



Global burden of COVID-19 pandemic on healthcare workers
- Eleni Papoutsi1,
- Vassilis G. Giannakoulis1,
- Vasiliki Ntella1,
- Sofia Pappa2 and
- Paraskevi Katsaounou1
- 1First ICU Dept, Evaggelismos Hospital, National and Kapodistrian University of Athens, Athens, Greece
- 2Dept of Psychiatry, Imperial College London, London, UK
- Paraskevi Katsaounou, Pulmonary and Respiratory Failure Dept, First ICU, Evaggelismos Hospital, National and Kapodistrian University of Athens, Faculty of Medicine, 45-47 Ipsilandou Street, Athinon 106 79, Greece. E-mail: paraskevikatsaounou{at}gmail.com
Abstract
Provision of PPE, placing experienced HCWs mostly in organisational positions, increasing testing, minimising exposure by adjusting shift schedules, and providing food and sleep facilities could be some restorative measures to protect HCWs from #COVID19 https://bit.ly/2zcVARW
The novel coronavirus disease (COVID-19) was declared a pandemic οn March 11, 2020. Healthcare workers (HCWs), though vital for the functioning of the health systems during this global pandemic crisis, are unequivocally exposed to increased risk of infection through direct contact with patients. The European Respiratory Society, in a signed joint statement at the end of March, urged the European Union and national governments to prioritise health and safety of the frontline fight against COVID-19 [1]. In COVID-19 Situation Report 82, the World Health Organization (WHO) subject stressed the under-representativeness and paucity of publications and national situation reports that provide information on the number of infected HCWs. In this report, 52 countries had reported a total of 22 073 HCWs that had contracted COVID-19 [2]. Considering the current paucity of consolidated data on this, we attempted to quantify the number of reported HCW infections and case fatalities from COVID-19 in different areas and countries.
We searched all relevant grey literature up to April 17, 2020, in order to identify the most up-to-date government reports, official statements and newspaper reports concerning community or hospital-related COVID-19 infections and deaths of HCWs. Although methods for assessing risk of bias in controlled trials are well established, these may not be appropriate when grey literature is also included [3]. Therefore, a collaborative process was applied, where any disputes were thoroughly discussed and debated by the authors before a consensus was reached. The percentage of HCW cases in relation to the total country, region or city cases was either provided by government reports or calculated as: In areas where an “at least” number was reported, the safest estimate was included. Similarly, case fatality was calculated as:
In areas where an “at least” number was reported, the safest estimate was included. Similarly, case fatality was calculated as: Simple descriptive statistics such as median and range were also utilised.
Simple descriptive statistics such as median and range were also utilised.
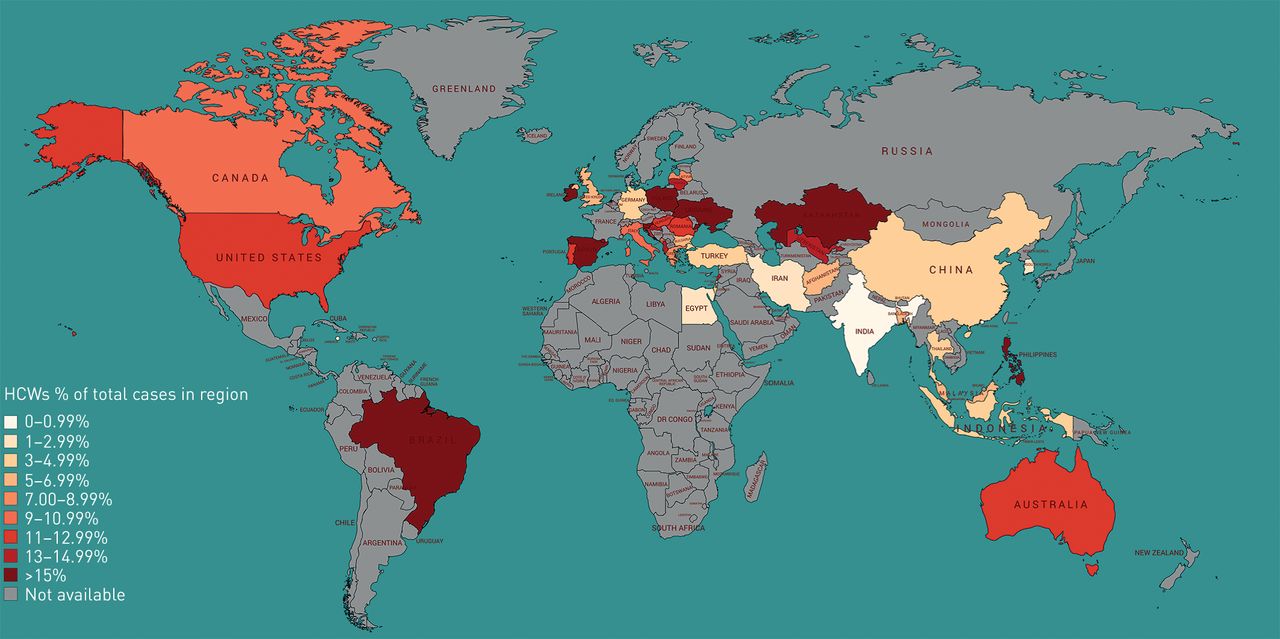
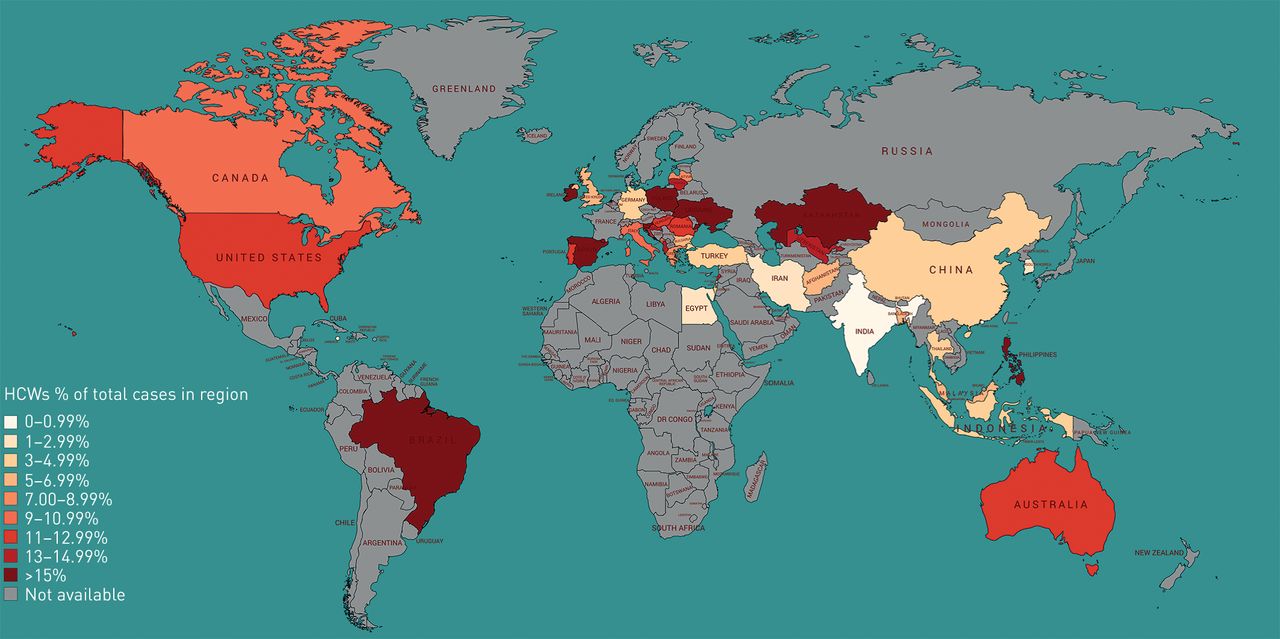
Data were available for 41 countries out of over 150 searched, a number close to the 52 reported by WHO. Where up-to-date data were not available, the most recent values were included. The retrieved findings are presented in table 1, showing the number of total cases and HCW infections, and case fatality, as well as health workforce density and total tests per million of population in each country (to assess health system and testing policy). Notably, in many countries, such as France, Finland and Sweden, data on the number of HCW infections could not be found. The percentage of HCW infections among total cases is depicted in a global, colour-scale map (figure 1). The median HCW infection percentage among total cases was 10.04% (range 0–24.09%). South Korea, Hong Kong (China), Iran, India, Egypt and Jamaica had <3% HCWs infected among total cases, whereas in Andorra, Brazil, Ireland, Kazakhstan, Philippines, Poland, Slovenia, Spain and Ukraine, the respective percentage was >15%. Case fatality could be calculated in 18 regions, with a median value of 0.8% (range 0–18.95%). The maximum case fatality value was observed in Indonesia (18.95%), followed by Uzbekistan (9%), Iran (8.41%), Egypt (6.52%), Philippines (2.83%), Alberta (Canada) (1.29%), Thailand (0.98%), Bangladesh (0.9%), Greece (0.8%), South Korea (0.8%), Italy (0.77%), China (0.67%), the UK (0.61%) and the USA (0.29%). Finally, we have also retrieved an “In Memoriam” list of healthcare workers who died of COVID-19 globally [4]. In this list, on the date accessed (April 8, 2020), age data were retrieved for 230 out of 341 HCWs, with a calculated median value of 62 years (range 24–93 years).
