



Social deprivation in Scottish populations with pulmonary hypertension secondary to connective tissue disease and chronic thromboembolic disease
- Michael McGettrick,
- Paul McCaughey,
- Alexander MacLellan,
- Melanie Brewis,
- A. Colin Church and
- Martin K. Johnson
- Michael McGettrick, Scottish Pulmonary Vascular Unit, Golden Jubilee National Hospital, Agamemnon Street, Clydebank, Glasgow, G81 4DY, UK. E-mail: michael.mcgettrick{at}nhs.net
Abstract
Socioeconomic factors have been shown to have an adverse impact on survival in some respiratory diseases. Studies from the USA and China have suggested worse survival in idiopathic pulmonary arterial hypertension in low socioeconomic groups. We looked at the effect of deprivation on the outcomes in patients with connective tissue disease-associated pulmonary hypertension (CTDPH) and chronic thromboembolic pulmonary hypertension (CTEPH) in a retrospective observational study.
Data were obtained from 232 patients with CTDPH and 263 with CTEPH who were under the care of the Scottish Pulmonary Vascular Unit, Glasgow, UK. We used Cox proportional hazards regression to assess for a relationship between deprivation and survival.
We found no difference in survival across deprivation quintiles in the CTDPH (p=0.26) or CTEPH cohorts (p=0.18). We constructed multivariate models using enrolment time, age, sex and body mass index, with no significant change in findings. There was no difference between expected and observed population distribution of CTDPH (p=0.98) and CTEPH (p=0.36). Whilst there was no difference in presenting functional class in the CTDPH group, the CTEPH patients in more deprived quintiles presented in a worse functional class (p=0.032). There was no difference between quintiles of CTEPH patients who had distal or proximal disease (p=0.75), or who underwent surgery (p=0.5).
Increased social deprivation is not associated with worse survival in patients with CTDPH and CTEPH managed in the Scottish National Health Service. Whilst there is no evidence of referral barriers in CTDPH, this may not be the case in CTEPH, as lower deprivation was associated with worse functional class at presentation.
Abstract
Increased social deprivation is not associated with worse survival in patients with connective tissue disease-associated pulmonary hypertension or chronic thromboembolic pulmonary hypertension managed in the Scottish NHS https://bit.ly/32KbzSv
Introduction
Socioeconomic status is measured by a number of factors, including income, housing, education and health status [1]. It has been well documented that social deprivation in the UK leads to a worse overall health status but there are other factors, including lifestyle choices, that affect morbidity and mortality in lower socioeconomic status groups [2]. Of concern, recent studies into chronic diseases have suggested that lower socioeconomic status is associated with adverse outcomes [3], including respiratory diseases such as chronic obstructive pulmonary disease and cystic fibrosis [4, 5].
Whilst prognostic demographic and clinical variables have been well defined in pulmonary hypertension, there is a paucity of data on the effects of social deprivation in this condition. Recent publications from the USA [6] and China [7] where there is insurance-based medical care suggest an adverse effect of deprivation. Patients present in a worse functional class and have worse survival overall.
Connective tissue disease-associated pulmonary hypertension (CTDPH) is in group 1 of the 2018 classification of pulmonary hypertension from the 6th World Symposium on Pulmonary Hypertension (Nice, France) [8]. It arises from increased pulmonary vascular resistance, secondary to a vasculopathy, which ultimately leads to right heart failure and death [9]. In the majority of cases, the condition is incurable and is associated with significant morbidity and has a high mortality rate. However, treatment prolongs time to clinical worsening and improves quality of life [10]. Treatment of CTDPH is mainly medical. Combination pharmacotherapy targeting the nitric oxide and endothelin pathways, in the form of phosphodiesterase inhibitors and endothelin receptor antagonists, is usually the first-line therapy. Those identified as high risk, or who deteriorate despite first-line therapy, are escalated to prostanoid therapy.
