Article Text

Abstract
Background Cross-sectional studies have suggested a rapid expansion in paediatric long-term ventilation (LTV) over the last 20 years but information on longitudinal trends is limited.
Methods Data were collected prospectively on all patients receiving LTV over a 15-year period (1.1.95–31.12.09) in a single regional referral centre.
Results 144 children commenced LTV during the 15-year period. The incidence of LTV increased significantly over time, with an accompanying 10-fold increase in prevalence due to a significant increase in institution of non-invasive ventilation (NIV). There was no significant increase in invasive ventilation. 5-year survival was 94% overall and was significantly higher for patients on NIV (97%) than invasively ventilated patients (84%). 10-year survival was 91% overall. Although some children were able to discontinue respiratory support (21% at 5 years and 42% at 10 years), the number of patients transitioned to adult services increased significantly over time (26% of total cohort). Patients with neuromuscular disease were less likely to discontinue support than other patients.
Conclusions The paediatric LTV population has expanded significantly over 15 years. Future planning of paediatric hospital and community services, as well as adult services, must take into account the needs of this growing population.
- Respiratory
- Intensive Care
Statistics from Altmetric.com
What is already known on this topic
-
Cross-sectional studies have suggested a rapid expansion in paediatric long-term ventilation (LTV) over the last 20 years.
-
LTV patients are resource intensive and have a significant impact on both hospital and community services.
What this study adds
-
This study quantifies the expansion of long-term ventilation (LTV) in children and provides information on longitudinal trends and outcomes of LTV.
-
The incidence of LTV in children has increased significantly over the last 15 years, principally due to increased use of non-invasive ventilation.
-
About one in five children is able to discontinue respiratory support but increasing numbers are being transitioned to adult services.
Introduction
Advances in medical care and expansion of supportive care options have contributed to the survival of children with complex medical conditions, including those dependent on chronic ventilatory support.1 Cross-sectional surveys in a number of countries have described the patient population receiving long-term ventilation (LTV).2–10 A survey of Canadian centres in 1993 identified 82 children dependent on assisted ventilation, seven of whom were living in British Columbia.5 Serial cross-sectional surveys have suggested there has been a rapid expansion in paediatric LTV over the last 20 years.2 ,6 ,9 However, information on longitudinal trends in the number of patients, the profile of the LTV population and their outcomes is limited.
We sought to describe longitudinal trends in LTV over a 15-year period in a single regional referral centre that provides all paediatric LTV care for the province of British Columbia (population four million).
Methods
BC Children's Hospital is the tertiary paediatric referral centre for British Columbia and is the only centre in the province that establishes long-term respiratory support for children. A comprehensive database of all such patients has been maintained, with prospective data entry from 1993 to the present, allowing complete capture of data of all patients on LTV in the province. Data were collected on all patients aged 18 years or younger receiving LTV over the 15-year period from 1 January 1995 to 31 December 2009, using information in the database augmented by the patients’ hospital records. LTV was defined as ‘the continued requirement of a mechanical aid for breathing for all or part of the 24 h day, when medically stable and after an acknowledged failure to wean, 3 months after the institution of ventilation’.11 Premature infants who were likely to be weaned from ventilation were excluded, as were children with tracheostomy alone. Data were subdivided into three 5-year epochs for statistical analysis of longitudinal trends.
Results`
Overall patient characteristics
One hundred forty four children (85 (59%) male) commenced LTV during the 15-year period studied. In addition, six children (three male) were already receiving respiratory support at the beginning of 1995 (five invasive, one non-invasive ventilation (NIV))—these patients are included only in the prevalence data. Median age at initiation of LTV was 9.4 (0–18) years but there was a bimodal distribution with peaks in the 1st and 14th years of life (figure 1).

Age at initiation of long-term ventilation (LTV).
The principal diagnostic categories leading to requirement for LTV were neuromuscular disorders (including Duchenne muscular dystrophy (n=18), spinal muscular atrophy (SMA) type I (n=6), SMA type II (n=14), congenital or other myopathy (n=18)) (47%), spinal injury (6%), abnormal ventilatory control (acquired (n=16) or congenital central hypoventilation syndrome (n=3)) (13%), airway malacia (8%) and craniofacial abnormalities/obstructive sleep apnoea (OSA) (16%). The remaining 10% patients had a range of other conditions including diaphragm paresis postcardiac surgery, kyphoscoliosis, pulmonary hypoplasia secondary to giant omphalocoele and pulmonary involvement of Langerhans cell histiocytosis.
