



Effect of facial skin cooling induced by a handheld fan on the cough reflex threshold and urge to cough induced by citric acid
- 1Dept of Physical Therapy, Faculty of Health Care Sciences, Himeji Dokkyo University, Himeji, Japan
- 2Dept of Rehabilitation Medicine, Toho University Graduate School of Medicine, Tokyo, Japan
- Masashi Kanezaki, Dept of Physical Therapy, Faculty of Health Care Sciences, Himeji Dokkyo University, 7-2-1, Kamiohno, Himeji, Hyogo, Japan. E-mail: kmasashi{at}gm.himeji-du.ac.jp
Abstract
Facial skin cooling induced by a handheld fan alleviates the cough reflex and the urge to cough induced by citric acid http://bit.ly/2m1kzAP
To the Editor:
Chronic cough is a condition that impairs the quality of life of affected patients and may persist despite optimal intervention. Thus, a novel therapeutic approach with broad clinical utility based on the nature of the cough reflex is required.
Galbraith et al. [1] studied the effectiveness of a handheld fan in reducing dyspnoea by blowing air into the nose and mouth in patients with advanced disease. Because several pulmonary and airway sensory receptors and afferent pathways show similarities between cough and dyspnoea [2], a handheld fan could be an effective antitussive therapy.
Recent studies have suggested the role of trigeminal nasal afferent neurons in antitussive effects in guinea pigs [3]. Based on the inhibition of dyspnoea by handheld fan air-blowing to the face, innervated by the trigeminal nerve branches, we tested our hypothesis that stimulating a trigeminal somatosensory input by blowing air across the face alleviates cough and the urge to cough produced by citric acid in healthy volunteers.
20 participants (11 men and nine women, mean±sd age of 21.3±2.4 years and body mass index of 21.2±2.2 kg·m−2) were included in our randomised, single-blind, controlled, crossover study of the handheld fan and control conditions. The hypothesis of the study was not revealed to any of the participants before the challenges. All participants were recruited by public postings in and around the Himeji Dokkyo University campus (Himeji, Japan). Subjects had no history of cigarette smoking, pulmonary or airway diseases, recent (within 4 weeks) suggestive symptoms, respiratory tract infection, or seasonal allergies. Subjects were receiving any regular medication, were instructed to not apply make-up before the experiment and underwent five sessions separated by a 24-h interval within a 2-week period. Visit 1 was a baseline assessment, visits 2 and 3 aimed to assess the cough reflex thresholds and the urge-to-cough log–log slope in the handheld fan and control conditions, and visits 4 and 5 aimed to determine the urge to cough induced by citric acid concentrations labelled M1–4 in the control and handheld fan conditions.
During visit 1, subjects were trained in the use of the handheld fan and the modified Borg scale. To determine baseline cough reflex thresholds and the urge to cough, a cough challenge was performed under normal tidal breathing using citric acid delivered by an ultrasonic nebuliser (NE-U17; Omron Co. Ltd., Kyoto, Japan) through a mouthpiece with a nose clip [4]. Citric acid solutions ranging from 0.7 to 360 g·L−1 in concentration were delivered sequentially in two-fold incremental concentration intervals. Participants were instructed to cough freely. Following each 15-s inhalation, the number of coughs was counted by an experienced operator for 1 min. The cough reflex thresholds were defined based on the citric acid concentrations that evoked the initial two or more coughs (C2) and five or more coughs (C5). After each inhalation, participants rated the magnitude of their urge to cough from 0 (no discernible urge) to 10 (maximal urge) according to modified Borg scale [5]. The estimated urge-to-cough scores were plotted against the corresponding citric acid concentration using a log–log transformation [5]. Because the estimated urge-to-cough scores and tussive agent concentration are known to have a linear relationship on a log–log scale, the slope and intersection were determined by linear regression analysis. During visits 4 and 5, to confirm the effect on the urge to cough using a handheld fan under similar citric acid inhalation conditions, moderate stimulus intensity (M1) was defined as the minimum citric acid concentration that caused an urge to cough with a rating of ≥6 according to the baseline cough reflex challenge. Furthermore, M2 (M1/2), M3 (M2/2) and M4 (M3/2) were defined for each participant.