Chronic thromboembolic pulmonary hypertension (CTEPH) constitutes group 4 of the 2018 classification of pulmonary hypertension [11]. It is characterised by obstructive, fibrotic thromboembolic material within central and/or peripheral pulmonary blood vessels leading to a vasculopathy, progressive increase in pulmonary vascular resistance and, eventually, right heart failure [12]. For central disease, there is a potential cure available, in the form of pulmonary endarterectomy. For distal disease, surgery is not an option. There have been recent developments towards the use of balloon pulmonary angioplasty, but the mainstay of treatment is medical. Riociguat, a guanylate cyclase stimulator, and macitentan, an endothelin receptor antagonist, have been shown to reduce pulmonary vascular resistance and increase exercise capacity in distal chronic thromboembolic disease [13–15].
Pellino et al. [16] have published on the effect of social deprivation in heritable and idiopathic pulmonary arterial hypertension (PAH) in Scotland, UK, where healthcare is free at the point of need. This study demonstrated no effect of social deprivation on survival and suggested no obstacles to access to treatment. CTDPH and CTEPH comprise the majority of the remaining pulmonary hypertension patients where treatment with disease-targeted therapy for PAH is indicated. We aimed to establish the effect of social deprivation on survival and access to treatment of patients with CTDPH and CTEPH throughout Scotland.
Methods
The West Midlands–South Birmingham research ethics committee granted ethical approval (Research Ethics Committee Reference 16/WM/0419). We obtained data on all patients with CTDPH and CTEPH attending the Scottish Pulmonary Vascular Unit (SPVU) between 24 January 1992 and 7 September 2018. The SPVU is the only centre for pulmonary vascular disease in Scotland and, as such, diagnoses and manages all patients with pulmonary hypertension and gives a near-complete capture of patients within this well-defined area.
Both demographic and clinical variables recorded at the time of diagnoses were obtained. Demographic variables taken were age and sex. Postcodes at the time of diagnosis were used to calculate deprivation score. Clinical variables at diagnosis were World Health Organization (WHO) functional class, body mass index (BMI), right heart catheterisation haemodynamics (right atrial pressure, pulmonary arterial wedge pressure, mixed venous oxygen saturation and thermodilution cardiac output), 6-min walk distance (6MWD), N-terminal pro-brain natriuretic peptide (NT-proBNP), transfer factor of the lung for carbon monoxide (TLCO) and quality of life assessment using the emPHasis-10 score. Mortality events were collected from the patient's clinical records. To ensure that mortality during the study was not underestimated, a further check was made of survival status in May 2019 by confirming directly from clinical records that patients not seen since September 2018 were still alive at that time-point.
The Scottish Index of Multiple Deprivation (SIMD) is a tool developed by the Scottish Government, used to identify deprivation. The score combines seven domains: income; employment; health; education; skills and training; geographical access to services; crime and housing. The data from these domains are weighted and pooled to give a composite rank from 1 (most deprived) to 6976 (least deprived). The ranks are data areas based on postcodes. The ranks are then split into quintiles, with the first applied to the 20% most deprived zones and fifth assigned to least deprived. SIMD updates were published in 2004, 2006, 2009, 2012 and 2016 to reflect changes in deprivation over time.
We used the social distribution data from the National Records of Scotland, divided by sex, age and year, to calculate the expected distribution of SPVU patients with CTDPH and CTEPH amongst the social deprivation quintiles.
Quality of life was assessed using the emPHasis-10 questionnaire, which has been designed specifically for use in pulmonary hypertension. It is a multidimensional tool developed using qualitative research that assesses the physical perception of symptoms, the emotional effects and psychological distress. It consists of 10 questions, each graded on a six-point semantic differential scale (0–5), which has contrasting adjectives at each end (see supplementary material). The maximum overall score is 50. It has been validated with related patient outcome measures including the Hospital Anxiety and Depression questionnaire and the Dyspnoea-12 score. There is moderate correlation between emPHasis-10 and 6MWD, and it has been shown to discriminate subgroups of patients stratified as WHO functional class II and III [17]. It has also been shown to correlate with haemodynamic indices, specifically mean pulmonary arterial pressure and pulmonary vascular resistance, and with NT-proBNP [18].