Healthcare worker (HCW) infections among total cases in each region and the respective case fatality on the same day of the report, searched as of April 17, 2020
{kind=link}
Global map depicting, in colour scale, the percentage healthcare workers (HCWs) among total cases in each region. Data for the following countries refer to certain regions: Australia (Victoria), Brazil (Sao Paolo), Canada (Alberta, British Columbia, Manitoba and Ontario) and Indonesia (Jakarta). This map was created at https://www.mapchart.net/ and is distributed under the terms of the Creative Commons Attribution ShareAlike 4.0 International Licence.
Contrary to aforementioned number of infected HCWs from WHO, our research revealed ≥67 569 cases of COVID-19 infected HCWs. Interestingly, countries in Asia seem to have lower infection rates among HCWs; this could possibly be attributed either to the readiness of these countries to deal with outbreaks [5, 6] or to the relatively lower health workforce density in south-east Asia [7]. However, a possible pitfall in comparing HCW infections across countries is that in each country, different policies regarding testing and other measures apply (e.g. under-reporting of total cases or prioritisation of HCW testing). In addition, findings derived from grey literature are inherently of limited quality and time-dependent due to the rapid progress of the situation.
Evidently, our findings represent only a “snapshot” of the current situation. However, they highlight the fact that the number of infected or deceased HCWs embody a concerning percentage of total cases in many countries. What is more, the median age of HCWs as calculated in the In Memoriam list reveals that a substantial proportion of them belonged to a vulnerable population subgroup. Nonetheless, the age of the deceased ranged between 24 and 93 years, highlighting that young and healthy HCWs could also be in danger.
A month after the declaration of COVID-19 as a pandemic, global health systems showed gross unreadiness for such a pandemic, leaving some of their HCWs as casualties. Adequate personal protective equipment (PPE) is essential for all healthcare professionals involved in the treatment of COVID-19 in order to protect their health and safety. However, the shortage of PPE worldwide, leaves most HCWs exposed to COVID-19. Moreover, since the virus is in the community and could be spread from asymptomatic carriers, HCWs not working with already diagnosed COVID-19 patients risk exposure to the virus and, hence, also need protective measures. Consequently, prioritising the provision of PPE, increasing testing, placing older, more experienced HCWs mostly in organisational positions, minimising exposure by adjusting shift schedules, providing food and sleep facilities, and regular breaks and adequate time off between shifts could be some first restorative measures in the right direction [8, 9]. Additionally, the importance of provisions for the mental wellbeing of HCWs should not be underestimated [10, 11]. Finally, adequate training of HCWs in the proper use of respiratory devices and handling of COVID-19 patients is essential, as this pandemic sets new norms.
The study is not without flaws as the use of grey literature and unsophisticated methodology present some challenges. However, in the absence of a completely consolidated picture, the present work is indicative and presents an opportunity to open vigorous public discourse on the safety of HCWs.
Acknowledgements
The authors thank Ilias I. Siempos from Weill Cornell Medicine, New York, NY, USA, for his insightful thoughts towards improving the manuscript, and Alexander Osarogue for proofreading.
Footnotes
The dataset and sources supporting the conclusions of this editorial are publicly available in the FigShare repository at https://doi.org/10.6084/m9.figshare.12148518.v1.
Author contributions: P. Katsaounou, E. Papoutsi, V.G. Giannakoulis and V. Ntella designed the study. E. Papoutsi, V.G. Giannakoulis and V. Ntella performed the literature search. S. Pappa helped with the literature search and reviewed the manuscript. V.G. Giannakoulis, E. Papoutsi and V. Ntella wrote the first draft of the manuscript. P. Katsaounou suggested improvements, wrote the second draft and supervised the publication. E. Papoutsi and V. Ntella created the supplementary table. V.G. Giannakoulis created the illustration. E. Papoutsi, V.G. Giannakoulis and V. Ntella contributed equally to this work.
Conflict of interest: V. Ntella has nothing to disclose.
Conflict of interest: S. Pappa reports travel grants and honoraria from Janssen, Sunovion and Recordati outside the submitted work.
Conflict of interest: V.G. Giannakoulis has nothing to disclose.
Conflict of interest: E. Papoutsi has nothing to disclose.
Conflict of interest: P. Katsaounou reports travel grants, honoraria and grants from Astra, GSK, Pfizer and Chiesi outside the submitted work.
- Received April 18, 2020.
- Accepted May 15, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.