Article Text

Abstract
Objective In England, the National Health Service commissioned a National Management Service for children with primary ciliary dyskinesia (PCD). The aims of this study were to describe the health of children seen in this Service and compare lung function to children with cystic fibrosis (CF).
Design Multi-centre service evaluation of the English National Management PCD Service.
Setting Four nationally commissioned PCD centres in England.
Patients 333 children with PCD reviewed in the Service in 2015; lung function data were also compared with 2970 children with CF.
Results Median age at diagnosis for PCD was 2.6 years, significantly lower in children with situs inversus (1.0 vs 6.0 years, p<0.001). Compared with national data from the CF Registry, mean (SD) %predicted forced expiratory volume in one second (FEV1) was 76.8% in PCD (n=240) and 85.0% in CF, and FEV1 was lower in children with PCD up to the age of 15 years. Approximately half of children had some hearing impairment, with 26% requiring hearing aids. Children with a lower body mass index (BMI) had lower FEV1 (p<0.001). One-third of children had positive respiratory cultures at review, 54% of these grew Haemophilus influenzae.
Conclusions We provide evidence that children with PCD in England have worse lung function than those with CF. Nutritional status should be considered in PCD management, as those with a lower BMI have significantly lower FEV1. Hearing impairment is common but seems to improve with age. Well-designed and powered randomised controlled trials on management of PCD are needed to inform best clinical practice.
- primary ciliary dyskinesia
- management
- lung function
- cystic Fibrosis
Statistics from Altmetric.com
What is already known on this topic?
Primary ciliary dyskinesia (PCD) is a rare autosomal recessive condition where abnormal ciliary function leads to impaired mucociliary clearance.
Historically PCD has been considered a mild respiratory condition.
There is little evidence to guide the management of children with PCD, with only one randomised controlled trial published to date.
What this study adds?
In England, forced expiratory volume in one second (FEV1) was lower in children with PCD compared to those with cystic fibrosis, particularly in younger age groups.
Nutritional status should be considered in PCD management, as those with a lower body mass index have significantly lower FEV1.
Hearing impairment is common but seems to improve with age.
Introduction
Primary ciliary dyskinesia (PCD) is a rare autosomal recessive condition where abnormal ciliary function leads to impaired mucociliary clearance. This loss of function to the mucociliary escalator leads to recurrent sinopulmonary infection and, ultimately, bronchiectasis. Historically, it has been considered a mild respiratory condition; however, recent data suggest that lung function declines at a similar rate through childhood to children with cystic fibrosis (CF).1–3 In addition, about 80% of patients suffer with persistent otitis media with effusion and associated conductive hearing loss.4 5 Half of the patients have situs inversus totalis 6 and up to 17% have congenital heart disease (CHD).7 8 Many men are infertile due to immotile sperm and women can have reduced fertility.9 10 The estimated prevalence is 1 in 10 000 live births1 11 but this can be significantly higher in certain populations.12 13
In 2012, National Health Service England commissioned a National Children’s PCD Management Service to complement the existing diagnostic service.14 Four PCD centres were commissioned to undertake annual review assessments, to a standardised service specification, by a specialist PCD multi-disciplinary team (MDT) on all children with PCD in England.
Here, we describe the first full set of data collected from children at annual review, in 2015. We compare the lung function of children with PCD to those with CF in England and identify areas of future research that will help to improve patient care.
