Article Text

Abstract
Objective To report the population-based, gestational age (GA)-stratified mortality and morbidity for very preterm infants over 13 years in Switzerland.
Design A prospective, observational study including 95% of Swiss preterm infants (GA <32 weeks) during three time periods: 2000–2004 (P1), 2005–2008 (P2) and 2009–2012 (P3).
Setting The Swiss Neonatal Network, covering all level III neonatal intensive care units (NICUs) and affiliated paediatric hospitals.
Patients 8899 live-born preterm infants with GA <32 weeks.
Main outcome measures Trends in GA-specific mortality (overall, delivery room and NICU), ‘survival free of major complications’ and major short-term morbidities: bronchopulmonary dysplasia (BPD, oxygen requirement at 36 weeks), grades 3 and 4 intraventricular haemorrhage (IVH 3–4), necrotising enterocolitis (NEC) and cystic periventricular leukomalacia (cPVL).
Results Survival rate was 84.4%; 5.7% died in the delivery room and 9.9% died in the NICU. Neonatal mortality was 8.6% and post-neonatal mortality in NICU admissions was 1.3%. Reductions were observed in overall mortality from 18.4% (95% CI 17.0% to 19.8%) in P1 to 13.8% (13% to 15%) in P3, NICU mortality from 12.6% (11.4% to 13.8%) to 8.2% (7.2% to 9.2%) and IVH 3–4 from 7.8% (6.8% to 8.7%) to 5.8% (4.9% to 6.6%). There was no change in the incidence of cPVL and NEC. The BPD (oxygen requirement at 36 weeks) incidence displayed a U-shaped distribution across the three time periods. Overall, 71.0% (70.0% to 72.0%) had ‘survival free of major complications’ at the time of hospital discharge, and this significantly improved from 66.7% (65.0% to 68.4%) to 72.4% (70.8% to 74.0%) between P1 and P3.
Conclusions Survival rates of very preterm infants increased with decreasing delivery room and neonatal mortalities, mostly in extremely preterm infants. The incidence of IVH 3–4 decreased, whereas the incidences of cPVL, NEC and BPD (oxygen requirement at 36 weeks) remained largely unchanged from 2000 to 2012 in Switzerland.
- Neonatology
- Mortality
- Epidemiology
- Pathology
- Qualitative research
Statistics from Altmetric.com
What is already known on this topic
The survival rate for preterm infants is continuously increasing.
The relationship between morbidity and mortality of preterm infants is different in regions and countries.
What this study adds
Improvement of mortality has shifted towards younger infants in recent years.
Morbidity rates may increase with decreasing mortality of the youngest preterm infants.
The bronchopulmonary dysplasia rate may present a sensitive marker of increasing morbidity and a target for further improvement.
Introduction
Preterm births account for 10% of births in the USA and 5%–7% of births in European countries.1–3 Prematurity remains the single most important factor influencing an infant's subsequent survival and health outcome.4 Mortality and morbidity data of preterm infants are indicative of trends in the field of neonatology and obstetrics; they reflect improvements in overall patent management.5 Outcomes are strongly dependent on gestational age (GA), but most published data summarise outcomes for larger and thus inhomogeneous groups, such as very preterm or extremely preterm infants. Up-to-date and reliable, population-based, longitudinal and GA-stratified data are essential for sound clinical decision-making and objective counselling of parents during the perinatal period.
In the years 2000–2004, reported survival from the Swiss Minimal Neonatal Dataset was 81% for infants <32 weeks GA, with a weekly incline along with increasing GA (5% at 23 weeks to 97% at 31 weeks).6 A second national study comparing survival data of infants with a GA of 25 completed weeks showed a significant improvement of survival from 42% in 2000–2001 to 60% in 2003–2004, but then remained unchanged at 63% over the next 5 years (2005–2009).7
As more evidence becomes available that mortality and morbidity rates in preterm infants are decreasing, it is important for parent counselling and healthcare decision-makers alike to understand nationwide data, particularly as the incidence of short-term morbidities may not follow decreasing mortality and may even increase.6–12 Nationwide longitudinal data that include morbidities are hard to come by. The current study reports the trends of GA-stratified mortality, delivery room mortality, neonatal intensive care unit (NICU) mortality and short-term morbidities as well as ‘survival free of major complications’ at dismissal of all preterm Swiss neonates with a GA <32 weeks over a 13-year period from 2000 to 2012.
