





Abstract
Background Several studies demonstrated that Propionibacterium acnes (P. acnes) may be involved in sarcoidosis pathogenesis. Presence of P. acnes was found in granulomas of the majority of Japanese sarcoidosis patients. However, presence of P. acnes in tissue has never been related to sarcoidosis phenotypes and clinical outcome. Therefore, the aims of our study were to demonstrate whether P. acnes can be detected in granulomas of Dutch sarcoidosis patients and to investigate whether its presence is related to a clinical phenotype and/or course of disease.
Methods Sections of formalin fixed paraffin-embedded tissue blocks of 76 sarcoidosis patients were examined by immunostaining with a P. acnes-specific monoclonal antibody (PAB antibody) using a VENTANA BenchMark ULTRA. Clinical outcome status (COS) was determined and classified into two phenotype groups: A: resolved, minimal or persistent disease without treatment (COS 1–6) and B: persistent disease with need for treatment (COS 7–9).
Results P. acnes was detected in samples of 31 patients (41%) and located within granulomas in samples of 13 patients (17%). The frequency of P. acnes detected in granulomas at diagnosis was significantly higher in patients with phenotype B compared to patients with phenotype A (29% versus 0%, p=0.021).
Conclusion Presence of P. acnes in granulomas can be confirmed in Dutch sarcoidosis patients. It is intriguing that presence of P. acnes in granulomas is more frequently found in patients with chronic disease requiring treatment. This adds to the rationale that a subgroup of sarcoidosis patients might benefit from antibiotic therapy.
Abstract
Significantly more sarcoidosis patients with a chronic disease course requiring treatment had presence of P. acnes in granulomas. This contributes to the premise that it is relevant to further explore antibacterial therapy in sarcoidosis.
Introduction
Sarcoidosis is a multisystem inflammatory disorder of unknown etiology that is characterised by the presence of non-caseating granulomas. In over 90% of patients the lungs are involved [1], but the disease can also affect other organs [2]. Patients with symptomatic organ involvement or risk of permanent damage can be treated with immunosuppressive drugs [3], which suppress disease activity but do not cure the disease.
The cause of sarcoidosis is still puzzling scientists for more than a century. Several studies demonstrated that specific microorganisms, including mycobacteria and Propionibacterium acnes (P. acnes) could be involved in its disease pathogenesis [4–9]. As P. acnes is a commensal, Koch's postulates cannot be applied, which makes it difficult to elucidate its etiologic role [10]. A higher number of P. acnes genomes have been found in tissue from Chinese, Japanese, Italian, English and German sarcoidosis patients compared to tissue of controls, suggesting involvement in disease pathogenesis [11–13]. Furthermore, an increased immune response to P. acnes among patients with sarcoidosis was found in different studies using Japanese or German patients [7, 8, 14]. Remarkably, in recent work from our own group, we found a lower percentage of Dutch sarcoidosis patients than controls with an immunological response to P. acnes [15] which is conflicting with the abovementioned previous papers.
In addition to its role as possible antigen, P. acnes can also act as a mitogen which is demonstrated by the fact that P. acnes enhances immunogenicity of certain vaccines [16] and enhances cytotoxic activity toward different tumor cells [17–19]. A potential mitogenic role of P. acnes in sarcoidosis has not previously been studied.
Based on both a possible antigenic as well as mitogenic role for P. acnes, we hypothesise that presence of P. acnes in tissue could be related to certain clinical phenotypes in sarcoidosis. We therefore examined the presence of P. acnes in tissue of Dutch patients with sarcoidosis using an existing P. acnes specific monoclonal antibody (PAB antibody) [20] and related results of immunostaining to clinical characteristics such as organ involvement and course of disease.
Methods and materials
Study patients
Unstained tissue blocks were requested from two sarcoidosis cohorts previously studied at the St Antonius Hospital (Nieuwegein, The Netherlands) [15, 21]. The diagnosis of sarcoidosis had been established according to the criteria of the American Thoracic Society/European Respiratory Society [22]. Patients were included in the study when enough residual tissue was available and when presence of granulomas could be clearly detected in the hematoxylin and eosin (H&E) stained tissue sections. The study was approved by the Medical research Ethics Committees United (MEC-U) of the St Antonius Hospital (R05-08A) and written consent was obtained from all patients.