To assess access to diagnosis and hence treatment, we looked at the difference between the expected and observed distribution of patients across the social deprivation quintiles. The expected proportions were derived from the distribution of the Scottish population as a whole across the deprivation quintiles, matched by age and sex. The population distributions are produced by the Scottish Government and updated in line with the SIMD.
Statistical analysis
Statistical analysis of data was performed using IBM SPSS (IBM, Armonk, NY, USA). Evaluation of possible links between quintiles and baseline variables were completed using multiple ANOVA for continuous outcome measures and Chi-squared for dichotomous measures.
In order to assess the association between survival and social deprivation, Cox regression analysis was used. 1-, 3- and 5-year mortality rates were calculated using Kaplan–Meier methods. Patients still alive at time of analysis or lost to follow-up were censored. Cox proportional hazard regression and Kaplan–Meier methods were used to evaluate baseline variables as prognostic markers. Hazard ratios, 95% confidence intervals and associated p-values were determined for each covariate.
Results
Data were obtained from 232 patients with CTDPH. 16% of the patients were male, which is in keeping with the known prevalence of connective tissue disease [19]. We obtained data from 263 patients with CTEPH, of which 53% were male. Median follow-up for CTEPH patients was 2.9 years and for CTDPH was 1.7 years. The relationship between clinical variables and social deprivation quintiles is shown in table 1. CTDPH patients in the least deprived quintiles presented in older age and were shown to have a significantly higher emPHasis-10 score than those in the more deprived quintiles. The CTEPH cohort in the most deprived quintile had significantly lower % predicted TLCO. These patients walked shorter distances over 6 min, and more of them presented in a worse functional class and with a worse quality of life.
ANOVA analysis of the relationship between social deprivation quintile and clinical variables
We divided the CTEPH patients into distal and proximal disease because of their different outcome [20]. 1-, 3- and 5-year survival rates of patients with CTDPH and distal and proximal CTEPH, for all patients, are shown in table 2. Univariate analysis (table 3) was performed using baseline clinical and demographic variables and showed prognostic significance for variables where it would be expected from previous studies [21]. We demonstrated prognostic value in the emPHasis-10 questionnaire in CTDPH.
Survival rates in connective tissue disease-associated pulmonary hypertension (CTDPH) and proximal and distal chronic thromboembolic pulmonary hypertension (CTEPH) patients across all social quintiles
Univariate analysis of all-cause mortality for baseline clinical variables in connective tissue disease-associated pulmonary hypertension (CTDPH) and both proximal and distal chronic thromboembolic pulmonary hypertension (CTEPH)
When looking for the effect of social deprivation on survival, we found no difference in survival across the SIMD quintiles in the CTDPH (p=0.26) or CTEPH cohorts (p=0.18). We constructed multivariate models using time of enrolment, age, sex and BMI, with no significant change in findings from the univariate analysis (see supplementary material).
