Article Text

Abstract
Tracheostomy-associated ventilation for the respiratory insufficiency caused by amyotrophic lateral sclerosis (motor neurone disease (MND)) is a complex issue with practical, ethical and economic dimensions. This article considers the current prevalence of tracheostomy in MND, the evidence for its benefit both for survival and quality of life, and the practicalities of its implementation. The decision to request invasive ventilatory support is among the most challenging for those living with MND. Neurologists should be prepared to discuss this option openly and objectively: we suggest a framework for discussion, including withdrawal of therapy.
- amyotrophic lateral sclerosis
- motor neurone disease
- tracheostomy
- therapy
- prognosis
- ventilation
Statistics from Altmetric.com
Introduction
Motor neurone disease (MND), synonymous with amyotrophic lateral sclerosis, is a severely life-shortening neurodegenerative disorder in which a complex series of genetic and environmental factors result in progressive loss of motor neurones from the spinal cord, brainstem and motor cortex.1 There is clinical, histopathological and genetic overlap with behavioural variant frontotemporal dementia. Most MND cases appear to be sporadic, but genetic variants account for up to 15% of cases, the most common of which is a hexanucleotide expansion in C9orf72, associated with nearly 10% of all MND and 15% of all frontotemporal dementia.2
The essential clinical feature of MND is progressive loss of skeletal muscle strength, with death, usually due to ventilatory insufficiency, a median of 30 months from symptom onset. The pathway for those living with a diagnosis of MND involves multiple difficult decisions that have to be considered in the context of relentless loss of limb and bulbar function, where intervention to prolong life does not stop or slow the decline in physical independence.3 Invasive and permanent ventilatory support is one such intervention. In this review, we consider the current use of tracheostomy ventilation, the evidence for its benefit in MND, and the practicalities of its implementation and withdrawal; we also offer a framework for professionals to help people living with MND to make an informed decision on its application to their care.
The cause of death in MND
In counselling those living with MND, a frequent issue that arises and reinforces the motivation to undergo tracheostomy is the perception that the mode of death as sudden and unpleasant. Due to the diversity of care in the palliative phase of MND, and the overwhelming wish of most people to die at home, it is difficult to establish the cause of death objectively in most cases, and there are very few systematic and unbiased studies in population-based cohorts. It is generally assumed that most people with MND die of ventilatory failure, with or without superadded respiratory infection. However, MND specialists commonly encounter people who, based on disability scales such as the amyotrophic lateral sclerosis functional rating score (ALSFRS) and forced vital capacity measures would normally be predicted to live for months, yet in fact die unexpectedly and abruptly.
A French study of 302 people (which only captured 70% of all deaths predicted to be from MND in the study population, so with potential biases) found that 77% of those ascertained died of respiratory complications of MND (most were recorded as ‘terminal respiratory failure’, with some cases coded as bronchopneumonia).4 A smaller proportion of deaths were from pulmonary embolism, cardiac arrhythmia, head injury or suicide (each 2% or less), and less than 1% were from medical conditions unrelated to MND. The cause of death was undetermined in 13%. Typical ALSFRS scores at death were 15–17 (range of 9–28), which means that most were in a profound state of disability at the time of death. Studies from Italy and Germany report similar data, but with the additional information that 6%–12% died suddenly.5 6 A study of 100 postmortems may contain biases, as these were on people admitted to hospital after having undergone a precipitous decline7; this may explain their significant rate of pulmonary embolism (6%, mostly affecting spinal-onset disease with lower limb paralysis) as a likely contributor to the cause of death, and also a significant incidence (10%) of clinically relevant heart failure as a terminal event. Other plausible triggers of sudden unexpected death, but for which there is currently no clear evidence, might include cardiac arrhythmia, or loss of brainstem respiratory reflex control (eg, from neuronal loss in the pre-Botzinger nucleus).8 9 Note that asphyxiation through ‘choking’, a very common focus of anxiety for those living with MND, was exceptionally rare in these studies.