Immunostaining
4 µM thick sections were cut from the formalin-fixed paraffin-embedded tissue sections which were immunohistochemically stained with the PAB antibody; a P. acnes specific monoclonal antibody that reacts with cell-membrane bound lipoteichoic acid of the bacterium [20]. The PAB antibody was kindly provided by Prof. dr. Eishi and colleagues, Department of Human Pathology, Tokyo Medical and Dental University, Tokyo, Japan. We followed the protocol described by Negi et al. [20], but instead of the original manual procedures the sections were stained by the use of a VENTANA BenchMark ULTRA (Ventana Medical Systems, Inc., Tucson, AZ, USA) using ultraView Universal Alkaline Phosphatase Red Detection Kit (Ventana Medical Systems, Inc.). We modified the original protocol to optimise the sensitivity and specificity of the staining results for the VENTANA BenchMark ULTRA. Shortly, sections were de-paraffinized and rehydrated followed by antigen retrieval using the hot plate heating system of the machine instead of antigen retrieval by microwave. Because mineral oil (Liquid Coverslip, Ventana Medical Systems, Inc.) covering the tissue slides was found to inhibit the reaction with PAB antibody, before the primary antibody reaction with the PAB antibody, a washing step (3 times for 5 min each) in the EZ Prep buffer (Roche Nederland B.V, Woerden) was added under the Antibody Titration program selected, followed by washing 5 min with tap water and 5 min with reaction buffer (Roche Nederland B.V, Woerden, The Netherlands). The PAB antibody (crude mouse ascites fluid) was used in a concentration of 1:30.000 (diluted with DAKO REAL antibody diluent, S2022, DAKO, Glostrup, Denmark) and incubated for 16 min at room temperature. Instead of using peroxidase substrate diaminobenzidine (DAB) to develop the signal, ultraView Universal Alkaline Phosphatase Red Detection Kit (Ventana Medical Systems, Inc.) was used. Sections were counterstained with Mayer's hematoxylin. Detection of P. acnes in tissue was analysed by a pulmonary pathologist (KS). The staining was considered positive when small round/dot like structures were seen. If such structures were detected, it was determined whether positive PAB staining was present in or outside the granulomas.
Identification of P. acnes related phenotypes
To determine possible P. acnes related phenotypes, organ involvement, age at diagnosis and Scadding stage at diagnosis and follow up was collected from medical records of sarcoidosis patients.
The Clinical outcome status (COS), a definition of clinical outcome in sarcoidosis established by The World Association of Sarcoidosis and Other Granulomatous disease (WASOG) [23],was determined 2 and 5 years after diagnosis. The disease status of patients was retrospectively examined and classified into resolved, minimal or persistent disease. Resolved was classified as patients showing no signs of disease anymore, so normalisation of chest x-ray, pulmonary function test, laboratory tests etc. Minimal disease is defined as a disease burden of 25% or less compared to the maximum disease burden experienced by patients measured by for example pulmonary function test, Chest X-ray, biomarkers and skin lesions. For example, the worst pulmonary function test had to be improved by at least 75% to be considered minimal disease.
Furthermore, it was examined whether patients were ever treated, and if so whether they were still using medication or not (defined as no medication>1 year). Patients in whom medication was increased the last year were considered worsening. Medication included all immunosuppressive systemic therapies used for sarcoidosis, including corticosteroids, DMARDS and anti-TNFα antibodies, except for non-steroid anti-inflammatory drugs. This results in 9 COS scores:
1: Resolved disease, never treated
2: Resolved diseases, no treatment>1 year
3: Minimal disease, never treated
4: Minimal disease, no therapy>1 year
5: Persistent disease, never treated
6: Persistent disease, no therapy>1 year
7: Persistent disease, current therapy but no worsening in prior year and asymptomatic
8: Persistent disease, current therapy but no worsening in prior year and symptomatic
9: persistent disease, current therapy which worsened in the prior year
Patients who died in the period over which the COS was determined were placed in COS 9.
To analyse whether there was a correlation between presence of P. acnes and COS, we classified the COS scores into two phenotype groups: A: resolved, minimal or persistent disease without treatment (COS 1–6) and B: persistent disease with need for treatment (COS 7–9).
Statistical analysis
Data was analysed using IBM SPSS statistics version 24. An unpaired t-test was used to compare numerical data. Non-parametric tests were used for non-normally distributed data (Mann-Whitney U test). Categorical data were compared using the Chi-squared test. If expected cell frequencies were below 5, Fisher's exact test was used for categorical data up to two categories. p-values <0.05 were considered significant.
Results
Characteristics of study patients and tissue samples
Formalin-fixed paraffin-embedded tissue blocks were available from 76 patients. Mean age of included patients was 44 years, 84% was Caucasian and 71% had extra pulmonary involvement. 68% and 67% were classified in phenotype group B 2 and 5 years after diagnosis respectively (table 1).
Characteristics of study patients
P. acnes can be detected in tissue samples of Dutch patient with sarcoidosis
Most tissue sections used for staining originated from the lung, followed by lymph node and skin samples. P. acnes was detected in tissue samples from 31 of the 76 sarcoidosis patients (41%) and was located in the granulomas in 13 samples of all patients (17%) (table 2, fig. 1 and 2). When P. acnes was not detected inside granulomas, it was mostly located directly adjacent to granulomas in histiocytes and in a few cases in granuloma-free areas of the tissue. Besides lung, lymph node and skin tissue, we also found presence of P. acnes in bone marrow and liver tissue. No significant difference was observed in the frequency of P. acnes detected in tissue or granulomas between the different organs used in the study (p=0.583 and p=0.490, respectively). P. acnes was detected in tissue or granulomas in 3 (43%) and 3 (43%) respectively, of the 7 lung samples obtained by video-assisted thoracic surgery (VATS), and in 7 (28%) and 4 (16%) respectively, of the lung samples obtained by transbronchial lung biopsy (TBLB). No significant difference in presence of P. acnes in tissue or granulomas was observed between the different biopsy methods used for the lung samples (p=0.648 and p=0.157, respectively) and lymph node samples (p=0.167 and p=0.588, respectively).