Methods
This was an observational study based on prospectively collected data from the Swiss Neonatal Network, and covered 95% of the preterm population in Switzerland compared with the Swiss Birth Registry.13 Switzerland's population is largely of Caucasian ethnicity.6 Live-born preterm infants in Switzerland with GA between 23 0/7 and 31 6/7 weeks were recorded between 1 January 2000 and 31 December 2012, including newborns with malformations.
The Swiss Neonatal Network includes nine level III centres and six level II centres (see collaborators at the end of the paper). Participating centres prospectively collect data on all live-born babies born below 32 weeks GA. Data collection, gathered in paper form or electronically, is monitored for population coverage, dataset completeness, plausibility and reliability by a data manager, and since 2006 is in addition submitted to an automatic plausibility testing at entry.
Missing data comprises 5% of patients that were neither delivered nor transferred to a participating centre. GA was based on the first day of the last menstrual period and confirmed by a first trimester ultrasound. The following reported major short-term morbidities, defined in detail in the previous study,6 have been analysed: moderate/severe bronchopulmonary dysplasia (BPD) defined as supplemental oxygen requirement and/or positive pressure support at 36 weeks postmenstrual age, grades 3 and 4 intraventricular haemorrhage (IVH 3–4), necrotising enterocolitis (NEC) Bell stage II or higher14 and cystic periventricular leukomalacia (cPVL). Overall mortality was defined by all deaths that occurred after birth, further specified into delivery room and NICU deaths. NICU mortality was further subdivided into neonatal mortality (<28 days) and post-neonatal mortality (≥28 days). ‘Survival free of major complications’ required survival of NICU stay and absence of any of the following short-term complications: BPD (oxygen requirement at 36 weeks), IVH 3–4, NEC and cPVL. Mortality and ‘survival free of major complications’ refer to all infants, whereas specific morbidities refer only to infants admitted to the NICU. A mother was considered to have received antenatal steroids if at least two doses (full course) within a 24 h interval were administered, with the last dose administered >24 h before birth. Inborn was defined as an infant delivered in one of the participating Swiss centres. Small for GA (SGA) was defined as a birth weight (BW) less than the 10th percentile for GA and major congenital malformation as a lethal malformation or a malformation requiring a specific therapeutic intervention during the neonatal period.
The longitudinal trend was analysed using comparisons between cohorts from three different continuous time periods: period 1 (2000–2004, P1); period 2 (2005–2008, P2); period 3 (2009–2012, P3).
Ethics
Data collection and evaluation for this study were approved by the Swiss Federal Commission for Privacy Protection in Medical Research. Participating units were obliged to inform parents about the scientific use of the de-identified data.
Statistical analysis
Rates are presented as percentages with 95% CIs. Categorical variables were analysed with either χ2 or Mann–Whitney test, as appropriate. GA and BW were treated as continuous variables, reported as medians with IQR, and compared with Kruskal–Wallis test. A multivariable logistic regression model for the outcomes of interest including survival rate, ‘survival free of major complications’ and morbidities was performed to estimate the adjusted OR (aOR) with 95% CI by entering the following variables into a stepwise regression analysis: multiple birth, female gender, SGA, major congenital malformation, antenatal corticosteroids, inborn, weekly GA stratum (as a categorical variable) and time period. The Hosmer–Lemeshow test was used to assess the goodness-of-fit. A significance level of 0.01 was used and was not changed for multiple comparisons. SPSS was used for statistical analysis (V.18.0, IBM, Chicago, USA).