An important question is whether more intensive supportive treatment, non-invasive ventilation and enteral feeding, as well as tracheostomy, might change the mode of death in MND. Longer-term studies will be needed to provide a definitive answer, but a recent postmortem study indicated that in those using non-invasive ventilation, bronchopneumonia was significantly more frequent compared with those who were not.10
Prevalence of tracheostomy in MND
There are marked geographical differences in the prevalence of tracheostomy ventilation, even between countries of similar economic standing with near-identical diagnostic criteria and general disease management for MND. A review highlights some of this variation, although with the source articles not primarily focusing on prevalence of ventilatory support (Table 1, summarised from11). Factors that may influence a patient’s choice to have a tracheostomy include the neurologist’s preference, caregivers’ attitudes and presence or absence of advanced planning,12 and it is possible that this varies even between states of the United States or countries within Europe. Models of care funding may contribute to this variation but additional factors are also relevant, for example in Japan where there has been concern about the fear of legal action in shaping physician behaviour around end of life care.13 The increasing use of non-invasive ventilation in Europe has been driven by guidelines that emphasise the importance of maintaining the person’s ability to communicate, and their autonomy: for example, the National Institute of Health and Care Excellence Quality Standard on MND14 and European (European Federation of Neurological Societies) guidelines.15 From the financial perspective, in Japan, the cost of tracheostomy ventilation is fully covered by the government and medical insurance, and universal long-term care insurance was introduced in 2000.16 In contrast, in the UK National Health Service model and in other countries where funding is not readily available, securing funding for the additional care to provide for the more complex needs of an person on tracheostomy ventilation is a significant reason for delayed discharge.
Summary data on prevalence of non-invasive ventilation and tracheostomy ventilation in MND11