Detection of P. acnes and origin of tissue used




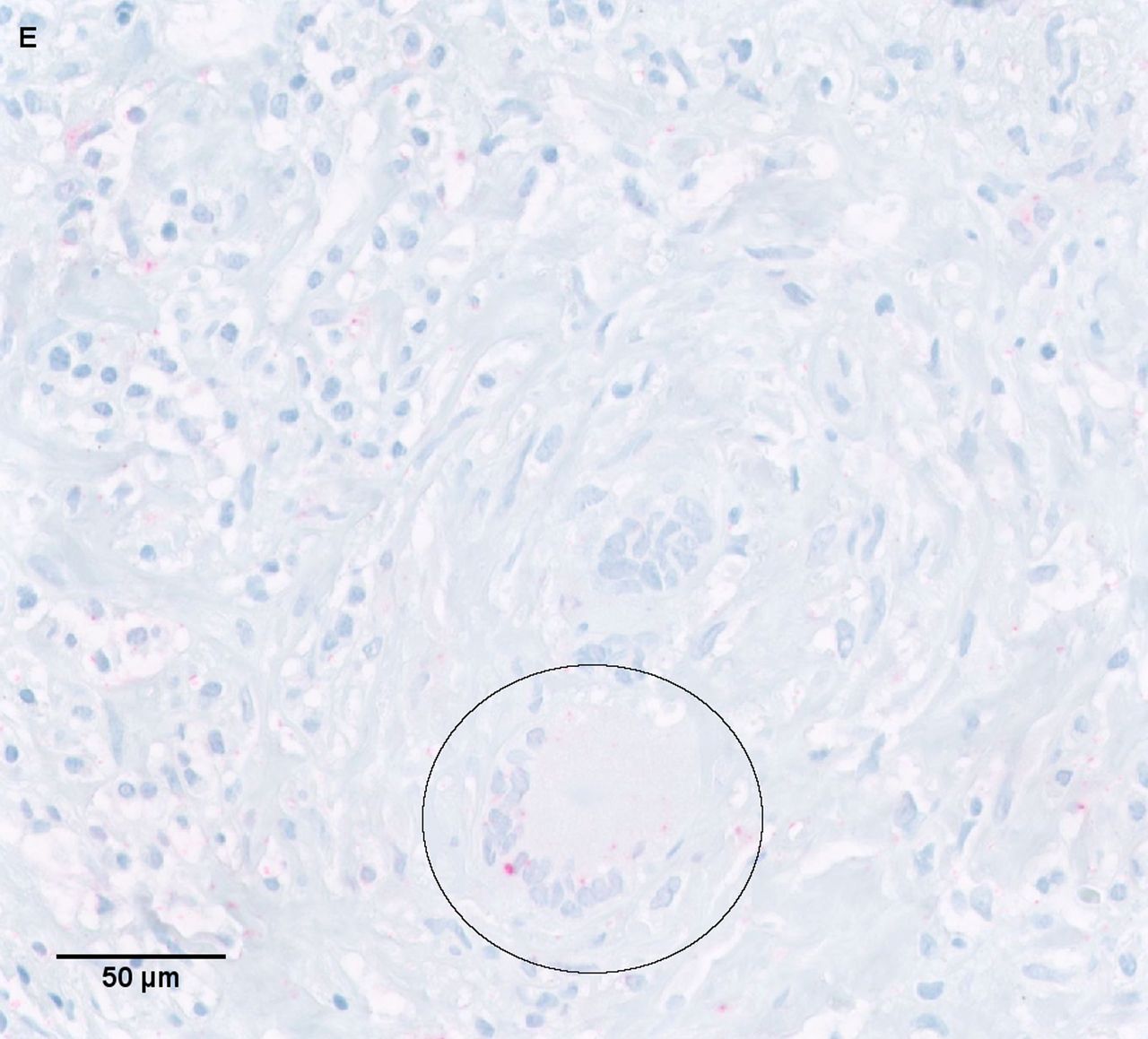
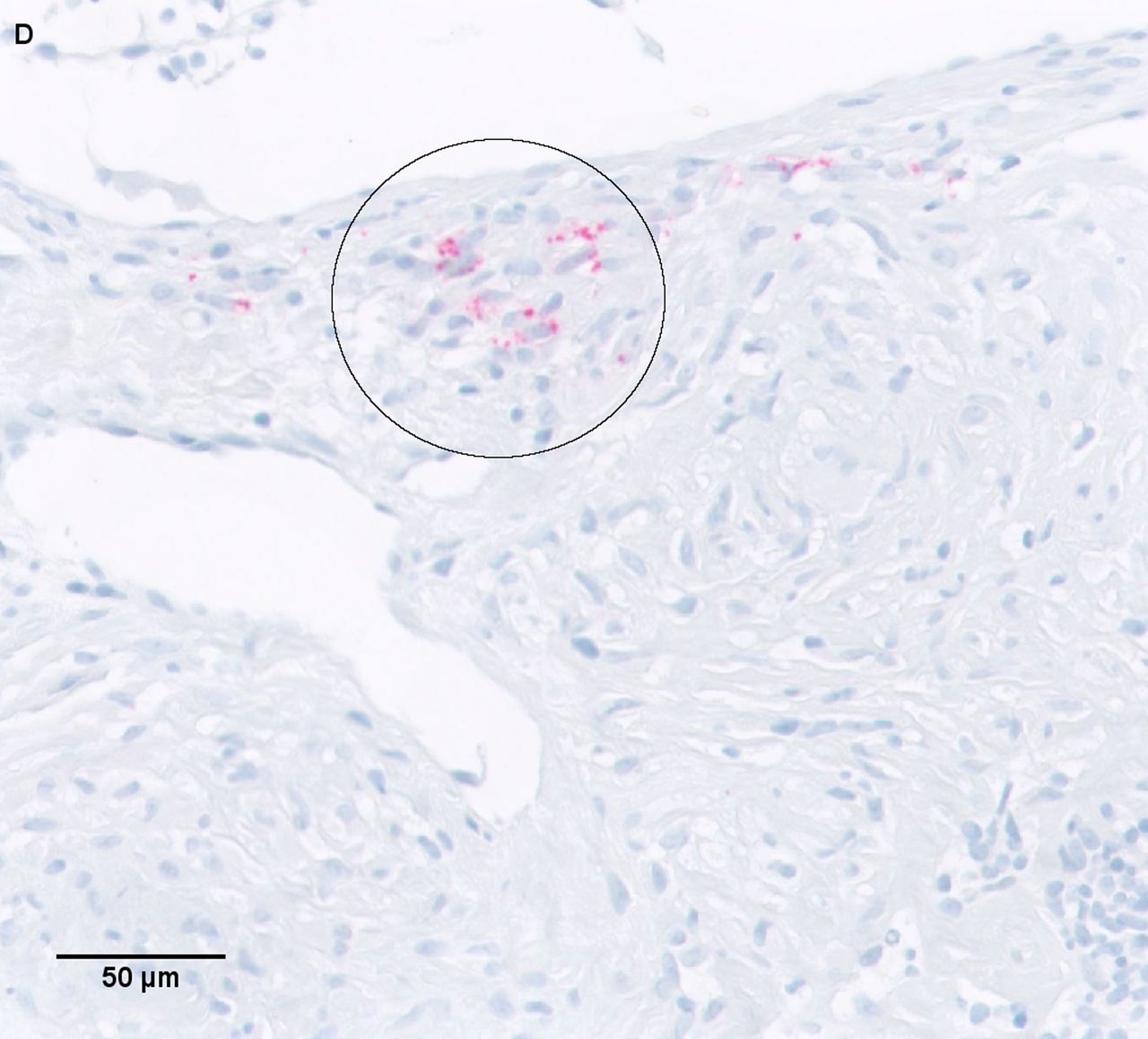
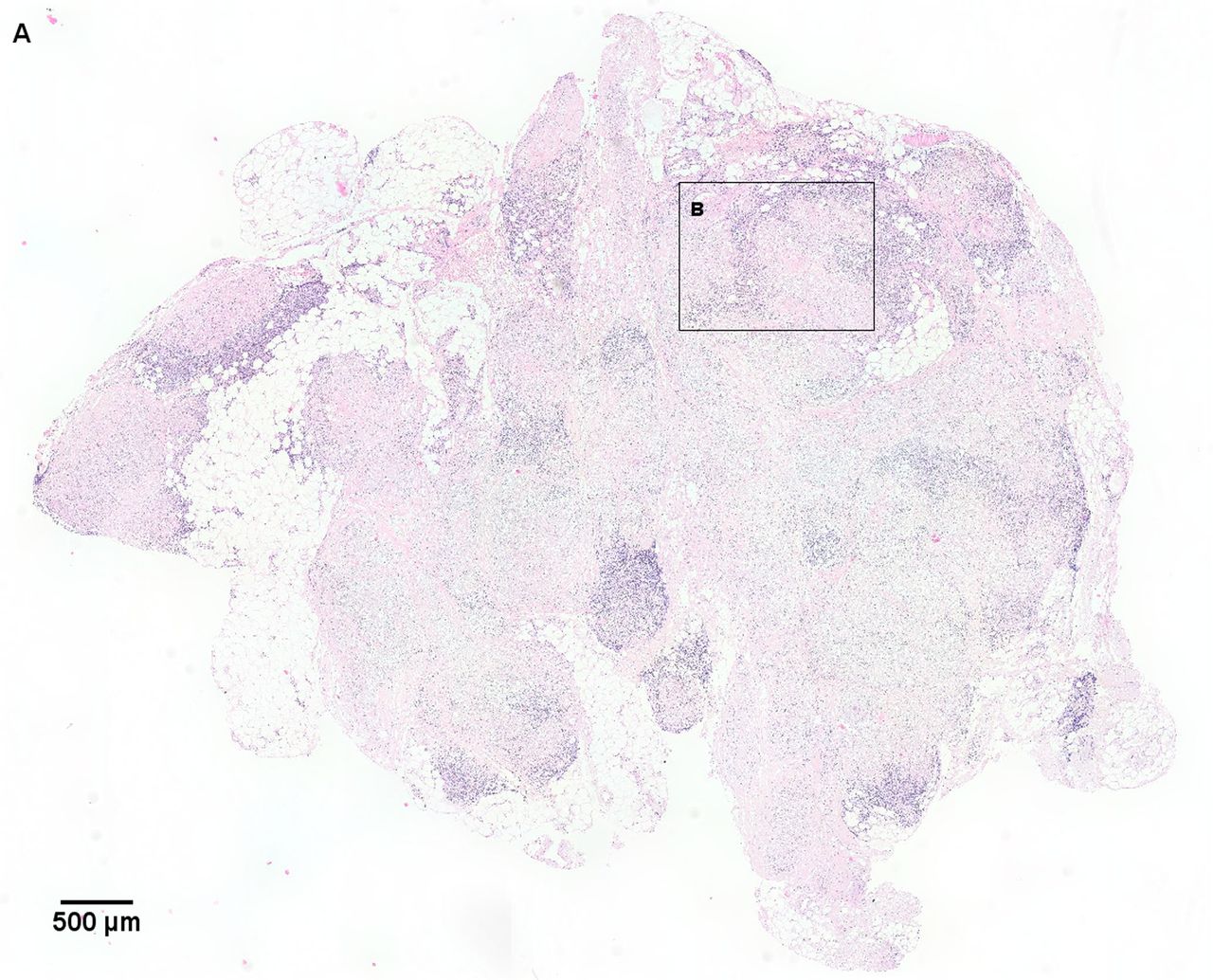
Presence of P. acnes in and around an immature granuloma of the lymph node a) Hematoxylin and eosin (H&E) staining of a needle lymph node biopsy including several mature granulomas. Arrow: a mature granuloma including a multinucleated giant cell (arrow head). Open arrow: an immature granuloma. b) PAB staining corresponding with the area in picture a, including several areas with P. acnes-positive red signals (rectangle c and d) and a mature granuloma negative for P. acnes (rectangle e). c) Higher magnification of positive P. acnes staining (circles) around granulomas. d) Higher magnification of positive P. acnes staining (circle) in an immature granuloma. e) Higher magnification of another area including a multinucleated giant cell positive for P. acnes.



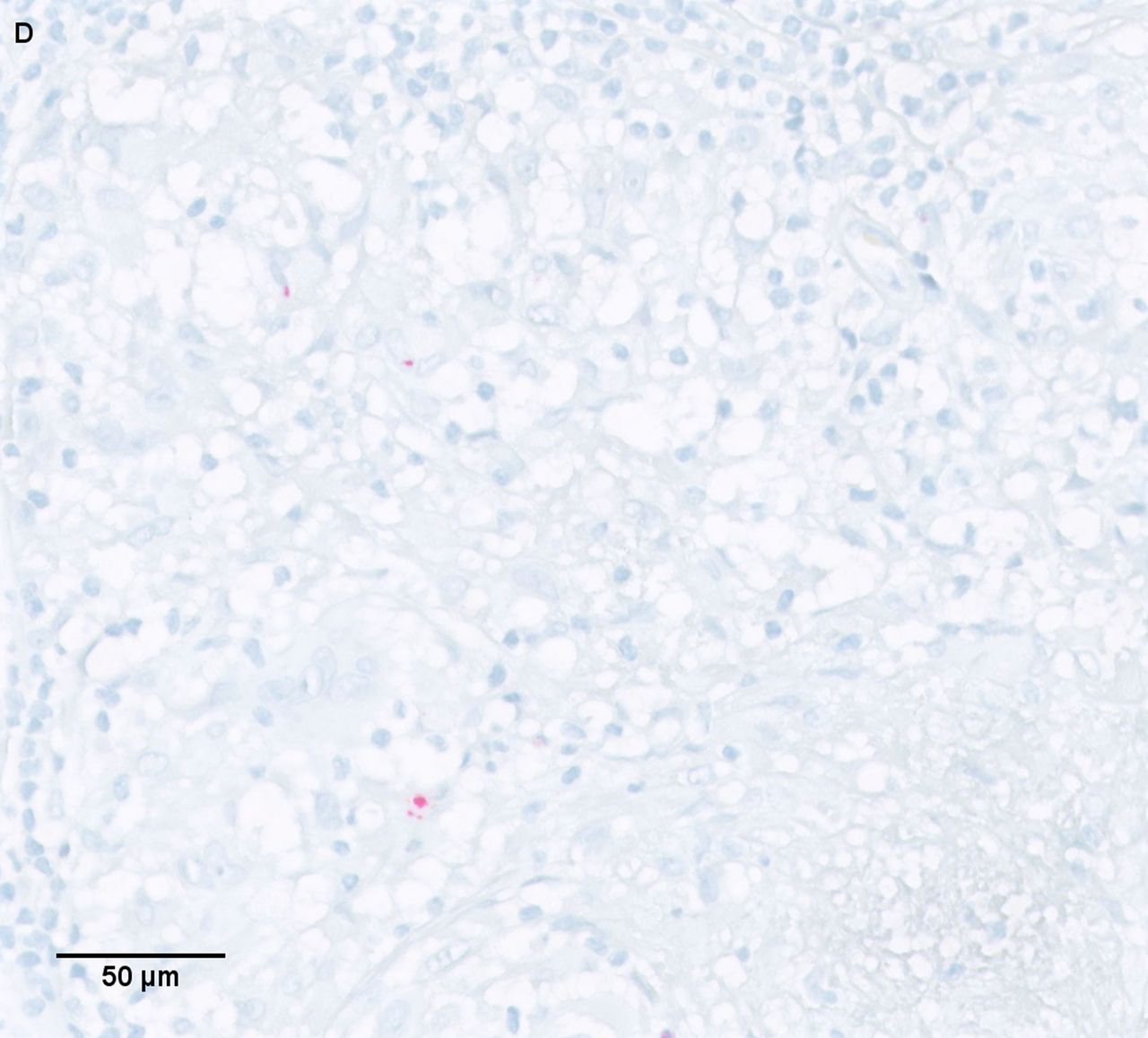
Presence of P. acnes in a mature granuloma in subcutaneous tissue of the lower eyelid. a) Overview of hematoxylin and eosin (H&E) staining of subcutaneous tissue of the lower eyelid. b) Higher magnification of area b from picture a, including mature granulomas (arrows) and multinucleated giant cells (arrow head). c) PAB staining of corresponding area of picture B, including several areas of P. acnes-positive signals (circles and rectangle d), in mature granulomas. d) Higher magnification of area d from picture c, with positive P. acnes staining in a mature granuloma.
