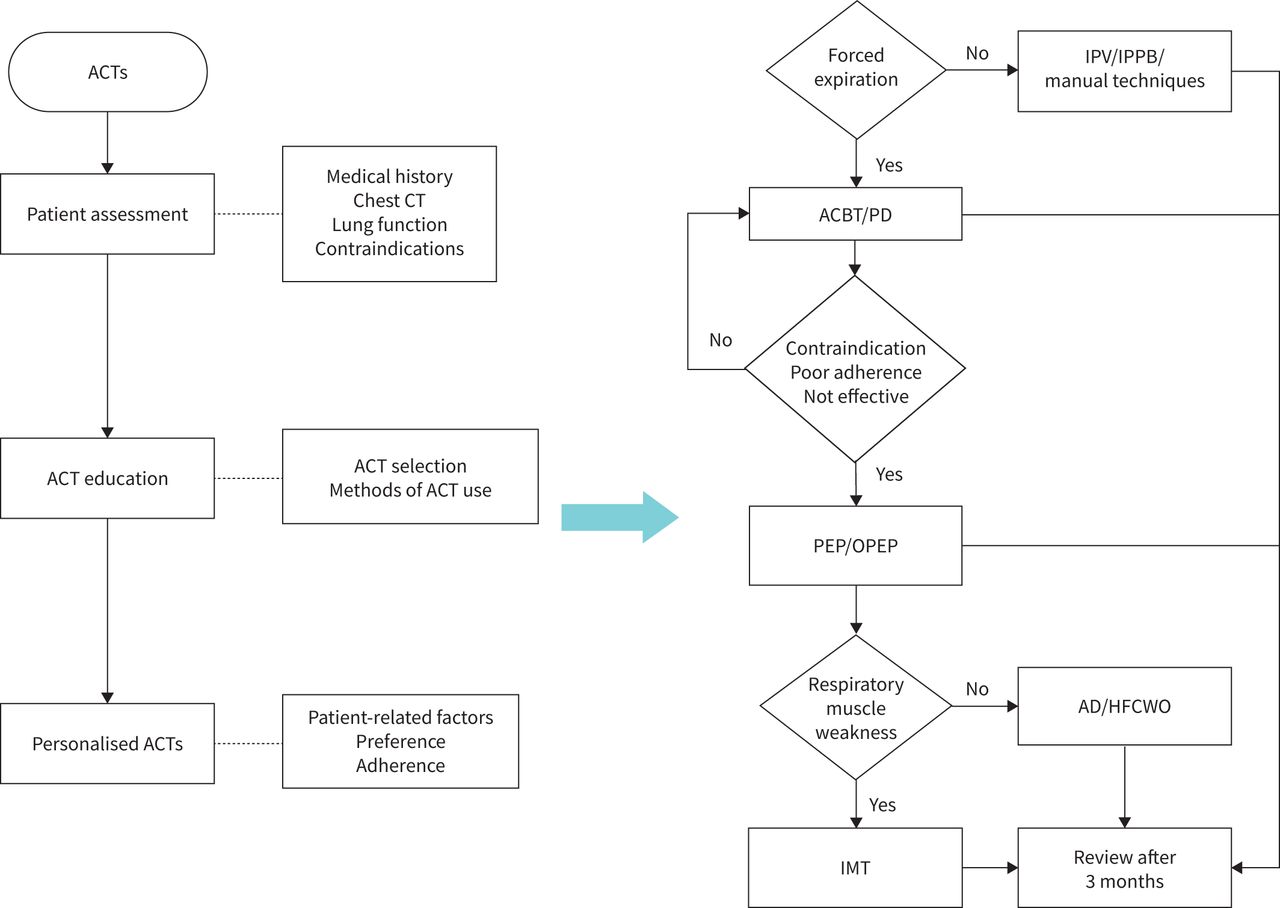
It is important to monitor the procedures of ACT management despite the lack of sufficient evidence. Prescription of ACTs should include careful patient assessment, protocol development, ACT execution and outcome review. Patient assessment consists of the fundamental clinical status appraisal (sputum volume or consistency, exacerbation frequency, quality of life, disease severity and the underlying aetiology, etc.), the radiological and laboratory test findings (chest computed tomography, pulmonary function, diaphragmatic muscle strength, etc.), and the assessment of contraindications [1, 2, 18]. Protocol development may facilitate the personalised decisions of selecting the preferred ACT manoeuvres based on the patient's clinical assessment. Patients need to be made aware of the spectrum of ACTs. Factors such as the patient's workload, financial burden, access to resources, preferences and adherence should also be taken into account when making the decisions [1–3, 17]. The treatment protocols should be continuously optimised and figure 1 outlines the recommended work flow for standardising ACT management in clinical practice among patients with bronchiectasis. The efficacy of airway clearance therapy should be assessed every 3 months. Although there remain some limitations within the current measures of efficacy, the most common measures include 24-h sputum volume, lung function and pulse oximetry. Common patient-centred outcomes in the literature included the health- and cough-related quality of life and dyspnoea metrics (e.g. Leicester Cough Questionnaire, St George's Respriatory Questionnaire and Modified Medical Research Council dyspnoea scale). The usefulness of the “Quality of Life – Bronchiectasis” questionnaire (the first validated disease-specific questionnaire) and Bronchiectasis Health Questionnaire (another simpler disease-specific questionnaire) should be evaluated in future clinical trials of ACTs [19].
{kind=link}
Airway clearance technique (ACT) management flow chart. Chest computed tomography (CT) is the gold standard for identifying the affected lobes or segments to inform appropriate postural drainage. IPV: intrapulmonary percussive ventilation; IPPB: intermittent positive pressure breathing; manual techniques: comprised of percussion, shaking, vibrations and overpressure; ACBT: active cycle of breathing techniques; PD: postural drainage; PEP: positive expiratory pressure; OPEP: oscillating positive expiratory pressure; AD: autogenic drainage; HFCWO: high-frequency chest wall oscillation; IMT: inspiratory muscle training.
Future research should focus not only on the technology and equipment being adopted to boost the effectiveness of ACTs but also on patients' understanding of and adherence to ACTs. A core mission for physiotherapists is to establish a follow-up plan and provide expert guidance to better implement the ACTs. The study findings by McLeese et al. [13] have provided an important basis for researchers and clinicians to better understand the status quo and improve the outcome of ACT treatment in patients with bronchiectasis.
Footnotes
Provenance: Commissioned article, peer reviewed.
Author contributions: C-X. Pan, M-X. Shi and W-J. Guan drafted the manuscript, and W-J. Guan critically reviewed the manuscript. All authors have approved for the final submission.
Conflict of interest: W-J. Guan is an associate editor of this journal. All other authors declare no potential conflict of interest related to this paper
Support statement: This editorial was supported by the National Natural Science Foundation Outstanding Youth Fund (number 82222001), the National Natural Science Foundation grant 81870003, Zhongnanshan Medical Foundation of Guangdong Province grant ZNSA-2020013 (to W-J. Guan) and Guangzhou Science and Technology Plans (number 202102010372). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received December 5, 2022.
- Accepted December 6, 2022.
- Copyright ©The authors 2023
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