It is perhaps not surprising that in countries where tracheostomy ventilation is much less common than in Japan, most tracheostomies are inserted as an emergency, for example 30/38 (79%) in one survey from four UK centres, with 76% of these being related to acute illness requiring intubation (unpublished abstract17). Of those undergoing elective tracheostomy, two-thirds were men, three quarters wanted to live as long as possible or were struggling with continuous use of the non-invasive ventilation interface, and all lived with a partner or parent.
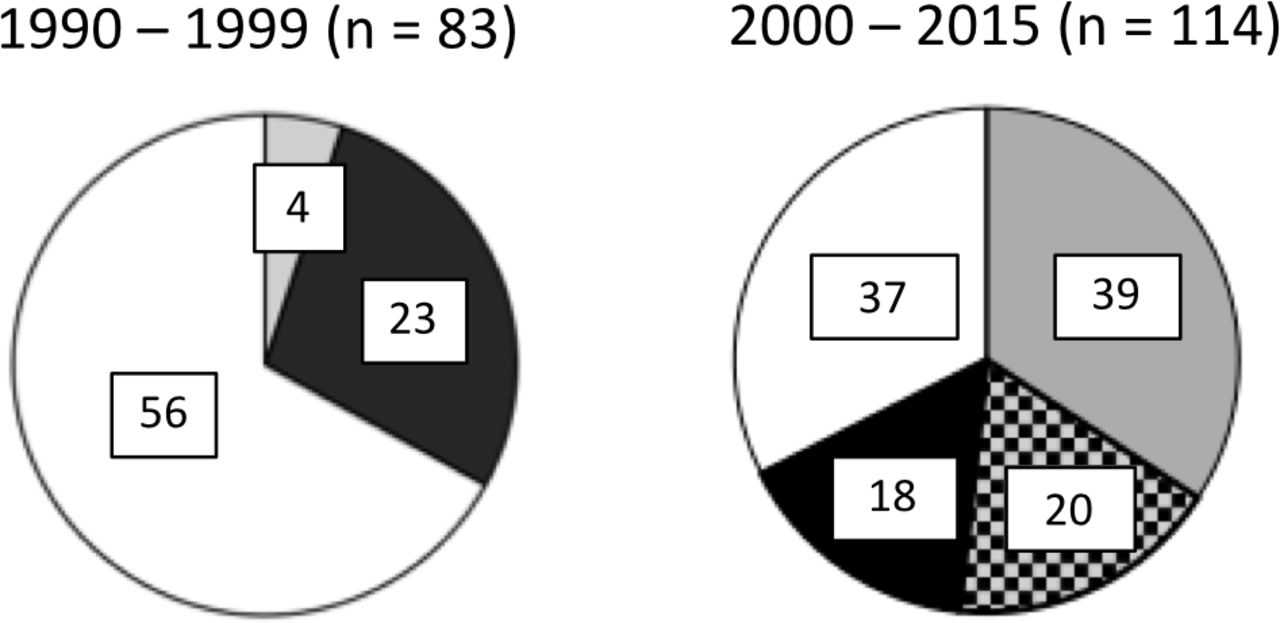
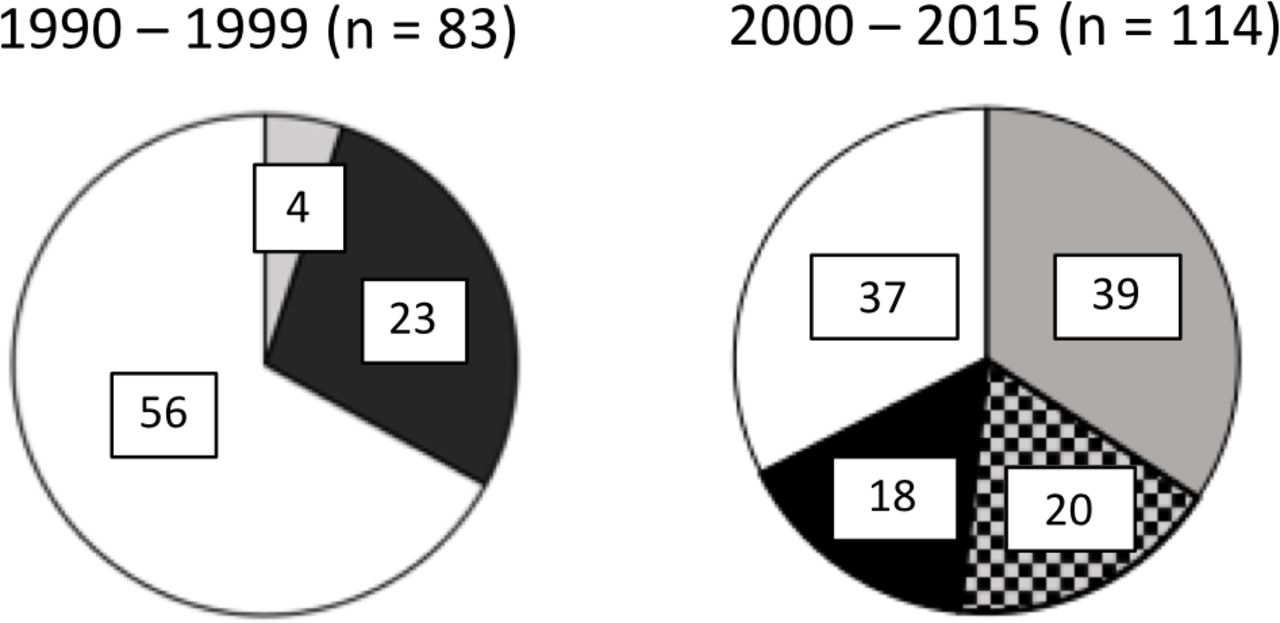
Patterns of ventilatory support provided to those with respiratory insufficiency due to MND in Japan have changed with time (figure 1). In a Japanese series, the proportion of those undergoing tracheostomy ventilation for MND has not changed substantially over a decade (28% and 33%) but, whereas non-invasive ventilation was infrequently used the early years (5%), it has been increasingly used over time (one-third overall, with half of these receiving tracheostomy ventilation in due course).16 As a consequence, more people now receive some form of ventilation (two-thirds compared with one-third in the 1990s). This change in practice has been attributed to publication of studies showing that non-invasive ventilation improves survival18 and quality of life18 19 is increasingly available and well tolerated.
{kind=link}
Number of individuals in a Japanese series with respiratory insufficiency secondary to MND receiving ventilatory support pre-2000 (left panel) and post-2000 (right panel) by modality. NIV alone (grey), NIV transitioning to tracheostomy ventilation (grey-black hashed) and primary tracheostomy ventilation (black) or no ventilatory support (white).16 MND, motor neurone disease; NIV, non-invasive ventilation.
The transition from non-invasive ventilation to tracheostomy ventilation is consistently much commoner in men than women.16 20 21 For example, in one cohort of 20, the male:female ratio was 17:3 in those transitioning, vers 19:20 in those continuing non-invasive ventilation.16 This difference may reflect a greater willingness of men to undergo invasive life-prolonging treatments. Having a caregiving spouse or partner may make a person living with MND who is considering a tracheostomy more willing to accept this invasive procedure. Those who are married were more than twice as likely to proceed to a tracheostomy and to have a longer survival after the procedure,22 23 although in multivariate analyses marital status is itself an independent predictor of survival in MND.