During visits 2 and 3, the cough reflex challenges were performed in the handheld fan and control conditions, assigned in a randomised crossover manner on different days. The area of the face innervated by the second and third trigeminal nerve branches was set as the target for blowing air by handheld fan (YGH365B; Best-Fire, China) which was positioned 5 cm away from the face. In the control condition, the target was set on the back of the hand. The handheld fan was used only during the cough challenge. The size of the handheld fan used for the study was 85 g (15×4×7 cm), and it had three soft rotor blades and an unfoldable rotor unit. Furthermore, subjects received an information leaflet with explanations and instructions regarding handheld fan use.
During visits 4 and 5, the effect of the handheld fan on the urge to cough was examined using the M1–4 concentrations previously defined in the baseline cough reflex challenge during visit 1. The magnitude of the urge to cough during 15-s inhalations of M1–4 concentrations was evaluated under control or handheld fan conditions.
All participants provided written informed consent and the study was approved by the Institutional Ethics Review Board of Himeji Dokkyo University (Himedokusei 17-07). This study was registered with the University Hospital Medical Information Network (UMIN) in Japan (study identifier: UMIN-CTR; UMIN000030478).
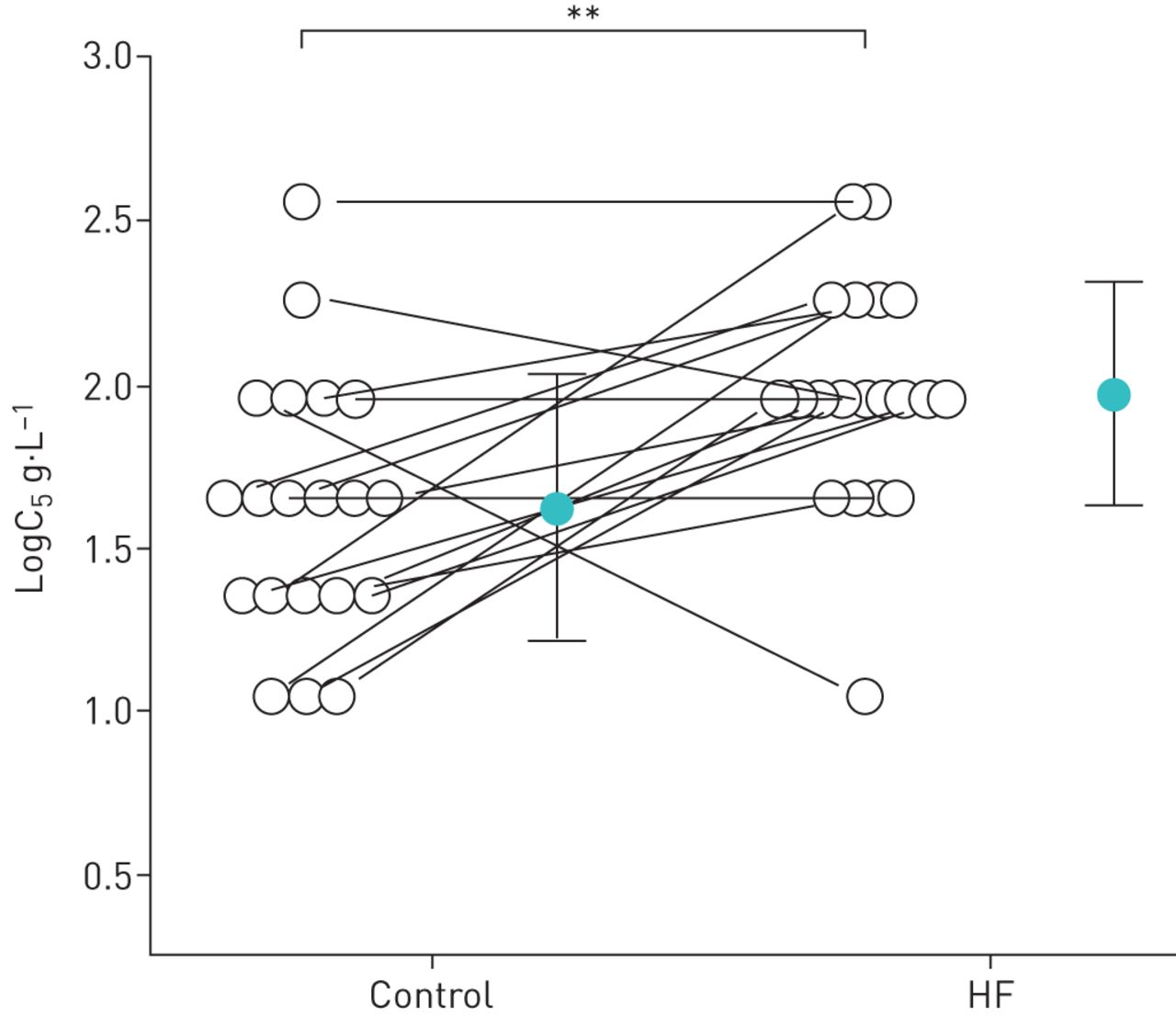
All participants completed the experiments without any difficulty or side-effects and described a cooling sensation on the face during the handheld fan condition. The cough reflex thresholds, expressed as logC2 and logC5, were significantly higher in the handheld fan condition (logC2 1.65±0.42 g·L−1 and logC5 1.97±0.35 g·L−1) than in the control condition (logC2 1.22±0.42 g·L−1 and logC5 1.62±0.40 g·L−1) (p<0.001 and p<0.01, respectively) (figure 1).