Results
Over the 13 years, from 2000 to 2012, there were 987 062 consecutive live births in Switzerland,15 of which 8899 (0.9%) were born extremely preterm or very preterm, and were included in our analysis (n=3064 during P1 (2000–2004); n=2767 during P2 (2005–2008) and n=3068 during P3 (2009–2012). A total of 8394 (94.3%) preterm infants were admitted to a NICU. For overall mortality, delivery room mortality and NICU mortality, there were no missing values. Missing values for cPVL, IVH, BPD (oxygen requirement at 36 weeks) and NEC were all below 1%. Birth characteristics are presented in table 1.
Characteristics in infants born alive, n (%)
Median GA, BW, female gender and SGA remained similar throughout the 13-year period. Multiples increased as did the use of antenatal corticosteroids and the proportion of inborns. The percentage of caesarean deliveries increased from P1 to P2 before decreasing marginally in P3, and the percentage of major congenital malformations presented a similar trend. The proportion of low Apgar scores at 1 min and 5 min increased across all three time periods.
Mortality
During the 13-year period, from 2000 to 2012, 1384 (15.6%) infants died, 505 (5.7%) of which in the delivery room (table 2). Delivery room mortality for infants <32 weeks GA did not change between time periods, except for the 25 weeks GA stratum (P1: 12.3% vs P3: 3.9%, p<0.01) (figure 1). The sum of neonatal and post-neonatal mortalities amounted to an average of 9.9% (9% to 11%). Neonatal mortality decreased from 11% (10% to 12%) in P1 to 6.7% (6% to 7%) in P3, while post-neonatal mortality remained unchanged in the trend analysis. Mortality for males was higher than for females (16.0% vs 15.0%, p<0.05). Between 24 and 28 weeks, overall mortality continuously and significantly decreased by 14.5% per additional GA week or 2% daily.
Rates of survival, ‘survival free of major complications,’ delivery room mortality and NICU mortality by gestational weeks, n(%)

Mortality and survival free of major complications. *Comparison between 2000–2004 and 2005–2008, p<0.01. +Comparison between 2005–2008 and 2009–2012, p<0.01. #Comparison between 2000–2004 and 2009–2012, p<0.01. GA, gestational age.