Methods
Participants
All children with a diagnosis of PCD who had an annual review assessment between 1 January and 31 December 2015, in one of the four nationally commissioned PCD centres in England were included in this study. The diagnosis of PCD was confirmed by a specialist PCD diagnostic MDT, in line with European Respiratory Society (ERS) consensus guidelines.14 15 Annual reviews were carried out to a standardised service specification.14 16 To ensure that children received similar care across centres, national guidelines were developed, teams met regularly to discuss clinical cases and clinical outcome data were audited. The project was reviewed by the Research and Development office at University Hospital Southampton and was deemed to be a service evaluation hence research ethics committee approval was not required.17
Data collection
Data were extracted from electronic and paper medical records and from annual review reports, using a standardised data sheet, agreed a priori, with variables pre-defined in a coding manual. These included demographics, diagnostic information and a clinical review of the year, focused on respiratory, ear, nose and throat (ENT), and cardiac issues. Also collected were data on treatments, including airway clearance physiotherapy techniques and adjuncts, nebulised mucolytics, antibiotic use (oral and intravenous) both prophylactically and for exacerbations, inhalers and nasal treatments; and anthropometry and investigations, including spirometry, audiometry and collection of an airway microbiology sample. Centres were contacted to clarify any discordant or missing data.
Investigations conducted at annual review assessment
Spirometry data
Equipment was calibrated as per manufacturers’ instructions and all measurements were obtained according to the ERS/American Thoracic Society guidelines.18 Global Lung Initiative (GLI) equations were used to estimate z-scores for forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) from the data, ethnicity-specific equations were used where available.19 GLI-based FEV1 z-scores were obtained from the UK CF Registry for all English children in 2015 for direct comparisons with our PCD FEV1 data.20
Audiology data
Hearing was defined as normal if <20 dB, mild loss if 20–40 dB, moderate loss if 40–70 dB, severe loss if 70–95 dB and profound loss if >95 dB.
Anthropometric data
Height and weight were performed and recorded in accordance with WHO guidelines.21 Body mass index (BMI) z-scores were calculated using the WHO Anthro Plus software V.3.2.2.
Statistical analyses
Data were cleaned, coded and analysed in Stata (V.14.0, Stata Corp, Texas, USA). Continuous variables were presented as mean with SD or median with IQR. Groups were compared using independent t-tests, Mann–Whitney and Kruskal–Wallis tests. Post-hoc for pairwise comparisons were performed for FEV1 % predicted and age categories, with Tukey’s method to adjust for multiple comparisons. Categorical variables were reported as proportions and groups were compared using χ2 or Fisher’s exact test. Multiple regressions were used to model FEV1 z-score, adjusting for possible covariates. Significant (p<0.05) variables were retained (backward selection) and results from the reduced regression model are reported. Normality of residuals was accessed using kernel density estimations and visual inspection of histograms. Results from the models were presented as number of observations, regression coefficients (r) with 95% CIs and model’s goodness-of-fitness (adjusted R2). Spearman’s rank correlation coefficient was used to compare association between variables that were not normally distributed or between continuous and non-continuous variables.
Results
In all, 333 children with PCD underwent an annual review during the study period. Median age at review was 9.8 years, 52.6% of those reviewed were men and the majority were either white British (n=122, 36.6%) or Pakistani and British Pakistani (n=121, 36.3%) (table 1, online supplementary figure 1).
Supplemental material
Clinical and demographic data on children with PCD who underwent an annual review in 2015 across the four English National Children PCD Management Services
Diagnosis of PCD
Median age at diagnosis of PCD was 2.6 years (IQR: 0.5–7.2 years) (table 1). This was significantly lower in those with dextrocardia (n=172) compared with levocardia (n=151) (1.0 year of age (IQR: 0.3–3.2, range: 0–14.0) vs 6.0 years (IQR: 2.0–9.0, range: 0–16.2), p<0.001). 53.3% of children had dextrocardia with almost all having situs inversus totalis, only 12 patients (3.7%) had dextrocardia in isolation. CHD was reported in 13.1% of children spirometry.