Differences in the clinical pattern of disease between men and women may also be relevant, with men being over-represented in younger-onset, lower motor neurone-predominant MND, which has an intrinsically slower progression and better prognosis,24 25 but often earlier respiratory muscle involvement. The probability of transitioning to tracheostomy ventilation reduces with the duration of non-invasive ventilation.16 Those who have used non-invasive ventilation for longer may have become more successfully accommodated to ventilatory support, and therefore the issue of invasive ventilation loses its immediacy. Although they may have accumulated greater physical limitation (and might therefore be reticent about escalating treatment), people who can tolerate long-term non-invasive ventilation probably also have different disease characteristics, though this is difficult to prove with small and highly selective studies. There is also a trend for those transitioning to tracheostomy ventilation to be slightly younger (65 vs 68 years).16
Evidence of benefit of tracheostomy in MND
In order to make an informed decision about tracheostomy ventilation, patients must consider the potential risks and benefits. There is no high-quality evidence to support the challenging discussions that take place when people living with MND raise the issue. It is important for healthcare practitioners to approach the conversation in an objective and value-free manner. Existing evidence can form part of the discussion as long as its limitations are acknowledged, including the impossibility of inferring direct causation about survival and quality of life in the absence of a controlled trial, and the considerable biases inherent in retrospective cohorts and anecdotal reports. Cases described of those who intended to have tracheostomy ventilation but then opted not to, and went on to have prolonged survival with non-invasive ventilation alone of 5 years, underline the uncertainty about choosing tracheostomy ventilation in order to increase survival.26 Accepting these limitations, several reports indicate survival in MND with tracheostomy ventilation of up to 74 months,23 26–33 with some indicating that people using tracheostomy ventilation had better survival than those receiving non-invasive ventilation alone. The decision to have elective tracheostomy ventilation, and indeed survival, was influenced by the person’s age, presence of a spouse and having enteral feeding. Interesting observations include the absence of a survival benefit in older people (over 60 years). If one accepts that tracheostomy ventilation affects survival, potential mechanisms in addition to the obvious effect of replacing the work of breathing using pressure support, include improving gas exchange, lung compliance and secretion management. Tracheostomy aftercare typically requires the 24 hours availability of highly trained personnel, whether in a managed care facility or at home. The increased level of specialist care may in itself play a major role in the reported survival benefit. Median survival after tracheostomy in a 10-year study Italian was 253 days (25% survived 3 years and 10% survived 5 years) with lower mortality in those followed at MND specialised multidisciplinary centres.23
Personality type may be a strong driver for survival, and it is often those with a desire to live at any cost, with an energetic drive to exert control of all aspects of MND, who undergo elective tracheostomy ventilation.34 However, the lack of systematic data on outcomes in tracheostomy ventilation make it difficult to draw any firm conclusions, particularly since much of the existing data relate to those who have undergone unplanned tracheostomy ventilation in respiratory crisis.35 Furthermore, people living with MND frequently change their mind about interventions or defer decisions. A major factor that appears to colour the attitude of physicians to tracheostomy ventilation in MND is the perception that it will have a negative effect on quality of life, particularly if a person loses the ability to communicate and has profound physical impairments. There is no high-quality evidence to draw on, and any studies that exist are by definition carried out retrospectively in the highly selected group undergoing tracheostomy ventilation, and are unlikely to be generalisable. In a small German study quality of life was assessed using questionnaires in those with tracheostomy ventilation (n=21) and their carers (n=20).36 Approximately 80% of those using tracheostomy ventilation indicated they would choose ventilation again and would advise others to do so. There were similar findings in two Italian cohorts.28 37 A common theme in these studies was the identification of high levels of stress and burden on the carers, with 30% of the tracheostomy ventilation caregivers rating their own overall quality of life lower than that of their loved one.
Finally, a key area for future study is how the efficacy of tracheostomy ventilation (as well as non-invasive ventilation) relates to the balance of clinical upper versus lower motor neurone involvement. Anecdotally, those with lower motor neurone-predominant phenotypes, those with respiratory-onset to symptoms, and those with slowly progressive disease may benefit most from tracheostomy ventilation, but this issue needs to be objectively delineated.