Morbidities
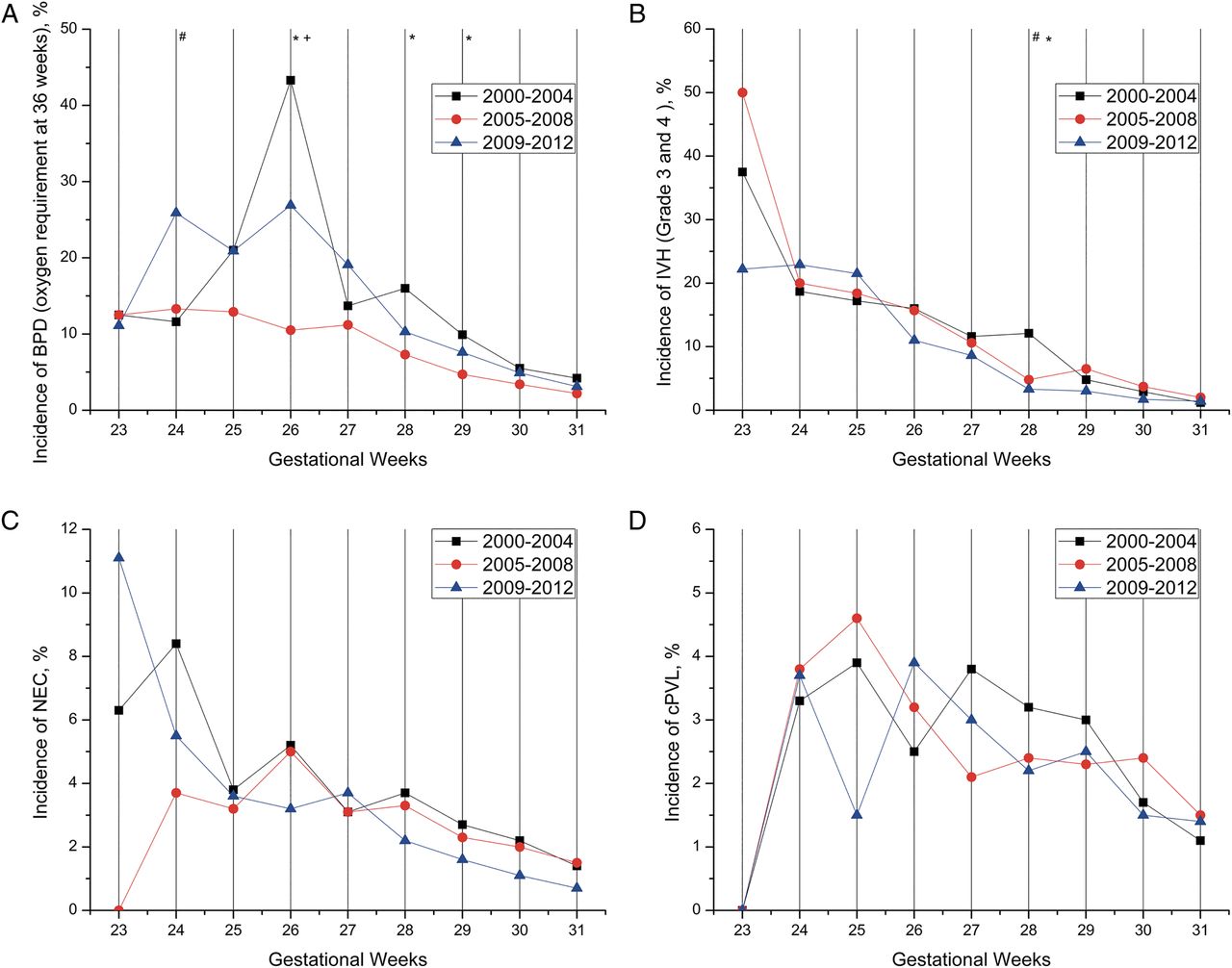
The overall incidences of the major morbidities were 6.9% (95% CI 6.3% to 7.4%) for IVH 3–4, 2.3% (2.0% to 2.7%) for cPVL, 2.5% (2.2% to 2.9%) for NEC and 9.5% (8.9% to 10.1%) for BPD (oxygen requirement at 36 weeks). One or more of these four major morbidities were observed in 15.8% of survivors. Figure 2 illustrates individual morbidity rates stratified by GA for the three time periods.
{kind=link}
{kind=link}
Bronchopulmonary dysplasia (BPD), intraventricular haemorrhage (IVH), necrotising enterocolitis (NEC) and cystic periventricular leukomalacia (cPVL) by gestational age week. *Comparison between 2000–2004 and 2005–2008, p<0.01. +Comparison between 2005–2008 and 2009–2012, p<0.01. #Comparison between 2000–2004 and 2009–2012, p<0.01.
The rate of IVH 3–4 showed a reduction over the 13-year period, with a significant difference between P1 and P3. There was no notable change for cPVL and NEC between the three time periods. The BPD (oxygen requirement at 36 weeks) incidence decreased from 11% (10.0% to 12.3%) in P1 to 6.1% (5.2% to 7.1%) in P2, but increased again to 10.9% (9.8% to 12.1%; p<0.001) in P3. Among infants with more than one of the morbidities, BPD (oxygen requirement at 36 weeks) was the most common complication; this association of BPD (oxygen requirement at 36 weeks) with another morbidity occurred in 78.9% (306/388) in P1, 56.2% (154/274) in P2 and 82.5% (298/361) in P3; p<0.001.
Survival free of major complications
The overall incidence of ‘survival free of major complications’ was 71.0% (95% CI 70.0% to 72.0%), and for NICU admissions excluding delivery room deaths it was 75.3% (95% CI 74.3% to 76.2%), with 70.8% (69.1% to 72.5%) in P1, 78.7% (77.1% to 80.2%) in P2 and 76.8% (75.2% to 78.3%) in P3 (p<0.05) (figure 1 and table 2). ‘Survival free of major complications’ increased from 2.4% at 23 weeks GA to 64.5% (61.4% to 67.6%) at 27 weeks GA and 90.7% (89.5% to 92.0%) at 31 weeks GA, with an average improvement of 11% per additional week.