Mean (SD) FEV1 z-scores for children with PCD were −1.9 (1.4) and FVC z-scores were −1.3 (1.5), mean predicted FEV1 (SD) was 76.8% (table 1). FEV1 z-score was significantly lower in older children, with a decrease of 0.6 z-scores for every increase of 10 years in age (n=240, regression coefficient=−0.06, 95% CI −0.11 to −0.02, p=0.008, adjusted R2=2.9%; figure 1a), adjusted for centre of origin, age at diagnosis, sex, cardiac situs and presence of cultured pathogens (online supplementary table 1). Spirometry data from children with CF in 2015 were available as predicted FEV1 and hence this was used for comparison with our patients with PCD.20 Mean predicted FEV1 was significantly lower in PCD children compared with CF children up to the age of 15 years (p=0.001), with no difference seen in the 16- to 18-years-old category (p=0.7). The largest difference was in the 5- to 7-year olds, where the mean predicted FEV1 was 91.3% (SD=15.7%) in CF but was 78.3% (SD=18.6%) in PCD (figure 1b).20

a) Age (years) versus FEV1 z-score for 240 children with PCD in 2015. (b) Mean (95% CI) % predicted FEV1 of 240 children with PCD versus 2970 children with CF in England in 2015, stratified by age group (20), (c) BMI z-score versus FEV1 z-score for children with PCD in 2015. BMI, body mass index; CF, cystic fibrosis; FEV1, forced expiratory volume in one second; PCD, primary ciliary dyskinesia.
Mean (SD) BMI z-scores in children with PCD were normal (z-score=0 (1.4)) (table 1). However, children with lower BMI also had lower FEV1 z-scores (n=238, regression coefficient=0.35, 95% CI: 0.22 to 0.47, p<0.001, adjusted R2=10.8%) (figure 1c).
Microbiology
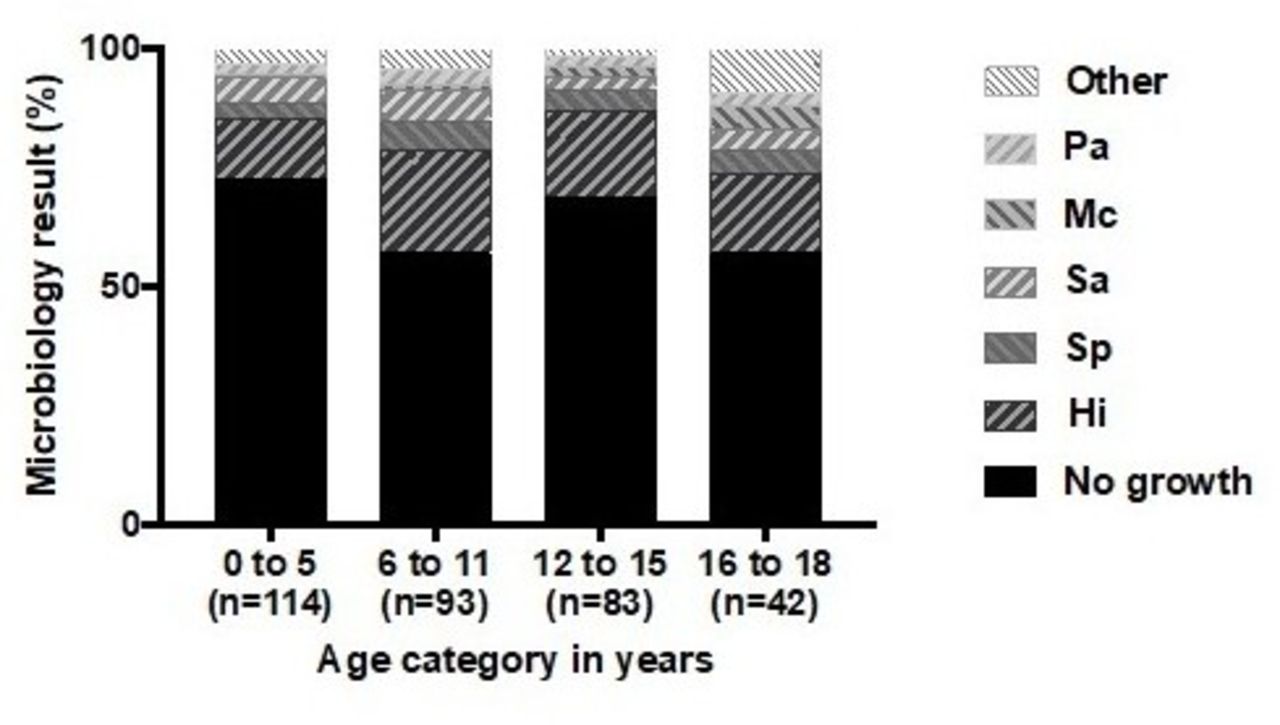
Microbiology data were available for 312 children, of which 67% did not culture a respiratory pathogen at annual review. Haemophilus influenzae was the most prevalent pathogen (17.9%, corresponding to 53.9% of those with a positive culture), followed by Staphylococcus aureus (5.1%) and Streptococcus pneumoniae (4.2%), with Pseudomonas aeruginosa cultured in 2.6% of children (online supplementary table 2). No children cultured non-tuberculous mycobacterium. There was no correlation between those culturing respiratory pathogens and FEV1 z-scores and no statistically significant differences were observed in respiratory pathogens when stratified by age category (figure 2).

Microbiology results taken at annual review by percentage, stratified by age category. HI, Haemophilus influenzae; MC, Moraxella catarrhalis; PA, Pseudomonas aeruginosa; SA, Staphylococcus aureus; SP, Streptococcus pneumoniae.
