Article Text

Abstract
We propose that the respiratory transition at birth passes through three distinct, but overlapping phases, which reflect different physiological states of the lung. Accordingly, respiratory support given to infants should be optimised to suit the underlying physiological state of the lung as it passes through each phase. During the first phase, the airways are liquid-filled and so no pulmonary gas exchange can occur. Respiratory support should, therefore, be focused on clearing the gas exchange regions of liquid. In the absence of gas exchange, little or no CO2 will accumulate within the airways and, therefore, interrupting inflation pressures to allow the lung to deflate and exhale CO2 is unnecessary. This is the primary rationale for administering a sustained inflation at birth. During the second phase, the gas exchange regions are mostly cleared of liquid, allowing pulmonary gas exchange to commence. However, the liquid cleared from the airways resides within the tissue during this phase, which increases perialveolar interstitial tissue pressures and the risk of liquid re-entry back into the airways. As a result, respiratory support should be optimised to minimise alveolar re-flooding during expiration, which can be achieved by applying an end-expiratory pressure. The third and final phase occurs when the liquid is eventually cleared from lung tissue. Although gas exchange may be restricted by lung immaturity, injury and inflammation during this phase, considerations of how fetal lung liquid can adversely affect lung function are no longer relevant.
- Neonatology
- Fetal Medicine
- Respiratory
- Physiology
Statistics from Altmetric.com
Introduction
As the future airways of the fetal lungs are liquid-filled and gas exchange occurs across the placenta before birth, the site of gas exchange must immediately switch to the lungs after birth as soon as the umbilical cord is clamped.1–3 To achieve this, the airways must be rapidly cleared of liquid so that the lungs can aerate. However, lung aeration is not only critical for pulmonary gas exchange as it is also responsible for initiating the cardiovascular changes at birth, which together underpin the transition to newborn life.1 ,3 As such, lung aeration is the critical central event that initiates a sequence of interdependent physiological changes that enable the infant to transition to independent life after birth.
Failure to adequately clear the airways of lung liquid at birth is a major cause of neonatal morbidity and mortality, particularly in very preterm infants.4 ,5 As a result, these infants usually require some form of respiratory support, which commonly involves the application of positive pressure ventilation, applied either non-invasively (via a face mask) or following intubation of the trachea.6–8 However, there is still considerable debate as to how this respiratory support should be delivered.8 Recent advances in our understanding of the mechanisms regulating lung aeration at birth9 ,10 have provided new insights as to how this process can be facilitated in newborn infants. However, the current focus is almost entirely on gas exchange with little or no attention applied to facilitating airway liquid clearance, uniform lung aeration or preventing alveolar re-flooding during the immediate newborn period. While gas exchange is the primary consideration, these additional factors should not be overlooked as they greatly impact on the capacity of the lung to exchange respiratory gases. In this review, we will discuss recent advances in our understanding of the factors driving airway liquid clearance and propose a new approach for supporting pulmonary ventilation at birth. Specifically, we suggest that the respiratory transition occurs in three phases and that any respiratory support provided requires different approaches to be effective in each phase (figure 1).