Presence of P. acnes does not correlate with organ involvement
When relating positive P. acnes staining results to clinical characteristics, no relation with age, sex, ethnicity, organ involvement or Scadding stage was observed (table 3).
Presence of P.acnes in tissue and granulomas related to organ involvement and Scadding stage
Presence of P. acnes correlates with clinical outcome
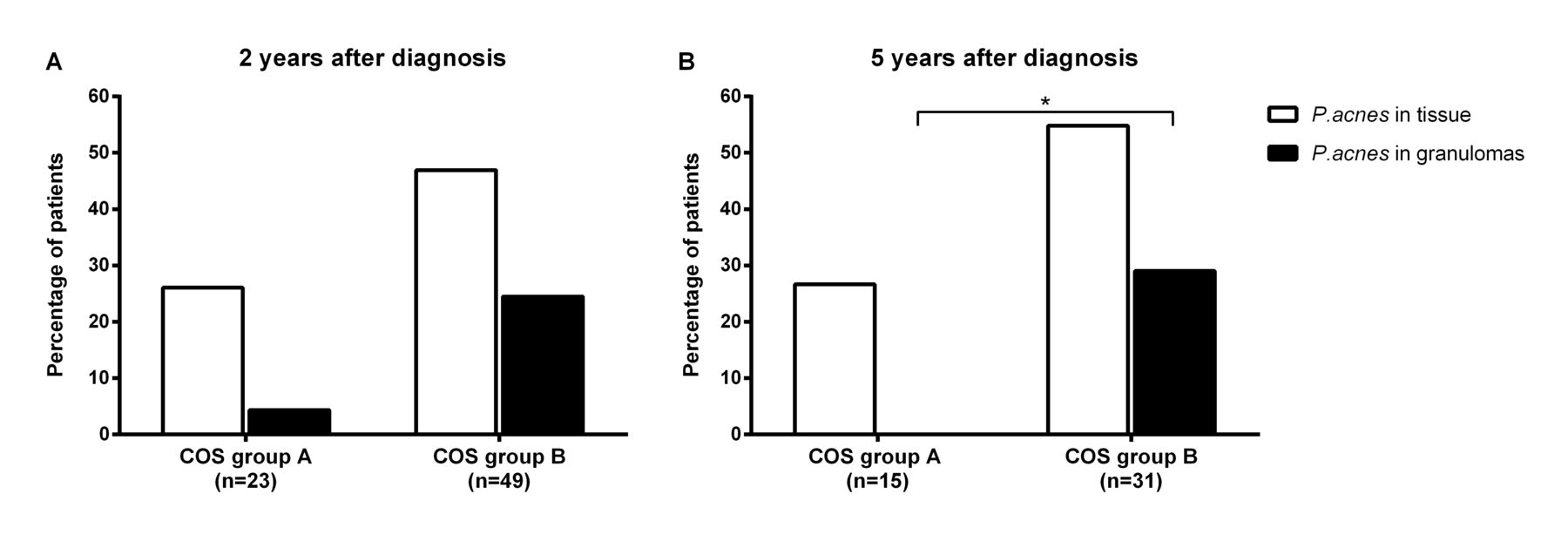
Presence of P. acnes in tissue was compared between the two COS groups defined 2 and 5 years after diagnosis. Two years after diagnosis, a trend (p=0.093) towards a higher prevalence of P. acnes in tissue was seen in COS group B (47%, 23/49) compared to COS group A (26%, 6/23). When comparing presence of P. acnes specifically inside granulomas, also a trend (p=0.050) towards a higher prevalence was seen in COS group B patients (25%, 12/49) compared to COS group A patients (4%, 1/23) (fig. 3a). COS defined after 5 years revealed a trend (p=0.072) towards a higher prevalence of P. acnes in tissue in COS group B (55%, 17/31) compared to COS group A (27%, 4/15). A significantly higher percentage of patients within COS group B (29%, 9/31) were positively stained for P. acnes inside granulomas compared to COS group A patients (0, 0/15) (p= 0.021, fig. 3b).