Twenty eight (19%) children were ventilated invasively via tracheostomy and 116 (81%) received NIV (22 continuous positive airway pressure (CPAP), 94 bilevel). For the patients on NIV, the main interface used was a nasal mask in 86 (74%), an oronasal mask in 25 (21%), nasal pillows in three (3%) and a total face shield in two (2%). Three patients, all with high cervical spinal cord injuries, used intermittent diaphragmatic pacing in addition to tracheostomy ventilation. 17/144 (12%) were ventilated for 24 h per day while 127 (88%) were supported for less than 24 h per day, typically during sleep only. Compared to only one child on NIV (χ2 63.8, p<0.001), 16 (57%) invasively ventilated children required 24 h/day support.
One hundred forty three (99.3%) children were discharged home on LTV. One patient died in hospital prior to discharge after 10 months of tracheostomy ventilation.
Longitudinal trends in incidence and prevalence of LTV
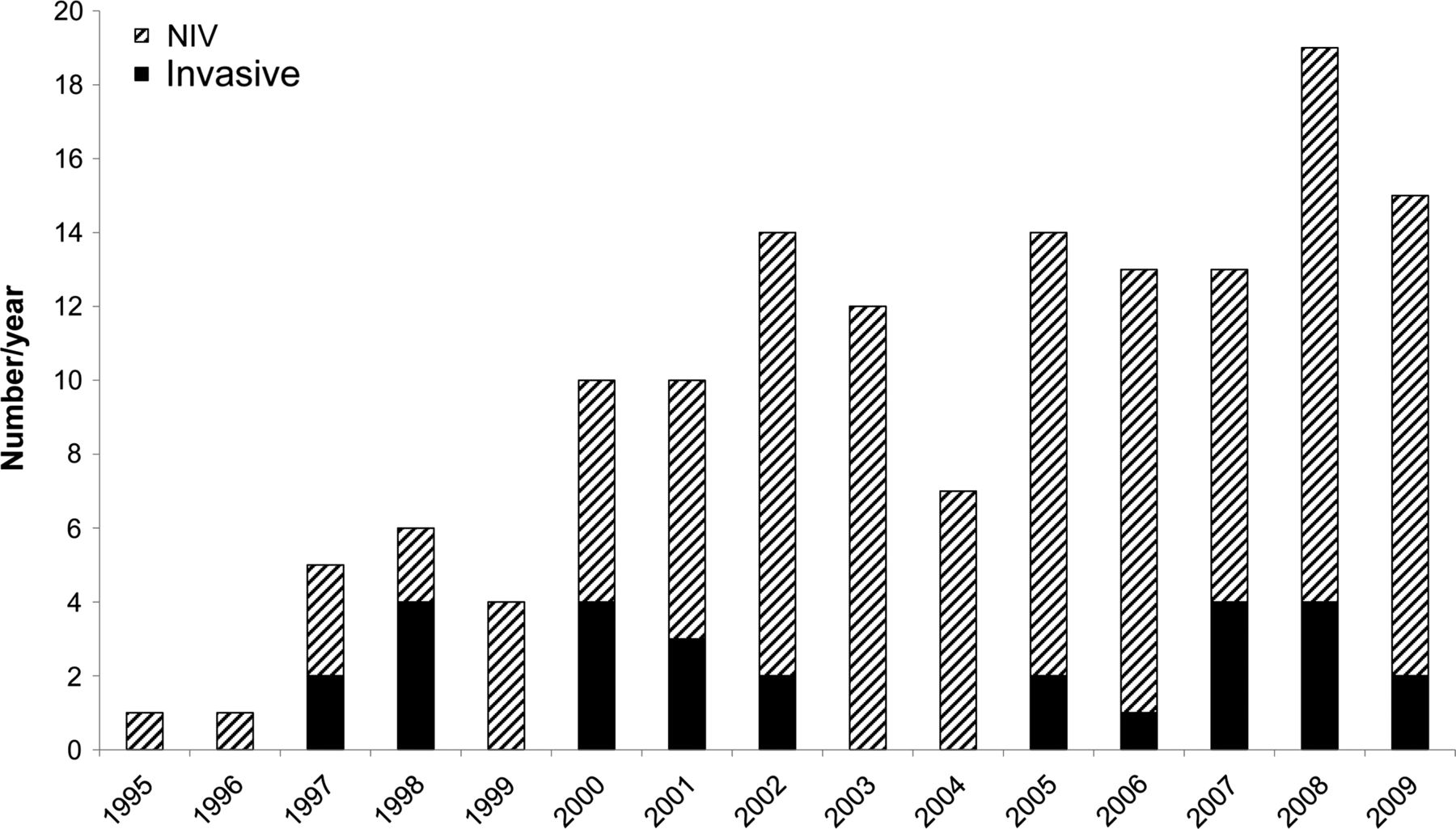
The number of children commencing LTV each year has increased over the 15-year period with an accompanying increase in the total number of children in the LTV service each year (figures 2 and 3). The incidence of LTV increased significantly across the three 5-year epochs (p=0.003, Kruskal–Wallis test), with a median of four (1–6) new patients per year in 1995–1999, increasing to 11 (7–14) new patients per year in 2000–2004 and 14 (13–19) new patients per year in 2005–2009. The increase in annual prevalence was also statistically significant (p=0.002, Kruskal–Wallis test), with a median of 11 (6–18) patients in 1995–1999, 45 (27–57) in 2000–2004 and 74 (70–87) in 2005–2009.