Audiology
Normal hearing levels were observed in 44.3% of children with audiology results available (n=271; 81.4% of all children), 34% had mild hearing loss and 21.8% had more significant hearing loss. At the time of annual review, 23.6% of children were wearing hearing aids. Moderate to profound hearing loss was seen in 26.4% of children younger than 6 years of age but in only 13.8% of those aged between 16 and 18 years (figure 3). Once the children were under the care of the National Children’s PCD Management Service, only two of the 333 children had ventilation tubes inserted.

{kind=link}
{kind=link}
{kind=link}
Proportion of children with PCD with varying degrees of hearing loss in different age groups in 2015. PCD, primary ciliary dyskinesia.
Physiotherapy and mucolytic nebulisation
All children were trained to perform, and advised to undertake, regular age-appropriate airway clearance physiotherapy. The majority used either oscillating positive expiratory pressure (PEP) (49.2%) or PEP physiotherapy (32.1%) (table 2). Approximately half of children (53.2%) were prescribed nebulised hypertonic saline as a mucolytic agent to aid airway clearance. Children using hypertonic saline had significantly lower FEV1 z-scores (mean difference −0.4, 95% CI −0.76 to −0.04, p=0.028). Nebulised Dornase Alpha (Pulmozyme, Genentech, San Francisco, USA) was used in only 4.9% of children.
Management of children with PCD in England in 2015
Antibiotics
Thirty per cent of children with PCD had at least one courses of intravenous antibiotics over the preceding 12 months. Approximately 10% of the children were prescribed regular intravenous antibiotics (table 2). Those that received intravenous treatment had a lower FEV1 z-score, adjusted for BMI z-score and age (n=234, regression coefficient=−0.52, 95% CI: −0.88 to −0.16, adjusted R2=17.5%). Children received a median of two courses of oral antibiotics over the preceding year (IQR: 1–3). 59% were prescribed prophylactic antibiotics and of these, over half used Azithromycin (59.8%) (table 2, online supplementary table 3). A significantly lower mean FEV1 z-score was found in children taking prophylactic antibiotics, adjusted for use of antibiotics in the last year (intravenous or oral) and cultured pathogens (n=162, regression coefficient: −0.66, 95% CI: −1.23 to −0.08, p=0.0008, adjusted R2=8.3%).
Discussion
This study provides detailed characterisation of a large and well-defined group of children with PCD, diagnosed and managed under the unified, specialised National Children's PCD Management Service in England.