Influence of prenatal factors on major morbidities
Table 3 displays the odds of the major morbidities when adjusted for potential confounders. When stratified by time period, the aOR for mortality compared with P1 was 0.67 (95% CI 0.56 to 0.80) in P2 and 0.68 (0.57 to 0.82) in P3; the aOR of ‘survival free of major complications’ was 1.59 (1.38 to 1.82) in P2 and 1.33 (1.16 to 1.51) in P3.
Multivariable logistic regression model for clinical variables associated with morbidities
In the multivariable analysis, the odds for survival were increased for female gender (aOR: 1.17; 95% CI 1.0 to 1.4), antenatal corticosteroids (2.14; 1.84 to 2.49), additional GA week (1.94; 1.87 to 2.01), increasing time period (1.21; 1.11 to 1.33), and odds were decreased for SGA (0.32; 0.26 to 0.40) and major congenital malformations (0.08; 0.07 to 0.11).
The odds for ‘survival free of major complications’ were increased for female gender (aOR: 1.31; 95% CI 1.17 to 1.46), antenatal corticosteroids (1.41; 1.28 to 1.61), additional GA week (1.68; 1.63 to 1.72), increasing time period (1.16; 1.63 to 1.72), and odds were decreased for SGA (0.34; 0.28 to 0.40) and major congenital malformations (0.17; 0.13 to 0.21).
Discussion
Our study analysed the trends in mortality, short-term morbidities and the chances of ‘survival free of major complications’ in a large national cohort over 13 years.
Population-based studies highlight time-sensitive trends in mortality and morbidity. In this nationwide, population-based observational study, we found a significant increase in overall survival and ‘survival free of major complications’ for very preterm infants compared across the three time periods, mainly in younger GA strata. Available studies on outcomes of very preterm infants have reported varying results on survival and related major short-term morbidities. The EPICure study reported a decrease in mortality from 60% to 47% of infants at 22–26 weeks GA between 1995 and 2006, while the proportion of affected survivors remained unchanged.16 The EPIBEL and Norway studies revealed more than 50% mortality and almost 50% of moderate-to-severe disability in surviving premature infants below 26 weeks gestation.17 ,18 During a similar time period, the US NICHD Neonatal Research Network reported unchanged mortality among infants born before 27 weeks, between 2003 and 2007.19 Over a longer period from 2000 to 2009, another NICHD study found a decrease in mortality for infants weighing 501–1500 g from 14.3% to 12.4%, but major morbidities remained high in 41.4% of survivors in 2009.20
In our study on three time periods from 2000 to 2012, overall survival rate increased significantly by 4.6%. The improvement of survival rate can predominantly be attributed to infants below 28 weeks GA, suggesting an improved or changed management of these extremely preterm infants.9 ,11 ,21
At 23 weeks GA, considered at the lower limit of viability in 2002,9 mortality was 95%, with most deaths occurring in the delivery room, and there was little or no change over this 13-year time period. Swiss national recommendations for perinatal care at the limit of viability were first published in 2002 and updated in 2011,9 so that it can be safely admitted that the latest recommendations only marginally influenced the currently presented data. The earlier recommendations cautioned against resuscitation below 24 weeks GA.9
Between 24 and 28 weeks GA, our study showed a decrease in mortality between P1 and P3. This change was inconsistent during the middle time period, matching an earlier report by Berger et al7 on data between 2005 and 2009. The GA strata and place of death are consistent with the trend to resuscitate infants born ≥24 weeks GA and appear to be in accordance with the Swiss guidelines.9 The high delivery room mortality at 24 weeks and below reveals withholding of care and mirrors the perceived value balance of the Swiss population and perinatal community, whether the limited chances of morbidity-free survival justify the burden of obstetric interventions and neonatal intensive care. We speculate that improvements after 24 weeks GA are related to more optimistic international attitudes regarding life-saving interventions in extremely preterm neonates, leading to the update of the 2002 Swiss guidelines in 2011.9
The odds for survival were higher for female gender and increasing weekly GA across the three periods. The improved survival of the smallest preterm infants also correlated with an increased use of antenatal corticosteroids.22–24 In the present study, we detailed the full courses of antenatal steroids that increased significantly. Any steroids before birth were given in 6763/8872 (76.2%), and similarly increased from 64.4% in P1 to 86.4% in P3. Antenatal corticosteroids were indeed a main independent factor associated with a reduced mortality by a factor of 2 across the three time periods.