Incidence of long-term ventilation in children 1995–2009. NIV, non-invasive ventilation.

Prevalence of long-term ventilation in children 1995–2009. NIV, non-invasive ventilation.
Census of Canada data reveal that the numbers of young people aged 0–19 years in British Columbia in 1996, 2001 and 2006 were 978120, 976 345 and 953 165, respectively.12 Thus, the incidence rate of LTV in children was 1 per million per year in 1996, 11 per million per year in 2001 and 14 per million per year in 2006. The prevalence of LTV in children in British Columbia increased from 6 per million in 1996 to 37 per million in 2001 and 74 per million in 2006.
Longitudinal trends in mode of respiratory support
There was no significant difference across the three 5-year epochs in the number of children commencing invasive ventilation (p=0.38, Kruskal–Wallis test) (table 1). However, there was a significant increase in institution of NIV over time (p=0.004, Kruskal–Wallis test), with increases in both CPAP (p=0.008) and noninvasive bilevel support (p=0.008).
Details of long-term ventilation (LTV) patients by epoch of initiation of LTV
Longitudinal trends in LTV patient profile
Patients with neuromuscular disease constituted a significantly decreasing proportion of the total number starting LTV over time (χ2 7.9, p=0.02) as the numbers of patients in other diagnostic categories increased (table 1). The age distribution of children commencing LTV did not change across the three epochs (median age 5.7 (0.2–16) years in 1995–1999, 10.2 (0.4–18) years in 2000–2004 and 8.0 (0–18) years in 2005–2009).
Trigger for initiation of ventilation
Information regarding the trigger for initiation of respiratory support was available for 141 patients (table 1).
Outcomes of LTV
Of the 144 children commenced on LTV during the 15-year study period, 68 (47%) remained on LTV in our service on 31 December 2009 (53 (78%) patients on NIV and 15 (22%) children ventilated via tracheostomy). The median duration of respiratory support to date was 3.2 (0.3–12.1) years. Seven (5%) children had died while in our programme, 28 (19%) had discontinued respiratory support and 37 (26%) had transitioned to adult services. One child had moved out of province and three were lost to follow-up.
Six children died as a result of progression of their underlying disease process (three supported non-invasively for SMA and three on 24 h/day tracheostomy ventilation) and one from accidental ventilator disconnection. For the entire cohort, the 5-year and 10-year cumulative incidences of survival were 94% and 91%, respectively. Cumulative survival during childhood was significantly higher for patients on NIV than invasively ventilated patients (Log rank 4.3, p=0.04), with 5-year and 10-year survival rates of 84% and 77%, respectively, for invasive ventilation compared to survival of 97% at both 5 and 10 years for patients on NIV (figure 4). There were no differences in survival between the epochs studied or between the different diagnostic groups.

Kaplan–Meier survival curves for children on invasive ventilation (n=28) and NIV (n=116).
All 28 children who discontinued respiratory support were ventilated for less than 24 h/day, seven with neuromuscular disease, three with spinal injury (low cervical), five with abnormal ventilatory control, five with craniofacial abnormalities/OSA, four with airway malacia and four with other diagnoses. Four (15%) were liberated from tracheostomy ventilation, three of whom continued to require a tracheostomy for upper airway obstruction. The remaining 24 (85%) had been receiving NIV. The median duration of respiratory support prior to discontinuation was 1.9 (0.2–11.5) years. Excluding patients who died, the 5-year and 10-year incidences of liberation from LTV were 21% and 42%, respectively. When patients with neuromuscular disease were compared with all other patients, the cumulative incidence curves of liberation from LTV were significantly different (Log rank 6.5, p=0.01) (figure 5).