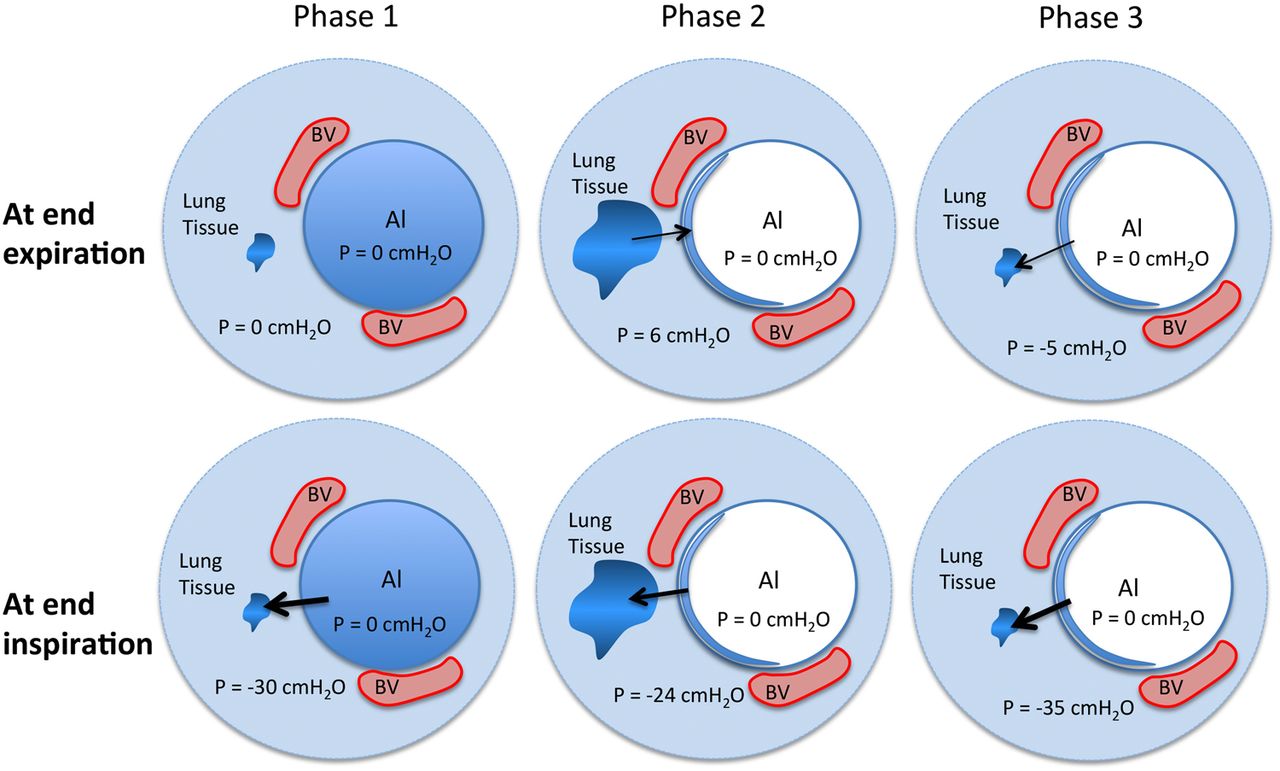
The lung passes through three distinct phases as it transitions from a liquid-filled organ with a low blood flow into the sole organ of gas exchange after birth. During the first phase, the liquid-filled airways must be cleared of lung liquid so that gas exchange can commence. Airway liquid clearance primarily results from transepithelial pressure gradients generated during inspiration, which provides the pressure gradient for liquid to move from the upper into the lower airways and then across the epithelium into the surrounding lung tissue. In most infants, it is likely that this phase is very short in duration (ie, seconds), but can extend for many minutes, which will be reflected by continuing low oxygenation and heart rates immediately after birth. During the second phase, the liquid cleared from the airways resides within the interstitial tissue, which increases interstitial tissue pressures and increases the likelihood of liquid re-entering the airways at end-expiration (ie, at functional residual capacity). As liquid clearance from lung tissue is much slower than it is from the airways, this phase can last for hours (∼4 h); however, application of a positive end-expiratory pressure will reduce the pressure gradient for airway liquid re-entry. The third phase depicts the lung following all airway liquid clearance from the chest, resulting in subatmospheric interstitial tissue pressures and the generation of end-expiratory pressure gradients, which assist in keeping the airways cleared of liquid. Al, alveolus; BV, blood vessels; P, pressure.
We propose that:
The first phase involves airway liquid clearance and principally involves the movement of liquid through the airways and across the distal airway wall. As gas exchange is not possible during much of this phase, because the distal airways are liquid-filled, the focus should be on moving liquid through the airways with the goal of uniformly aerating gas exchange regions (figure 1).
The second phase overlaps with and occurs as a direct result of the first phase, whereby liquid leaving the airways temporarily accumulates within the interstitial tissue compartment. This transiently increases interstitial tissue pressures and the probability of liquid re-entry into the airways, thereby compromising gas exchange (figure 1).
The third and final phase occurs when the liquid has been cleared from the tissue, although there is likely to be much overlap with phase 2 in different regions of the lung, at least during the initial stages. During this phase, respiratory support can primarily focus on gas exchange, uniform ventilation and maintaining respiratory homeostasis (figure 1).
Currently, the recommended approach is unidimensional, mainly focusing on strategies applicable for an already aerated lung that is not ‘water-logged’. We suggest that the respiratory support provided to an infant should be consistent with the physiological state of the lung and vary depending upon the phase of transition.
