



Is it feasible to perform a continuous laryngoscopy exercise test with a cold air inhalate? A case report
- Haakon Kvidaland1,2⇑,
- Sandra Stadheim3,
- Signe Bø3,
- Hege Clemm1,3,
- Ola D. Røksund1,4,5,
- Maria Vollsæter1,3 and
- Jon Hardie3
- 1Department of Pediatric and Adolescent Medicine, Haukeland University Hospital, Bergen, Norway
- 2Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway
- 3Department of Clinical Science, University of Bergen, Bergen, Norway
- 4Faculty of Health and Social Sciences, Western Norway University of Applied Sciences, Bergen, Norway
- 5Department of Otolaryngology and Head and Neck Surgery, Haukeland University Hospital, Bergen, Norway
- Haakon Kristian Kvidaland (Haakon.kristian.kvidaland{at}helse-bergen.no)
Abstract
The continuous laryngoscopy exercise (CLE) test can be combined with breathing cold air. Combining the CLE test and cold air does not cause excessive discomfort. The indicated laryngeal responses with cold air support the need for more research. https://bit.ly/3AChJ7V
To the Editor:
Exercise-induced laryngeal obstruction (EILO) describes laryngeal airflow obstruction during increased exercise [1], and is an important differential diagnosis for a variety of respiratory diseases, exercise-induced bronchoconstriction (EIB) being the most common [2]. The prevalence of EILO is reported to be as high as 27% among cross-country skiers [3], compared to 5–7% in the general young population [4, 5]. Breathing cold air may trigger airway obstruction in patients with EIB, and increase the test sensitivity [6].
The continuous laryngoscopy exercise (CLE) test is the gold standard for diagnosing EILO [7], without additional triggers other than exercise. Studies have discussed whether breathing cold air might induce EILO [8–10]. However, this has not been investigated systematically. We therefore aimed to see whether the CLE test is feasible to perform with cold air, in two patients with suspected EILO.
Two female participants (aged 27 and 28 years), otherwise healthy, with respiratory symptoms indicating EILO, were recruited from a specialist clinic for pulmonary diseases. They had been tested to rule out EIB prior to inclusion.
The regional ethics committee granted ethical approval (REK 109946), and informed written consent was obtained from the participants.
The two participants each completed two CLE tests 1 week apart, one while breathing room air (20–22°C) and one while breathing cold air (−15°C). Spirometry was performed before and 5 min after the CLE tests, measuring maximal expiratory flow volume curves [11].
The CLE test follows the setup described by Heimdal et al. [7]. A solution of 0.5 mL lidocaine hydrochloride (40 mg·mL−1) was applied in one of the nostrils. A flexible fibreoptic laryngoscope (Olympus ENF-V2, Tokyo, Japan), diameter 3.4 mm, was inserted via the nostril, to a position giving an optimal view of the larynx. The scope was attached to custom-made headgear and fixed to the nose using a plug in the nasal opening, taped externally on the wings of the nose. A nose clip closed the nasal opening. The laryngoscope allowed for video recording of the laryngeal inlet during the test.
The test protocol consisted of an 8-min running test on a treadmill with a 5.5% incline (Woodway PPS 55 Med, Weil am Rheid, Germany). The participants were asked to maintain a steady heart rate of 90–95% of estimated maximum heart rate (220 beats·min−1 − age) for the last 6 min. If the participants reached volitional exhaustion, they could stop earlier. Heart rate was measured using a heart rate monitor band (Polar H10, Kempele, Finland). The protocol was identical for both tests.
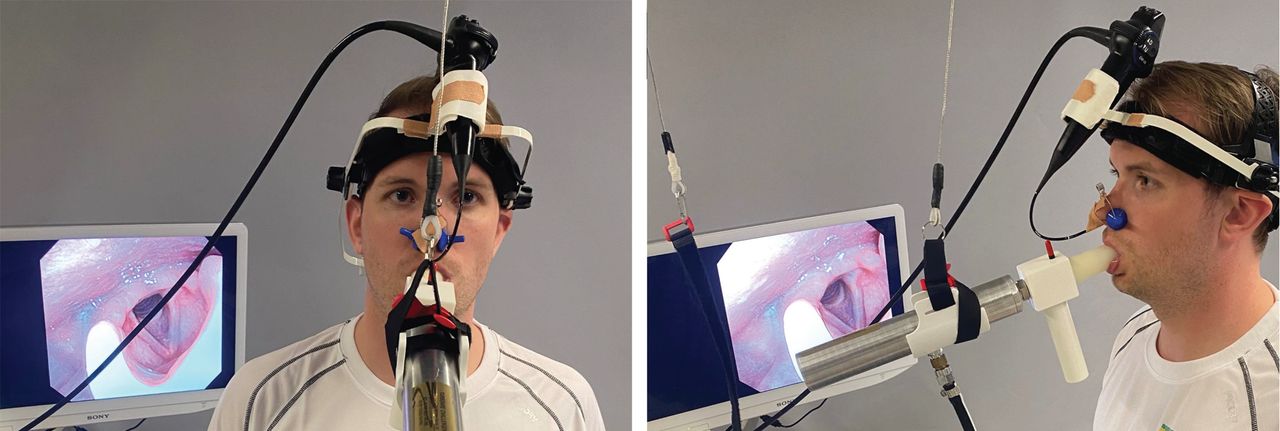
The TurboAire Challenger (Equilibrated Bio Systems, Melvillle, NY, USA) makes it possible to test ventilatory responses when breathing cold and dry air. The device is connected with medical air, and a pressure ∼6.8 bar provides an airflow of 240 L·min−1, creating an air temperature of ∼ −15°C (confirmed by a digital thermometer measuring at the outlet). The unit was hung from the ceiling and was adjusted to the subject's height. Figure 1 illustrates the complete setup.