More than two-thirds of the Swiss very preterm infants survived free of major complications, a number that increased significantly over the time periods. The incidence of IVH 3–4 decreased; cPVL and NEC remained largely unchanged. Among all neonatal morbidities, only BPD (oxygen requirement at 36 weeks) increased with increasing survival of the most immature infants in the last study period.
Data from the Vermont Oxford Network 2010 showed a variable incidence of BPD (12%–32%) among infants born <32 weeks gestation.25 In our Swiss population, the incidence of BPD (oxygen requirement at 36 weeks) was below 10%. BPD (oxygen requirement at 36 weeks) is considered a common adverse outcome of prematurity and an important predictor of late outcomes for respiratory disease and in terms of neurodevelopment. The incidence of BPD (oxygen requirement at 36 weeks) in our study displayed a U-shaped distribution over time with the lowest rates in P2. The increased survival from P1 to P3 mostly concerned the youngest infants with the highest risk of BPD (oxygen requirement at 36 weeks), and may explain its significant re-increase in P3 compared with P2. Similarly, one study from the Japanese neonatal network confirmed improved neonatal survival without improvement in chronic lung disease (CLD).24 The NICHD Neonatal Research Network also failed to show a significant improvement in CLD between 2000 and 2009.20 The low Swiss BPD (oxygen requirement at 36 weeks) rates may also result from early ventilation strategies.
A paradox in our findings is the association between the increased use of antenatal steroids and an increased BPD rate in the most recent period. In 1995, Crowley's meta-analysis also concluded that although antenatal steroids decreased the incidence of respiratory distress syndrome (RDS) by about 50%, they had little impact on BPD.26 In the presence of threatening preterm delivery, foetal lung maturation with antenatal corticosteroids was recommended from 24 0/7 weeks of gestation in Switzerland,9 similar to other recommendations.27 ,28 Our work and the NICUs network of Australia report a similar and significant increase in BPD or CLD in extremely premature infants after or despite prenatal steroids.29 Given these observations, it becomes necessary to better explore the association between antenatal corticosteroids and BPD (oxygen requirement at 36 weeks) as well as long-term respiratory morbidities.
The incidence of severe IVH 3–4 in Switzerland (5.8% in P3) compares closely with the NICHD data with an incidence of 6.2% severe IVH in 2000 and 6.1% in 2009 among infants from 501 to 1500 g.20 In our GA-stratified cohort, the decrease in IVH 3–4 mainly occurred for the age group ≥26 weeks GA and could not be demonstrated for infants <26 weeks GA, for which age group the incidence even showed a non-significant increasing trend in P3. The decreased mortality rates at the lowest GAs were inversely related to the increased rates of IVH 3–4, and may present the consequence of improved survival rates in the most immature and highly vulnerable infants requiring considerable intensive care measures.