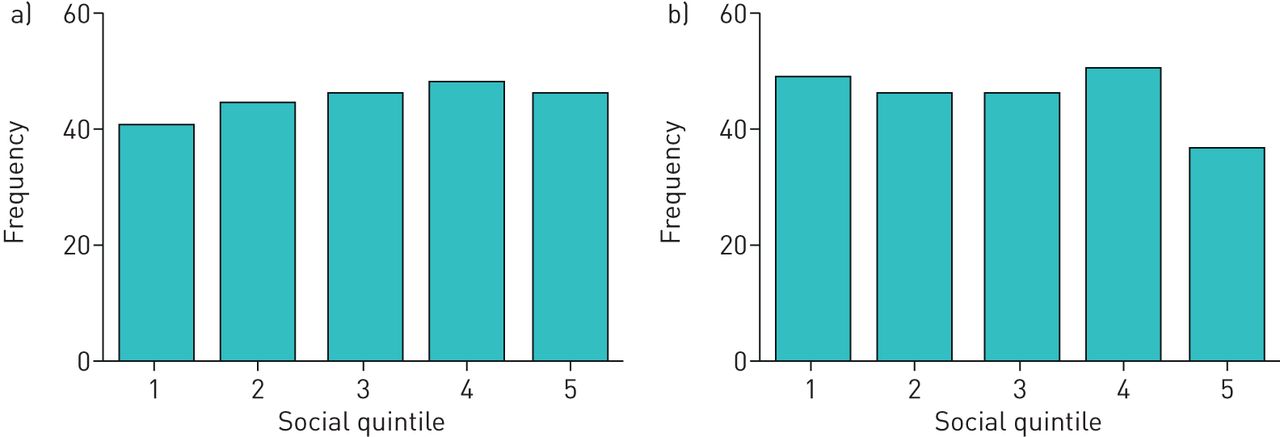
Figures 1 and 2 show the observed versus expected distributions of CTDPH and CTEPH across all deprivation quintiles. There was no significant difference between what we expected and what was observed in both groups.

The comparison between a) expected versus b) observed distribution of connective tissue disease-associated pulmonary hypertension (CTDPH) across social quintiles. p=0.98.

{kind=link}
{kind=link}
The comparison between a) expected versus b) observed distribution of chronic thromboembolic pulmonary hypertension (CTEPH) across social quintiles. p=0.36.
To assess access to surgery, we examined the proportion of patients who underwent pulmonary endarterectomy in each social deprivation quintile, and there was no significant variation (p=0.5 between quintiles). Given the influence of lifestyle choices in adverse outcomes in lower socioeconomic groups, we looked further into the reasons why patients did not have a pulmonary endarterectomy, and there were no significant differences between quintiles in those patients who were offered surgery but declined (p=0.26). There was no significant difference in the rate of distal versus proximal disease between quintiles (p=0.75).
Discussion
In this retrospective cohort study, we demonstrated no association between social deprivation and survival amongst patients with CDTPH and CTEPH in Scotland. We have, however, shown the prognostic significance of clinical variables usually associated with survival. This suggests that our data accurately reproduce the mortality behaviour seen in other pulmonary hypertension cohorts and lends confidence to the accuracy of the findings for social deprivation. Pellino et al. [16] have previously published the impact of social deprivation on patients with idiopathic PAH (IPAH) in Scotland and did not show any association. However, unlike in IPAH, we did not show any difference in the distribution of CTDPH or CTEPH amongst social deprivation quintiles when comparing observed to expected values. Whilst this may appear reassuring, the IPAH data would suggest that perhaps there should be a preponderance in the more deprived quintiles. Whereas patients with CTDPH did not present with a worse functional class, patients with CTEPH did, suggesting there are barriers to referral in CTEPH, incurring delay and leading to patients presenting in a worse condition. However, this did not lead to adverse survival outcomes. Baseline characteristics of our CTDPH and CTEPH patients are similar to those found in the IPAH cohort from the same centre, with similar age and functional class. Interestingly, our data suggest that the emPHasis-10 score appears to predict survival in CTDPH. Whilst the emPHasis-10 questionnaire has not been studied in the Scottish IPAH cohort, it has been shown to correlate with survival in IPAH in other centres [22, 23], but this has not been demonstrated in CTDPH. There is a trend towards significance in distal CTEPH, but small numbers limit the analysis.
The data that we present are supported by several Scottish studies looking at other health problems, but are in conflict with others. For example, Aitken et al. [24] assessed the effects of socioeconomic status on renal transplantation and showed no differences between the groups when measuring graft function or survival. Conversely, Shack et al. [25] showed that patients with lower socioeconomic status had a lower 5-year survival when they looked at patients diagnosed with the most common cancers. This could reflect differences in the way specific diseases are managed within the UK National Health Service (NHS). Alternatively, if a condition itself is associated with social deprivation, as common cancers are, then it may be more likely that survival too will be affected by the degree of social deprivation present, as it has been shown that people in lower socioeconomic groups are more likely to make lifestyle choices that will adversely affect their wellbeing [26].