{kind=link}
Cough reflex threshold expressed as the logarithmic transformation of the lowest concentration of citric acid that elicited five or more coughs (C5). Closed circles and error bars indicate the mean value and the standard deviation in each condition, respectively. Open circles indicate the value of each subject. HF: handheld fan. **: p<0.01.
The log–log slope and intersection between the citric acid concentration and the urge-to-cough scores using the modified Borg scale were estimated for each subject. The log–log slope for the urge to cough was significantly lower in the handheld fan condition (0.46±0.19 point·g·L−1) than in the control condition (0.72±0.30 point·g·L−1) (p<0.003). However, no significant difference in the log of the urge-to-cough threshold was observed between the control and handheld fan conditions (data not shown).
In the present study, the urge to cough evoked by citric acid inhalation revealed a significant association between the control and handheld fan conditions and M1–4 concentrations. The urge to cough evoked by citric acid from M1 to M2 was significantly lower in the handheld fan condition than in the control condition (p<0.001 and p<0.001, respectively).
To our knowledge, this was the first study to show that using a handheld fan to blow air onto the face alleviates the cough reflex threshold and citric acid-induced urge to cough. Furthermore, no significant changes were observed between control and handheld fan conditions in terms of the threshold and urge-to-cough scores at modestly low-dose citric acid challenges (M3–4).
Recent studies have demonstrated that vagal afferent cough inputs from the larynx travel via the jugular ganglia to the paratrigeminal nucleus, which is connected to the medullary and pontine trigeminal nuclei, the ventrobasal thalamus and the submedius thalamic nuclei in guinea pigs [6]. In addition, selected delivery of cold airflow or menthol vapour to the nose has been reported to suppress citric acid-induced cough in anaesthetised guinea pigs [3] and alleviate dyspnoea in humans [7]; these studies suggest a role of trigeminal nasal afferent neurons in antitussive effects [3]. Thus, the effect of a cooling sensation on the face, induced by a handheld fan, on cough and the urge to cough can result from afferent stimulation of the trigeminal nerves.
A major limitation of the study was that the lack of data on temperatures of the facial skin during the fan blow prevented us from investigating whether the skin of the face actually cooled down during fan treatment or if it was due to the tactile sensation on the facial skin of the airflow.
The nature of the cough reflex in humans, which can be modified by facial cooling by a handheld fan, may be applied as a novel technique to ameliorate chronic cough. However, we only studied healthy volunteers using an experimental cough model; thus, further studies are required to determine the effectiveness of handheld fans in patients with chronic refractory cough.
Footnotes
This study was registered with the University Hospital Medical Information Network (UMIN) in Japan (Study ID: UMIN-CTR; UMIN000030478). No data sharing allowance has been made for this study.
Conflict of interest: M. Kanezaki has nothing to disclose.
Conflict of interest: S. Ebihara has nothing to disclose.
Support statement: This study was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology (26870760, 23659375, 24300187, 24659397, and 257166), Research Grant for Longevity Sciences from the Ministry of Health, Labor and Welfare (H22-Junkanki-shi-Ippan-001), and Research Funding for Longevity Sciences (22-2) from the National Centre for Geriatrics and Gerontology. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received April 9, 2019.
- Accepted August 3, 2019.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.