Historically, PCD has been considered a mild respiratory condition22; however, we report a mean FEV1 of −1.9 z-scores in children with the disease in England. Almost a third of children required admission for intravenous antibiotics over the preceding 12 months with over 10% receiving regular intravenous antibiotics. Further to this, while a recent large international PCD cohort found a similar reduction in lung function between children with PCD and CF, we showed that % predicted FEV1 was significantly lower in those with PCD compared with those with CF up to the age of 15 years, as was also observed in a smaller Danish cohort study.2 3 23 This suggests that in 2015, younger children seen by the National Children’s PCD Management Service had lower lung function than their European counterparts. However, lung function decline over time was steeper in patients with CF and, by the age of 16 to 19 years, no statistically significant difference was seen between the two groups.
Our children had a median age at diagnosis of 2.6 years. This is considerably younger than previously reported in the literature,24 suggesting that the establishment of National Children’s PCD Diagnostic Service in 2006 and Management Service in 2012 might have raised awareness of this rare disease among paediatricians. However, newborn screening for CF was introduced in England in 2007 meaning that CF is generally diagnosed in infancy, allowing for early initiation of treatment. When comparing the spirometry data of our PCD children to those with CF, the largest differences in mean FEV1 were in younger children (figure 1b). We therefore hypothesise that earlier diagnosis and initiation of treatment for PCD may improve the low values of FEV1 observed in younger children.
Haemophilus influenzae, as reported in previous studies, was the most frequent respiratory pathogen cultured in our patients.25 26 Future studies clarifying the impact of chronic colonisation with this and other pathogens such as Pseudomonas aeruginosa in patients with PCD are needed. While these are cross-sectional data, we found no association between any cultured pathogen and FEV1. Well-powered longitudinal studies will be required to understand the impact of these pathogens on patients and, thereby, inform clinicians as to whether they should persist in attempting to eradicate them. Contrary to previous publications, the prevalence of respiratory pathogen did not vary between age groups, in particular there was no increase seen in the prevalence of Pseudomonas aeruginosa in older age groups.27
A recently published large international cohort of children with PCD28 29 found that patients with lower BMI z-scores have lower FEV1 z-scores, which had not been observed previously.30 Our findings support this novel observation and are similar to well-described correlations in children with CF.31 However, the majority of patients with CF have pancreatic insufficiency, which is not the case in PCD. This would therefore imply that having suppurative lung disease, independent of pancreatic issues, may impact negatively on nutritional status (or vice versa). These findings lead to the hypothesis that intervening on nutritional status may have a positive benefit on the respiratory health of children with PCD, as is the case in CF,32 and warrants further investigation.
Management of children with PCD is challenging due to the limited evidence base, with only one published randomised control trial (RCT) to date.33 Management is therefore based on expert opinion, consensus guidelines and extrapolated from the larger evidence base available for patients with CF.15 34 35
All children in the service were advised to undertake regular airway clearance physiotherapy.36 Over half the children used nebulised mucolytics agents, the vast majority using hypertonic saline. A RCT on use of hypertonic saline in PCD did not show improvement on quality of life in patients compared with controls33; however, the study did not use a disease-specific quality of life questionnaire, was underpowered and the control group received normal saline nebulisation, which might in itself have been beneficial for the patients.37 We found that children on hypertonic saline had a significantly lower FEV1 than those not. This is likely due to clinicians reserving its use for children with a more severe clinical phenotype; however, further research is needed to exclude the possibility that hypertonic saline has a negative effect on lung function in children with PCD.