There were no differences across the social quintiles between expected cases of CTDPH or CTEPH and those observed. A possible reason for this is that patients with connective tissue disease tend to have contact with healthcare professionals and are likely to undergo echocardiogram screening for pulmonary hypertension as part of standard care for connective tissue disease [27]. With regard to the CTEPH patients, they tend to present with an index case of acute pulmonary embolus and will have contact with medical practitioners as part of anticoagulation follow-up, so are likely to have a low threshold to having ongoing symptoms investigated.
This study was undertaken in a healthcare system where investigations and treatment are free at the point of need, and this may provide some explanation as to the differences seen in other centres looking at the effect of lower socioeconomic status on survival in pulmonary hypertension. Talwaret al. [6] and Wu et al. [7], both in private-based healthcare systems, showed disadvantage in those in lower socioeconomic groups. Given the lack of differences between social quintiles, our findings are a positive reflection on the performance of publicly funded healthcare in Scotland.
We used the SIMD as a measure of social deprivation. This is a well-validated, multi-domain tool developed by the Scottish Government, used to identify areas of deprivation. The factors included allow it to give a more realistic picture of overall social wellbeing. It is relatively specific as it is postcode based; the areas are small and of relatively similar population size. It is updated regularly to reflect changes in populations, whilst maintaining the same geographical boundaries.
Our study has a number of strengths. Although there have been studies looking at IPAH, this is the first study looking specifically at CTDPH and CTEPH. In addition, the SPVU is the only pulmonary hypertension centre in Scotland. As a consequence, the dataset in this study is not a sample open to bias but a complete population from a fixed geographical area. Finally, our unit is based in a healthcare system where investigations and treatments are free at the point of need, provided by the UK NHS. The results of this study echo the results from the IPAH population found by Pellino et al. [16], in that there were no significant differences in survival between demographic quintiles.
There are limitations within this study. First, this study is retrospective. Although the definition of pulmonary hypertension has remained constant and the unit had the same director for the duration of the study, we are relying on diagnostic practice not to have changed over the 16-year time period. NT-proBNP and emPHasis-10 scoring have not been used throughout the study period. Secondly, the small numbers in the divided CTEPH group affect the reliability of these results. Thirdly, despite this study covering the whole of Scotland, we have not absolutely excluded an association between social deprivation and survival in CTDPH or CTEPH. For example, it is possible that a reduced proportion of patients in the worse quintile are referred, although this is not supported by our observed distribution of patients across the quintiles. Further work from similarly funded healthcare systems would be useful to help validate our findings.
Conclusion
In this study we have demonstrated that increased social deprivation is not associated with worse survival in patients with CTDPH and CTEPH managed in the Scottish NHS. In addition, social deprivation does not appear to present a barrier to referral in CTDPH. However, this may not be the case in CTEPH, where increased social deprivation is associated with worse functional class at presentation.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
The Emphasis-10 Questionnaire 00297-2019.appendix
Supplementary material 00297-2019.supplement
Footnotes
Editorial comment in ERJ Open Research 2020; 6: 00638-2020.
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: M. McGettrick has nothing to disclose.
Conflict of interest: P. McCaughey has nothing to disclose.
Conflict of interest: A. MacLellan has nothing to disclose.
Conflict of interest: M. Brewis has nothing to disclose.
Conflict of interest: A.C. Church has nothing to disclose.
Conflict of interest: M.K. Johnson reports support for attendance at meetings, speaker fees, research grants and personal fees for advisory boards from Actelion and MSD, outside the submitted work.
- Received October 29, 2019.
- Accepted August 12, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.