Cumulative incidence curves of liberation from long-term ventilation (LTV) for children with neuromuscular disorders (n=62) and other indications for LTV (n=75).
The number of patients transitioned to adult services has increased significantly over time (n=1 in 1995–1999, n=4 in 2000–2004 and n=32 in 2005–2009; p=0.004, Kruskal–Wallis test). The median age at transition was 18.0 (16.4–19.3) years. The number of patients receiving NIV at the time of transition was 32 (87%), while five (13%) were invasively ventilated, two of whom required ventilation 24 h/day.
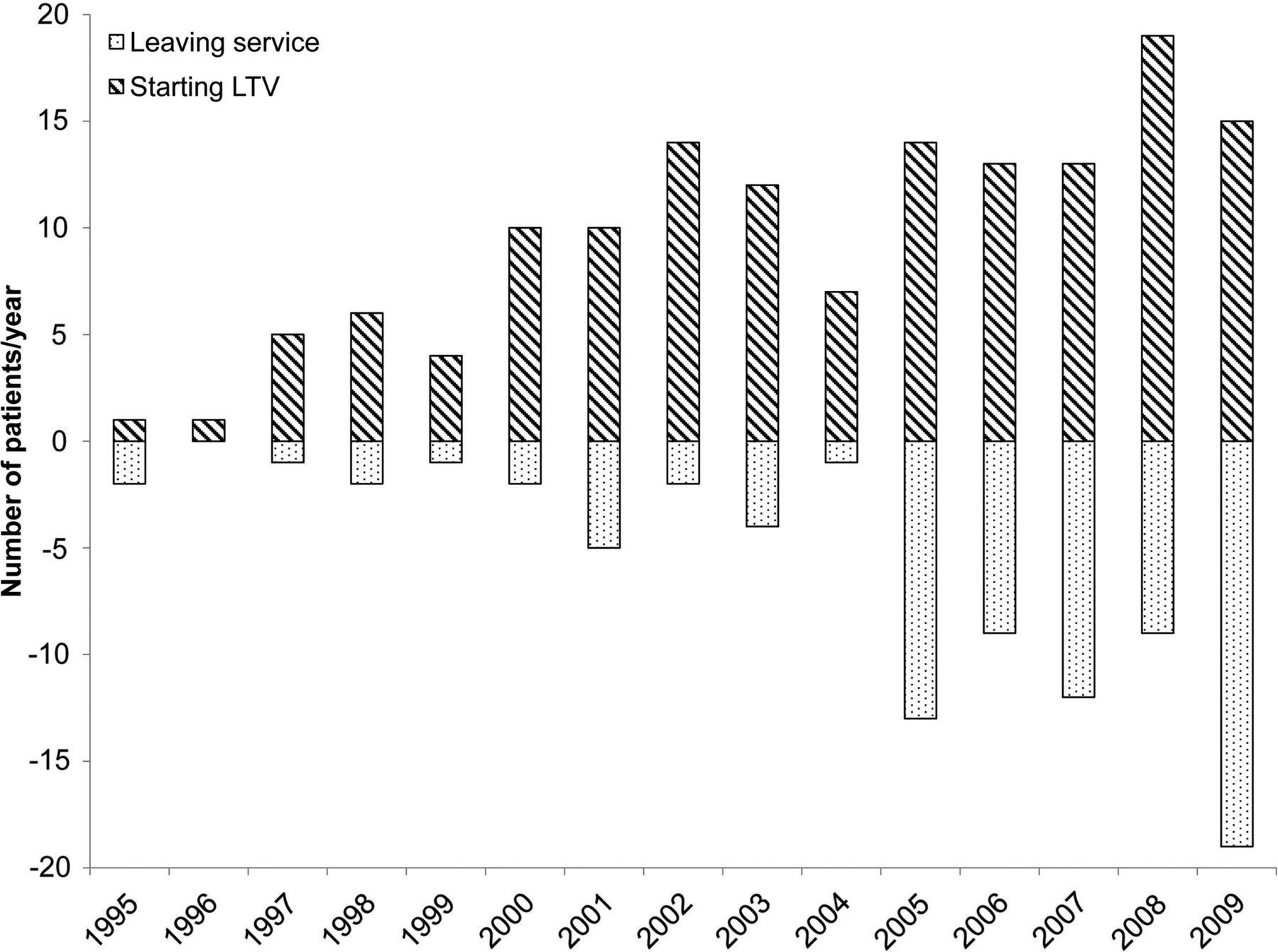
For many years, the number of children commencing LTV greatly exceeded the number leaving the programme. A steady state may have been approached in the last 5 years (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall numbers of patients commencing long-term ventilation (LTV) and leaving LTV service (for any reason) 1995–2009.