Frequency of P. acnes detected in tissue samples from sarcoidosis patients with a different clinical outcome status 2 years (a) and 5 years (b) after diagnosis COS group A=Resolved, minimal or persistent disease without treatment (COS 1–6). COS group B=Persistent disease with need for treatment (COS 7–9). PAB: P. acnes-specific monoclonal antibodies that react with cell-membrane-bound lipoteichoic acid.
Since COS group B can be a very heterogeneous group of patients, ranging from patients with remission of symptoms due to long-term corticosteroid treatment to severe therapy refractory patients requiring third-line medication, we also determined whether presence of P. acnes in tissue and granulomas was specifically related to patients requiring third-line medication at follow up. In a significant higher percentage of patients using infliximab, P. acnes was present in granulomas compared to non-third-line therapy requiring patients (33% versus 8%, p=0.009) (fig. 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Frequency of P. acnes detected in biopsy samples from sarcoidosis patients with or without thirdline therapy (infliximab) during follow up. A significantly higher percentage of third-line therapy requiring patients (all using infliximab) showed presence of P. acnes in granulomas than patients who did not require third-line therapy (p=0.009). PAB: P. acnes-specific monoclonal antibodies that react with cell-membrane-bound lipoteichoic acid.
Discussion
In this study we demonstrated that P. acnes is present in granulomas of Dutch patients with sarcoidosis, which is in line with previous studies in Japanese and German sarcoidosis patients [20]. Furthermore, to the best of our knowledge, our study is the first to show a relation between presence of P. acnes and clinical outcome in sarcoidosis. Regardless of whether the role of P. acnes might be antigenic or mitogenic, this data adds to the rational that P. acnes might be involved in the disease pathogenesis of sarcoidosis.
Negi et al. [20] previously examined the presence of P. acnes in tissue samples from sarcoidosis patients, using the same PAB antibody as used in the current study. A remarkable difference was found in percentage of P. acnes positive sarcoidosis patients. They found P. acnes in granulomas in 57% of the 77 lung samples from Japanese sarcoidosis patients whereas we found P. acnes in granulomas in 22% of the 32 lung samples from Dutch sarcoidosis patients. This difference could be partially explained by the lower proportion of VATS samples (35% in their study compared to 22% in our study). Negi et al. described that P. acnes in granulomas was more frequent detected in VATS samples compared to TBLB samples, probably due to the larger size of VATS samples. Similar to the lung samples, the percentage of Dutch patients with presence of P. acnes in granulomas of lymph node samples (8%) was lower compared to Japanese and German patients (88% and 89% respectively). Although the difference between Japanese and Dutch patients may be explained by difference in ethnicity, this is not a plausible explanation for the difference between German and Dutch patients. The difference in the detection frequency of P. acnes in granulomas can possible be caused by a lower sensitivity of immunostaining method used in our study. Therefore, future studies will have to compare the detection sensitivity of P. acnes in granulomas using the different immunostaining methods. It is however important to state that the localisation and pattern of P. acnes within and outside granulomas was comparable with the study of Negi et al. Specifically, we observed that presence of P. acnes outside granulomas was most frequently detected directly adjacent to granulomas but also in granuloma-free parts of the tissue in a few cases. Furthermore, the pattern within granulomas was comparable, with more intense dot like structures in immature granulomas and more sparsely- distributed staining or even no staining in mature granulomas.