{kind=link}
Continuous laryngoscopy exercise test with setup for breathing cold air. An experimental setup for a continuous laryngoscopy exercise test performed on a treadmill. The participant is breathing through a TurboAire Challenger biting over a mouthpiece. A wire connected to the celling adjusts the TurboAire Challenger. A gas flask with a pressure ∼6.8 bar gives the air a temperature ∼ −15°C.
CLE score was graded according to Maat et al. [12]. The scoring system contains four subgroups, each graded from 0 to 3 at glottic and supraglottic level at moderate and maximal effort. Higher scores indicate more laryngeal closure.
The Borg scale (CR10) was used to estimate perceived breathlessness immediately after exercise [13]. The scale goes from 0 (no breathlessness) to 10 (maximal breathlessness).
It was possible to combine the CLE test with the setup for breathing cold air, and the combination was well tolerated. Fixation of the laryngoscope directly to the nose and not through the facemask (as is normally done) gave a more unstable laryngoscope, and it was challenging to keep a steady video-recording. The part of the laryngoscope outside the nose tended to touch the TurboAire Challenger during vigorous running, causing additional disruption in the video-recordings.
At maximal effort, participant A had glottic obstruction grade 1 in room air and 3 in cold air. Participant B had no glottic obstruction in room air and grade 1 in cold air. Supraglottic scores did not differ. Participant A aborted the test after 3 min in cold air and 5 min in room air, with no Borg score difference. Participant B had Borg score 6 in room air and 7 in cold air.
There was no difference in spirometry pre- and 5 min post-exercise.
The CLE test is feasible to perform while simultaneously breathing cold air. Both participants ran to exhaustion on both tests and evaluated them as equal according to discomfort. The video-recordings were more unstable during the cold-air setup. Both participants had increased glottic obstruction when breathing cold and dry air.
It was more challenging to get satisfying video-recordings of the larynx when the participants were breathing cold air. We introduced the laryngoscope through a fitted plug in the nasal vestibule, and secured with nose clips and tape, but the laryngoscope was still not as steady as fixing it through a facemask.
During a standard CLE test, breathing sounds are registered. Noise from the TurboAire Challenger made it difficult to register respiratory sounds properly, and it was periodically challenging to differentiate between inspiration and expiration. In addition, the participants had difficulty communicating verbally while breathing cold air, and it was necessary to agree upon hand-signals beforehand.
The measured temperature in the TurboAire Challenger was ≤ −15°C, both pre- and post-test. However, it is challenging to predict the exact temperature of the air that passed through the larynx, as the inspired air heats when entering the mouth. However, this is not different from breathing cold air while exercising outside in the cold. Notably, we cannot separate the effect of dry versus cold air with this method.
Previous studies have reported that being surrounded by cold air might impact the lung capacity [14]. Using the setup described, air is travelling directly into the airways, and we are not able to investigate whether being surrounded by cold air impacts EILO.
Cold-air breathing may elicit bronchoconstriction in patients with airway hyperreactivity [15]. Thus, spirometry pre- and post-CLE test were performed 5 min post-exercise to ensure that differences in lung function did not affect the test result.
When CLE testing is already set up, the method does not require extensive resources and equipment to be performed. Besides breathing cold air, the original CLE setup is no different. This makes it easy for professionals familiar with the original CLE setup to perform this test.
The participants had a higher score on glottic obstruction when breathing cold air, and one participant quit the test earlier. The difference in performance between the tests corresponds with a more severe CLE score, underpinning the importance of investigating a potential connection between breathing cold air and EILO. To minimise the possible influence of a learning effect from one test to another, we randomised the order. The method in this study might be useful for future studies, to explore whether breathing cold air worsens or even causes EILO, and whether a certain subtype (glottic or supraglottic) is more affected with cold air.
Participant A aborted the test earlier than planned due to volitional exhaustion. Using an EIB protocol to diagnose EILO is not optimal, and a stepwise protocol to exhaustion may be more suitable to explore obstructions at different exercise intensities and at termination.
EILO patients should be investigated under different climatic conditions, such as temperature, humidity and altitude.
It is feasible to combine the CLE test with breathing cold air.
Acknowledgement
Tests were performed at the heart and lung testing laboratory at the Vitality Center for Children and Youth, Department of Pediatric and Adolescent Medicine, Haukeland University Hospital, Bergen, Norway.
Footnotes
Provenance: Submitted article, peer reviewed.
Conflict of interest: The authors have no conflicts of interest relevant to this article to disclose.
- Received April 2, 2022.
- Accepted August 24, 2022.
- Copyright ©The authors 2022
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org