The use of prophylactic antibiotics in PCD remains controversial, as the potential decrease in the number of respiratory exacerbations must be balanced against the risk of increasing antimicrobial resistance. Despite this, in 2015, approximately 60% of our children were on prophylactic antibiotics, with over half of these using Azithromycin. These children were noted to have significantly lower FEV1 than those not on antibiotics. Again, clinicians likely reserved the use of prophylactic antibiotics for more severe, or frequently exacerbating children. Results from a multicentre study assessing the use of prophylactic azithromycin in PCD should soon be available and will help inform future management.38
Almost a quarter of our children needed hearing aids for moderate to profound hearing loss. Hearing seems to improve with age but the high proportion of patients with some level of hearing loss stresses the importance of regular hearing assessments and ENT follow-up, particularly in early childhood, when hearing is fundamental to speech development. Only 2 out of 333 children in this study had ventilation tubes inserted under the care of the Service. The limited evidence for their use is both inconclusive and conflicting and a well-designed and powered study is needed to investigate this important area of management.39–42
The strength of this work is in the large number of well-characterised children with PCD evaluated under a nationally standardised Management Service. However, the data are cross-sectional and therefore do not allow for conclusions to be drawn on, for example, the potential benefits of therapeutic interventions or the detrimental impact of culturing particular pathogens on clinical outcomes. Detailed longitudinal follow-up of these children are therefore required and will help inform both management guidelines and therapies to be evaluated in future RCTs. Comparisons of lung function data between children with PCD and CF were limited to the data provided by the UK CF Registry (ie, GLI-based spirometry measurements) and we were therefore unable to adjust CF data for potential confounders.
Conclusions
Our data suggest that, far from being a mild respiratory condition, children with PCD have worse lung function than those with CF, particularly at an earlier age. Those with a lower BMI have a significantly lower FEV1; therefore, nutritional status should be considered in their management. Well-designed and powered RCTs on the management of PCD are needed to inform best clinical practice.
Acknowledgments
We would also like to thank all our shared care centres, our patients and the UK PCD Family Support Group.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Members of the English National Children’s PCD Management Service include: Amanda Harris, Amanda Friend, Victoria Keenan, Hannah Wilkins, Hasnaa Ismail-Koch, Andrea Burgess, Samantha Packham, Patricia Goggin, Gemma Marsh, Laura Baynton, Michael Leshen, Sarah Ollosson, Nicola Collins, Peter Rea, Ann-Louise McDermott, Amanda Parsons, Rajinder Kang, Nicola Lloyd, Alison Truscott, Lynne Schofield, l Knight.
Contributors WW, JSL, SC, CH, PC, EM, MN, PK, CO’C and MW developed the concept and design of the study. WW and BR are responsible for the integrity of the study and data; BR led standardised clinical data collection, data management and statistical analyses; WW and BR drafted the manuscript; SB, BR, SC, PK, PC, EM, RH, AS, PG, MN and WW extracted of clinical data from patient record; WW, JSL, SC, CH, PC, EM, MN, PK, CO’C and MW led the diagnostic service and annual reviews at their respective centres; JSL provided guidance and critically reviewed the manuscript at an early draft. All co-authors critically reviewed and approved the final manuscript.
Funding The National PCD Service is commissioned and funded by NHS England. Research in Southampton is supported by NIHR Southampton Biomedical Research Centre and NIHR Wellcome Trust Clinical Research Facility. Research in Royal Brompton Hospital is supported by the NHLI, Imperial College London. Research in GOSH is supported by the NIHR GOSH BRC. Research in the University Hospitals of Leicester NHS Trust is supported by University of Leicester, Leicester. Research in Birmingham Women’s and Children’s Hospital NHS Trust is supported by the University of Birmingham and Wellcome Trust Clinical Research Facility.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests JL reports grants, personal fees and non-financial support from Aerocrine/ Circassia, grants and personal fees from Vertex, grants from Parion, outside the submitted work. SC reports grants, personal fees and non-financial support from Vertex Pharmaceuticals, grants and other from Chiesi Pharmaceuticals, other from Pharmaxis Pharmaceuticals, personal fees from Actavis Pharmaceuticals, other from Profile Pharma, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data will be made available upon reasonable request by contacting the corresponding author.