Phase 1: airway liquid clearance
There has been considerable debate in the literature about the mechanisms of airway liquid clearance at birth and the timing at which this process commences.6 ,11 ,12 Nevertheless, when taken altogether (see below), it is evident that airway liquid clearance can occur due to a variety of different mechanisms.6 However, in any one infant, the mechanism that provides the greatest contribution will likely differ depending on the timing (gestational age) and mode of delivery (vaginal vs caesarean section (CS) delivery).
Liquid clearance before birth
While it has been suggested that airway liquid volumes can decrease days before birth,5 ,13 this has not been confirmed in pregnancies with established normal amniotic fluid volumes.14 Oligohydramnios is known to reduce lung liquid volumes due to an increase in transpulmonary pressure, causing the loss of lung liquid.15 Similarly, any situation that reduces the available intrauterine space, such as the presence of a twin, may reduce lung liquid volumes before labour onset. However, when considered in relation to the lung's capacity to clear airway liquid after birth (see below), this debate appears somewhat esoteric unless the infant is delivered by CS. In this situation, the mechanisms for airway liquid clearance during birth are absent, necessitating that all airway liquid is cleared across the airway epithelium, with little being lost via the nose and mouth.4
Liquid clearance during birth
Fetal postural changes
Numerous reports in the literature have described the loss of large volumes of liquid via the nose and mouth following delivery of the infant's head.6 ,16 This mechanism of lung liquid loss is commonly referred to as ‘vaginal squeeze’. However, this description is not entirely accurate as the infant's chest offers little resistance to delivery compared with the head and shoulders.17 Instead, it is thought that uterine contractions force a change in fetal posture, which greatly increases fetal spinal flexion.15 As for oligohydramnios, this increases abdominal pressure, which increases transpulmonary pressure by elevating the diaphragm, resulting in lung liquid loss via the nose and mouth. This process likely explains the ‘gushes’ of liquid that have been observed following delivery of the infant's head.
Na reabsorption
Until recently, the primary mechanism responsible for airway liquid clearance at birth was thought to result from Na+ uptake across the airway epithelium, which reverses the osmotic gradient leading to airway liquid reabsorption.5 This mechanism is stimulated by increased circulating adrenaline and vasopressin levels, released in response to the stress of labour, and provides a convenient explanation for why infants born by CS have a higher risk of transient tachypnoea of the newborn (TTN; wet lung).4 ,5 However, this mechanism only develops in late gestation and is absent in the immature lung of preterm infants, as RNA transcripts encoding epithelial Na channels (ENaC) subunits are virtually undetectable in the immature human lung.18 Clearly, preterm infants cannot use this mechanism to clear airway liquid.19 ,20
Although adrenaline and vasopressin infusions inhibit lung liquid secretion and activate liquid reabsorption late in gestation,21–23 pharmacological doses are required to achieve liquid reabsorption.22 ,24 Furthermore, based on the measured reabsorption rates achieved, it would take hours to clear all liquid21–23 and adrenaline would have to remain elevated throughout this time.25 However, normal healthy infants can clear their airways of liquid and establish effective gas exchange within seconds to minutes of birth.20 ,26 ,27 Similarly, although heart rates commonly increase (from ∼100 to 160 bpm) after birth,28 there is no evidence of a sustained tachycardia,28 which would be expected during a sustained stress-induced catecholamine release.
While there is considerable evidence indicating that ENaCs help to control airway liquid in an aerated lung,18 ,29 their role in airway liquid clearance at birth is less certain. Indeed, while inhibiting ENaC activity with amiloride delays lung liquid clearance in spontaneously breathing newborns, it does not prevent it and its effect in ventilated newborns is restricted to the expiratory phase.30 ENaCs are encoded by three different genes (α-, β- and γ-), with the mature protein comprised of three subunits.18 As α-ENaC knockout mice died of respiratory failure within 40 h of birth and had increased lung wet weights, it was assumed that deletion of the α-ENaC gene disrupted airway liquid clearance.31 However, these newborn mice also had weak inspiratory activity,18 which likely contributed to respiratory failure, as respiratory function is a major determinant of lung aeration at birth.9 ,10 Indeed, deletion of β-ENaC or γ-ENaC subunits does not cause respiratory failure despite reducing ENaC activity sixfold.18 Similarly, infants with gene mutations that markedly reduce ENaC activity (pseudoaldosteronism) do not suffer respiratory failure at birth.32
Liquid clearance after birth
While the mode and timing of delivery must influence the volume of airway liquid, at birth liquid must partly fill the airways as air is unlikely to enter the distal airways before the head is delivered. As such, a significant amount of liquid must be cleared after birth, particularly from the distal airways, but until recently, the role of postnatal mechanisms has been largely overlooked as a major mechanism driving airway liquid clearance. Indeed, recent studies indicate that respiratory activity plays the final and most significant role in airway liquid clearance9 ,10 at birth.