Logistics of tracheostomy in MND
Disease progression and transition to tracheostomy ventilation increase dependence on mechanical ventilation to prevent rapid death from respiratory failure. People living with MND depend not only on the ventilator but also on a team of carers, formal and informal, who work closely with expert clinical and technological professionals to ensure that the risks attached to ventilator malfunction, power failure, mucus plugging, tube displacement, etc. are managed in a timely and appropriate way to prevent permanent harm.
In Europe, recent studies show that between 62% and 86%17 37 of those who had tracheostomy ventilation in MND were discharged to their own home. 24-hour ventilation in a domiciliary setting can lead to significant carer burden, depression and burnout.28 37 Therefore, those living with MND and their families require appropriate information to enable informed decision-making regarding the final destination. Engagement of all stakeholders necessitates frequent multidisciplinary meetings with the person living with MND, or having their relative present throughout the hospital stay, particularly when planning and directly before discharge.
In the UK, most care at home for those with MND receiving tracheostomy ventilation is undertaken by trained carers (mean 22 hours) rather than by registered nurses (mean 2 hours).17 The situation in Europe is similar. In the United States, those with tracheostomy ventilation must have care provided by more expensive licensed practical nurses or registered nurses. Placement in a formal care setting does not always mitigate the risk, with several serious incidents involving ventilator-dependent individuals occurring over the past decade.38 39
Wherever the final destination or professional level of the primary carer, risk can only be managed through providing an appropriate team of formal care givers who are trained to a suitable level of competence to provide safe and effective care at home. Such packages are costly and can be extremely difficult to arrange and maintain. A 1:1 24-hour care package in the UK costs £180–200 k per annum. In the United States, a 16.5-hour package provided by licensed practical or registered nurses for those with tracheostomy has been costed at $270 k.40
Accessing funds via local continuing healthcare funding panels in the UK (and via insurance companies in other countries), together with recruitment and training of carers and safe discharge preparation, can all be fraught with logistical difficulties and delays. Following emergency tracheostomy for MND, mean length of stay in the UK is 18 weeks.17 Sometimes, funding can be authorised within a few weeks and for elective procedures could be sanctioned before admission. In one Spanish centre, the mean time to discharge from the respiratory care unit was just 27 days.29 Prolonged hospital stays lead to increasing burdens and frustrations for those living with MND, families and the institution. These are exacerbated by the patient’s and professionals’ lack of control in expediting discharge.
Financing the care package, however, does not mean that discharge is imminent. In the UK, a shortage of healthcare workers and the need for the necessary pre-employment checks cause delays, sometimes of many weeks, in recruitment to care agencies or, if using a personal care budget, directly to the care team. Once appointed, the eight or so carers required to provide 24-hour care, 7 days per week need to be trained to safely manage the ventilator-dependent individual, provide tracheostomy care, along with effective and safe augmented cough technique. In addition, some other training and equipment needs can hamper discharge. For example, enteral feeding, positioning and manual handling all need to be addressed to manage risk effectively on discharge. Sometimes, recruited carers have no previous experience of tracheostomy, ventilation and even MND, and their drop out can be high; others require many hours of working with the patient in hospital to achieve the required level of competence and confidence to provide safe management without supervision in their own home.
Uncuffed tracheostomy ventilation tubes, particularly where there is severe bulbar dysfunction may mean the individual remains at considerable risk of developing aspiration and bronchopneumonia. The ability to provide adequate chest clearance techniques mitigates this to some extent but nonetheless, the development of aspiration bronchopneumonia may remain high in those with an uncuffed tube. The majority (80%) of people with MND on tracheostomy ventilation receive a cuffed tube (UK audit by JP—unpublished). While a subglottic tube might allow safer deflation for the purposes of speaking, many living with MND have severe dysarthria at this stage anyway. An initially cuffed tracheostomy tube is usual in those admitted with acute respiratory failure. In that setting, some people diagnosed with MND may be able to be weaned completely to non-invasive ventilation, but this is less likely in those with significant bulbar dysfunction.