A new and clinical relevant finding, in our opinion, is the fact that this is the first study that shows an association between presence of P. acnes and clinical outcome in patients with sarcoidosis. We observed that presence of P. acnes in tissue and in granulomas is more frequently found in patients with a chronic disease course requiring chronic treatment. Several studies demonstrated the mitogenic properties of P. acnes on different immune cells [16, 24, 25]. Our study was not aimed to prove that P. acnes has a specific etiologic role in sarcoidosis. However, in our opinion, the results do suggest that at least a potential mitogenic role of P. acnes may contribute to sarcoidosis disease pathogenesis. It is tempting to speculate that presence of P. acnes in or around granulomas can enhance an ongoing inflammatory reaction in sarcoidosis, contributing to perpetuation of the inflammatory granulomatous response seen in some patients. If this holds true, it is interesting to see whether decreasing the bacterial load of P. acnes using antibiotics can be beneficial in a subgroup of patients with sarcoidosis.
A case report already described a good effect of clarithromycin on fever, joint pain, FDG uptake on PET-CT, CRP and s-IL2R levels in a sarcoidosis patient in whom P. acnes was present in granulomas [26]. Moreover, a retrospective study described good responses on treatment with minocycline in P. acnes positive cutaneous sarcoidosis patients [27]. When we examined severe therapy refractory patients for presence of P. acnes, we observed that patients requiring infliximab treatment at follow up, had more often presence of P. acnes in granulomas at diagnosis compared to patients without treatment or treated with first or second line treatment. If antibacterial treatment in sarcoidosis patients with presence of P. acnes in tissue and granulomas is beneficial, the requirement of 3rd line treatments (e.g. infliximab) may be prevented.
Currently, in a randomised controlled clinical trial (J-ACNES), the effect of antibacterial drugs in addition to standard corticosteroid therapy in cardiac sarcoidosis patients is examined [28]. However, in this trial presence of P. acnes in myocardial tissue was not an inclusion criterion. Therefore, in future studies it would be interesting to have information on the presence or absence of P. acnes in these patients while investigating the effect of antibiotic therapy.
A limitation of the study was that the COS after 5 years could not be determined in all patients. However, since the proportion of patients within COS group A and B was quite similar after two and 5 years and the results regarding association with P. acnes staining as well, we assume that this analysis on a smaller group of patients has not introduced a bias. A disadvantage of using COS is the fact that disease status and medication use have been retrospectively assessed. Since we only scored whether medication was used or not, we have no information on patients who declined the use of medication while they actually needed it.
Another limitation is that we probably have a more severe patient group than other general hospitals, since the Antonius Hospital is an national referral center for ILD and Sarcoidosis. As a consequence we had very few patients in the resolved and minimal disease COS groups. For this reason we had not enough patients in every group to adequately analyse whether disease status alone, irrespective of use of medication, was associated with presence of P. acnes in tissue and granulomas. However, instead of disease status we think that need for treatment could be of more value regarding presence of P. acnes. If we want to further explore the use of antibacterial therapy, in our opinion, it is more relevant to focus on patients who actually need treatment.
In future studies, it would be interesting to add a second detection method, such as PCR, to the immunostaining. To accurately compare the results, development and use of a primer specific to LTA of the P. acnes bacteria would be valuable.
To conclude, this study confirms the presence of P. acnes in tissue and granulomas of respectively 40% and 17% of Dutch patients with sarcoidosis. Interestingly, the presence of P. acnes inside granulomas of Dutch sarcoidosis patients was associated with a chronic disease phenotype and requirement of treatment. Regardless of whether the role of P. acnes is antigenic or mitogenic, our data contribute to the premise that it is relevant to further explore antibacterial therapy as a treatment option for a subset of sarcoidosis patients.
Footnotes
Author Contributions: EB contributed to data acquisition and analysis, statistical analysis and drafting and editing of the manuscript. KS participated in the design of the study, scored the staining results and edited the manuscript. YE developed the PAB antibody, advised on study design and edited the manuscript. KU reviewed the methods and advised on the automated staining protocol. JD cared out all the immunohistochemical stainings and developed the automated staining protocol. JG supervised the project and edited the manuscript. MV designed the study, supervised the project and edited the manuscript.
Support statement: This study is part of the TopZorg Lung grant funded by ZonMw (nr 842002001). This funder had no involvement in the study design; in the collection, analysis and interpretation of the data; in the writing of the report; or in the decision to submit the paper for publication. ZonMw; DOI: http://dx.doi.org/10.13039/501100001826; Grant: 842002001.
Conflict of interest: Dr. Beijer has nothing to disclose.
Conflict of interest: Dr. Seldenrijk has nothing to disclose.
Conflict of interest: Dr. Eishi has nothing to disclose.
Conflict of interest: Keisuke Uchida has nothing to disclose.
Conflict of interest: Dr. Damen has nothing to disclose.
Conflict of interest: Dr. Grutters has nothing to disclose.
Conflict of interest: Dr. Veltkamp has nothing to disclose.
- Received July 10, 2020.
- Accepted November 5, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