No significant change in the incidence of cPVL was noted during the observed time periods, overall or for specific GA strata. However, in the multivariable analysis, increasing weekly GA reduced the odds of cPVL, as shown by others.30
Despite an increased survival of extremely preterm infants, we observed a continuous decrease in overall NEC rates by time period, falling from 3.0% in P1 to 2.0% in P3 and making it one of the lowest reported population-based rates.31 The overall NEC rate for infants below 33 weeks was, for example, significantly higher in the Canadian Neonatal Network (CNN) from 2003 to 2008, with a reported incidence of 5.1%.32 Why Swiss NEC rates are low and whether enteral feeding strategies explain this discrepancy remain unanswered. In agreement with other reports however, the multivariable analysis confirmed in our study an increased risk of NEC with lower GA and in SGA infants.30 ,32
Infants at the lowest GAs were at the greatest risk for mortality and morbidity.33–35 One or more of the four major morbidities (ie, BPD (oxygen requirement at 36 weeks), IVH 3–4, NEC, cPVL) were observed in about 16% of survivors. Logistic regression analysis identified four factors associated with ‘survival free of major complications’ in addition to the GA by periods: female gender and antenatal steroids, as well as absence of SGA and congenital malformations. Female gender has been repeatedly associated with better outcome.6 ,36 We found a lower incidence of IVH 3–4 but not of other individual morbidities, similar to other published studies.24 ,37 ,38
Our study has some limitations. Stillbirths were excluded from the analysis. The 5% overall missing values may marginally underestimate the delivery room mortality if such deaths occurred in a lower-level unit. However, recommendations since 2002 urge transfer to a level III NICU from 23 0/7 weeks GA. Therefore, these cases concern preferentially preterm infants at the upper gestation age range that were not transferred into a level III NICU as in good condition. Beyond mortality, our study focused on short-term complications, which are only partial predictors for poor long-term outcome,37 despite being often used as surrogate markers of quality improvement.39 Furthermore, we may have missed some surrogate indicators of poor outcome. The retinopathy of prematurity (ROP) incidence, for instance, was not included in our analysis due to insufficient data quality during the first study period. During periods 2 and 3, the incidence of ROP stage III or higher in our <32 weeks GA infants remained unchanged at 1.9% (95% CI 1.4% to 2.5%). These low figures are in agreement with the 4.9% (41/844) ROP rate reported by Schlapbach et al40 in the Swiss cohort for the years 2000–2008 in a refined 2-year follow-up analysis of younger infants <28 weeks GA.
The strength of this study is its large size, the prospective and nationwide, population-based design, as well as a very high inclusion rate of 95%, providing short-term outcomes of virtually all live-born very preterm infants in Switzerland over a 13-year period.
The current population-based mortality and morbidity data for the very preterm population allow medical teams to provide up-to-date information for prenatal parental counselling and may aid in clinical decision-making, particularly at very early GAs where ethical considerations need epidemiologic support. Reported mortality and short-term outcomes also provide a benchmark for neonatal care in Switzerland and abroad. While the improvement in mortality rates is encouraging, areas for targeted improvement have been identified. Concentrated efforts must be undertaken to improve our understanding of why BPD is increasing and what may be done to further reduce short- and possibly long-term morbidities.
References
Footnotes
Collaborators The following investigators and hospitals participated in the Swiss Neonatal Network: Aarau: Cantonal Hospital Aarau, Children's Clinic, Department of Neonatology (Ph Meyer, C Anderegg); Basel: University Children's Hospital Basel, Department of Neonatology (S Schulzke); Berne: University Hospital Berne, Department of Neonatology (M Nelle), Department of Pediatrics (B Wagner); Chur: Children's Hospital Chur, Department of Neonatology (W Bär); Lausanne: University Hospital (CHUV), Department of Neonatology (J-F Tolsa, M Roth-Kleiner); Geneva: Department of Child and Adolescent, University Hospital (HUG), Neonatology Units (RE Pfister); Lucerne: Children's Hospital of Lucerne, Neonatal and Paediatric Intensive Care Unit (TM Berger); Neuchatel: Cantonal Hospital Neuchatel, Department of Pediatrics (M Ecoffey); St Gallen: Cantonal Hospital St Gallen, Department of Neonatology (A Malzacher), Children's Hospital St Gallen, Neonatal and Paediatric Intensive Care Unit (JP Micallef); Winterthur: Cantonal Hospital Winterthur, Department of Neonatology (L Hegi); Zurich: University Hospital Zurich (USZ), Department of Neonatology (D Bassler, R Arlettaz), University Children's Hospital Zurich, Department of Neonatology (V Bernet); Central data manager (M Adams).
Contributors FC and REP had primary responsibility for the study design, data analysis and interpretations and writing the manuscript. NMB was involved in data analysis and data interpretation and writing of the manuscript. KMP-B and PCR were involved in data analysis and revising the manuscript. All authors approved the final version of this manuscript.
Competing interests None declared.
Ethics approval Swiss Federal Commission for Privacy Protection in Medical Research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data is available to all Swiss Neonatal Network members under the control of the Swiss Society for Neonatology.