Withdrawal of tracheostomy in MND
It is profoundly important that clinicians discuss with individuals their wishes concerning future care as their MND progresses, especially in anticipation of the loss of the ability to communicate. For those with planned tracheostomy ventilation this should be a facet of the informed consent discussions. Advance care planning is not a single event and as their situation evolves, people with MND will value their views and thoughts about the future being revisited as a standard part of their care.41 42 Individual preferences may change over time and discussion enables people to develop a more considered view concerning assisted ventilation and resuscitation. It is very important that those living with MND and their families are aware that there is a choice about treatment and that they may change their mind.
In most, but not all, countries, it is entirely legal for someone to ask that their tracheostomy ventilation be stopped. The UK General Medical Council has clarified for doctors that such a request by person with capacity must be honoured in exactly the same way as it is for percutaneous gastrostomy and non-invasive ventilation. The MND Association provides excellent information about tracheostomy ventilation and considerations of choice in future care. Some may wish to document their wishes in relation to withdrawal of ventilatory support by completing paperwork that is of legal standing such as an Advance Decision to Refuse Treatment or appoint an attorney to make decisions on their behalf should they lose the ability to communicate their wishes (or lose mental capacity). All discussions should be documented and shared across the professionals and services caring for the person living with MND. These discussions may usefully be formalised in an advance statement of wishes and noted in treatment escalation plans such as the ReSPECT template recently introduced in England. These discussions need to consider the possibility of sudden, unexpected respiratory events so that attending staff aware of management decisions. The Association for Palliative Medicine of Great Britain and Ireland has developed clinical guidance to support best practice in withdrawing assisted ventilation (table 2).
Useful resources on institution and withdrawal of tracheostomy ventilation in MND
The withdrawal of assisted ventilation may rapidly lead to breathlessness and distress; effective management of these expected symptoms is a professional responsibility described in UK case law (eg, R v Adams 1957, Crim LR 365; House of Lords debate re: Annie Lindsell, Hansard HL 721–724, November 20 1997), and is similar to the anticipatory and ongoing symptom management required for painful procedures and operations. For many clinicians, this is a challenging area of practice, as it is rare and often raises practical and ethical concerns.43 44 It is crucial to involve palliative care. Preparation of the person living with MND, the family and the professional team is a key part of a safe and successful outcome. All parties need assurance about the ethics and legality. Professionals especially and occasionally family members can be concerned that this is assisted suicide or euthanasia. This has been discussed in the context of an Advance Decision to Refuse Treatment for stopping of ventilation for a person living with MND when they became unable to communicate.45
The process may take several hours, and the team needs to plan adequately for this and to prepare the family. Although the person will probably die within 15 minutes after the ventilation has been withdrawn, some have more respiratory reserve than anticipated and live longer (several days in exceptional circumstances). Symptoms require an individualised approach, with titration of a combination of an opioid and benzodiazepine (and occasionally additional drugs) to an adequate level of sedation before the tracheostomy ventilation is removed. The effectiveness of the symptom management should be assessed and adjusted by trial removal of the ventilation or reduced ventilation settings before complete removal. Both the subcutaneous and the intravenous routes for drug administration have proved effective. Although the subcutaneous route may require more time for the required level of sedation to be reached, it will be more aligned to the practices of palliative and end of life care and may be more feasible especially in the home and care home situations.
Single-centre case series in a Danish home ventilation service and German neurology service have been published.46 47 There is less experience of withdrawal of tracheostomy ventilation in MND in the UK since it is much less commonly used but the body of experience is systematically being documented through prospective evaluation.48 In the UK, most of the expertise in undertaking the withdrawal is vested in home ventilation nursing and palliative medicine and, while neurologists may have a key role in discussing initiating ventilation support, they will seldom have a role in stopping it.
Supporting decision-making
It is an axiom of optimal healthcare for the medical practitioner and the person with the illness to have a balanced discussion of risks versus benefits for any intervention. Proactively discussing tracheostomy ventilation in MND is a significant evolution from the reactive approach that is common practice currently. It is critical to understand the expectations of those considering tracheostomy ventilation, which may be based on unrealistic ideas about how the disease progresses. Furthermore, introducing ethically-charged concepts such as the best use of limited healthcare resources or consideration of the carer and family burden of tracheostomy ventilation49 is likely to be uncomfortable for both parties, though undoubtedly relevant to debate at a societal level.