Discussion
This study has quantified the expansion of LTV in children suggested by previously published cross-sectional studies. Cross-sectional surveys are often limited by incomplete ascertainment and they do not provide information on outcomes. Our study has the advantages of complete ascertainment from a clearly defined population and provides information on longitudinal trends and outcomes of LTV.
The incidence of LTV in children has increased significantly over the last 15 years, with an accompanying 10-fold increase in prevalence. Cross-sectional surveys6 ,9 and one longitudinal study13 in the UK over a similar time period documented a comparable increase in paediatric LTV. As in the present study, others have reported that the prevalence of invasive ventilation has not changed over time,14 and indeed, the relative proportion of tracheostomy ventilated patients has decreased.9 Rather, the increase in LTV is attributable to an increase in the use of NIV. NIV is now an accepted treatment option for children with sleep-related breathing disorders and has shown convincing benefit for children with neuromuscular weakness in terms of outcomes and patient acceptability.15–17 Overall, LTV is increasingly seen as an acceptable option both by health professionals and by patients and their families. Cumulative survival of these patients contributes to the increase in prevalence. It appears that after a very rapid rise in incidence of LTV in the first half of the last decade, there was a plateauing over the last 5 years. Goodwin et al13 report a similar pattern. Future monitoring is necessary to see whether this trend continues.
This study reports outcomes of paediatric LTV, which have not been widely described previously. Such data are important for both healthcare professionals and families considering LTV for a child. Outcomes of tracheostomy ventilation have recently been reported and reviewed18 and the 5-year and 10-year cumulative survival rates were comparable to our data. In our cohort, the survival of patients on NIV through childhood was very high. The outcomes of patients transitioned to adult services in our study are not known. Our survival data cannot, therefore, be extrapolated to patients commenced on NIV in their teenage years and then transferred to adult care. The 5-year survival rate of young people with hypercapnic Duchenne muscular dystrophy established on nocturnal nasal NIV has previously been reported to be 73%.15 Most of the deaths on LTV were not due to ventilation-related complications. This is consistent with previous reports in which most deaths have been due to progression of the underlying disease or have been unexpected.18 ,19
About one in five children overall were able to discontinue LTV, with the cumulative incidence of liberation continuing to increase even after 10 years. Consistent with previous studies, patients with neuromuscular disorders were less likely to be able to discontinue respiratory support. Rather, patients with lung disease, airway malacia or an upper airway abnormality have the best outlook in terms of discontinuing ventilation.18 ,20 ,21 Larger, probably multicentre, studies would be needed to allow better prediction of outcomes for particular patient subgroups.
It is recognised that there will be considerable variation between centres in the number and profile of LTV patients. Nonetheless, we believe that the trends in paediatric LTV reported here will be seen in all centres. The resource-intensive population of children on LTV is growing, which has significant implications for health services. It is accepted that home environment is preferable to hospital for a child with chronic respiratory failure who needs chronic ventilatory support. This requires provision of homecare packages that are particularly complex for patients on tracheostomy ventilation. The potential barriers to discharge are universal and well documented.11 ,21 ,22 Prolonged hospitalisation has led to concern about hospital beds, particularly paediatric intensive care beds, being blocked.23
Survival through childhood, along with a cohort of young people requiring initiation of respiratory support in their teenage years, has led to a growing number of patients on LTV requiring transfer of their care to adult services. Therefore, transitional programmes are required to ensure smooth transfer to adult services. Physicians for adults will need to become familiar with a range of hitherto unfamiliar childhood disorders, and adult service capacity for long-term care must be developed.
In summary, the incidence of LTV in children has increased significantly over the last 15 years, with an accompanying 10-fold increase in prevalence. The rise in incidence may now be plateauing but prevalence continues to increase because of patient survival. Overall survival is high and, although some children are able to discontinue respiratory support, a growing number are being transferred to adult care. Future planning of paediatric hospitals and community services, as well as adult services, must take into account the needs of this growing population.
References
Footnotes
-
Contributors CMcD, RA, DW and MS conceived and designed the study. The database was maintained by RA. CMcD undertook the analysis and drafted the paper. All authors contributed to and approved the final draft for publication. CMcD is guarantor for the study.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.