MND has significant clinical and pathological overlap with frontotemporal dementia. Although overt dementia with loss of capacity in MND has an estimated prevalence of <15%, there remains uncertainty about the natural history of cognitive and behavioural decline. In initial studies, those without significant cognitive impairment at baseline did not appear to develop this during follow-up.50 However, the natural attrition in longitudinal MND studies is known to enrich for more ‘benign’ and slowly progressive phenotypes. Analysis using clinical staging systems based on motor decline does suggest a greater burden of extramotor involvement over time,51 with obvious potential impact for those contemplating long-term tracheostomy ventilation. The limited number of autopsy studies over several years in people with MND following tracheostomy ventilation shows significant clinical heterogeneity, in which there may be very profound cerebral (frontal) atrophy over less than a decade on tracheostomy ventilation, presumably with associated dementia,52 versus cases with preserved communication and sparse if any TDP-43 cortical pathology after a total disease duration of more than 30 years.53 The assessment of cognitive function becomes important in the optimal management and maintenance of autonomy of those with long-term tracheostomy ventilation in MND, and this is challenging for those unable to write or speak. Although the use of eye-tracking for cognitive function testing has potential,54 the resistance of oculomotor function in MND is only relative compared with limb and bulbar musculature, and the use of brain–computer interfaces is the next frontier.55
When discussing tracheostomy ventilation with patients, it is important to acknowledge the lack of evidence in this area. There is no simple equation for harm or benefit from tracheostomy ventilation in terms of survival and quality of life, and we need more research data to be certain which (if not all) clinical phenotypes benefit. A lay summary of the evidence, limited though it is, would be a good starting point. This could be followed by a description of the practicalities of living with tracheostomy ventilation. Open questions might then help to facilitate someone living with MND to explore all of the issues in tracheostomy ventilation (table 3).
Questions to consider in a broad discussion about tracheostomy ventilation in MND
Closing remarks
For a condition like MND, in which respiratory failure is the key feature defining the survival in most people, openness to discussion about tracheostomy ventilation should be part of routine multidisciplinary care. Non-invasive ventilation offers a clear quality of life and survival benefit for many people living with MND with symptomatic respiratory insufficiency, but tracheostomy ventilation is a more nuanced issue in which it is not currently possible to predict aspects of the long-term natural history of the condition. Identifying unrealistic expectations is important, but also acknowledging practical issues, including the availability of resources for healthcare delivery. Making the experiences of people living with MND who have made a firm decision either way in respect of tracheostomy ventilation, more widely available to those still in the decision-making process, might be a valuable resource.
Key Points
The majority of deaths in MND arise from complications of neuromuscular respiratory insufficiency.
Tracheostomy may extend survival in some cases of MND, but does not prevent the progression of muscle weakness.
Use of tracheostomy in the management of MND varies internationally, with a particularly high prevalence in Japan and low in the UK.
Safe and reliable home-based tracheostomy use requires a well-trained and responsive community team.
Withdrawal of tracheostomy at the request of a person with capacity is entirely legal. Optimal symptom management may require palliative care services.
Access to open discussion about the pros and cons of tracheostomy should be available for all those living with MND.
References
Footnotes
Contributors MRT conceived the review, drafted the introduction, discussion framework, conclusions, and synthesised the overall draft manuscript; CF drafted the section on withdrawal; CJMD drafted the section on benefit; AHN drafted the section on prevalence; JP drafted the section on logistics; KT drafted the section on cause of death; All authors edited the synthesised manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned. Externally peer reviewed by Robin Howard, London, UK, and Nigel Leigh, London, UK.
Other content recommended for you
- Assisted ventilation in motor neurone disease during inpatient palliative care: barriers and utilisation
- Withdrawal of invasive ventilation in a patient with motor neurone disease and total locked-in syndrome
- Respiratory management of motor neurone disease: a review of current practice and new developments
- The management of motor neurone disease
- Weaning from prolonged invasive ventilation in motor neuron disease: analysis of outcomes and survival
- Who will benefit from tracheostomy ventilation in motor neuron disease?
- Non-invasive ventilation in motor neuron disease: an update of current UK practice
- Understanding living with tracheostomy ventilation for motor neuron disease and the implications for quality of life: a qualitative study protocol
- Home tracheotomy mechanical ventilation in patients with amyotrophic lateral sclerosis: causes, complications and 1-year survival
- Withdrawal of tracheostomy ventilation in motor neurone disease: implementing advance directives