Role of respiratory activity
Using phase-contrast X-ray imaging, the entry of air into the lungs after birth has been imaged to study the temporal and spatial pattern of lung aeration. These studies demonstrate that lung aeration mostly (∼95%) occurs during inspiration, in spontaneously breathing term newborn rabbits, with no liquid clearance occurring between breaths; movies can be viewed at http://www.neoresus.org.au/pages/LM1-7-Breathing.php#B_FirstBreaths and http://www.fasebj.org/cgi/content/full/fj.07-8208com/DC1.9 ,10 Instead, the air/liquid interface tended to move proximally between breaths, reflecting liquid re-entry into the airways and a gradual decline in functional residual capacity (FRC). As amiloride increases the rate of FRC decrease,30 Na reabsorption may assist in maintaining FRC by minimising liquid re-entry into the airways between breaths. Lung aeration and FRC accumulation only occurred during inspirations, resulting in a stepwise increase in FRC with each breath.9 ,10 The FRC increase per breath varied, but was as high as 3 mL/kg in some newborns, resulting in an FRC of 15 mL/kg after five breaths, over ∼30 s.9 ,10 Thus, with an inspiratory time of ∼0.3 s, these newborn rabbits cleared airway liquid at a rate of ∼9 mL/kg/s (or ∼32 L/kg/h) during inspiration, which is considerably greater than what can be achieved with adrenaline (maximum of 10 mL/kg/h).21–23
Inspiration-induced airway liquid clearance is thought to result from an increase in the transepithelial pressure gradient.9 ,10 This gradient is generated by inspiratory muscles, which reduce intrapleural and interstitial tissue pressures by expanding the chest wall. This produces a pressure gradient across the airway wall, between the interstitial tissue and airway lumen, as well as between the upper and lower airways. As a result, liquid is driven from the proximal into the distal airways from where it is cleared across the distal airway wall into the surrounding interstitial tissue space.
Facilitating airway liquid clearance after birth
Recognising that increased transepithelial pressure gradients drive airway liquid clearance has provided a new understanding for how lung liquid clearance can be facilitated in preterm infants.11 While inspiration generates the pressure gradients across the airway wall by creating subatmospheric pressures within perialveolar tissue, numerically similar pressure gradients can be achieved by applying positive pressures to the airways.30 This is commonly achieved by applying intermittent positive pressure ventilation via a facemask, with inspiratory times of 0.3–0.5 s. However, it is questionable whether this is the most appropriate ventilation strategy. Indeed, the principal goal at this stage of resuscitation is to clear the airways of liquid because gas exchange is prevented due to the presence of liquid in the distal airways (figure 1). As the viscosity of liquid is considerably higher than air, the airway resistance is ∼100 times higher when the lung is liquid-filled versus when it is air-filled. It is for this reason that the resistance decreases and lung compliance markedly increases as the lung aerates after birth.33 ,34
Due to the high resistance of moving liquid through the airways relative to air, either higher pressures or longer inflation times are required to move the same volume of liquid compared with air. Since the resistance rapidly decreases as the airways fill with air, the pressure required to move a fixed volume of air into the lung will also rapidly decrease as the lung aerates.33 ,34 Thus, using high pressures and short inflation times risk over inflating lung regions and causing injury if regions aerate more quickly than the caregiver expects. Furthermore, as lung aeration in different lung regions occurs at very different rates, aeration across the lung is initially non-uniform and progressively becomes more uniform as the inflation time increases.33–35 Thus, air will initially flow rapidly into and inflate aerated lung regions, simply because this is the lowest resistance pathway for airflow, whereas air will only flow into liquid-filled regions when airway pressure exceeds the pressure required to overcome the resistance to move liquid through the airways.33 ,34 As such, the flow dynamics and tissue mechanics of liquid-filled and aerated lung regions are vastly different, making it extraordinarily difficult to ventilate without overinflating and injuring aerated lung regions.
The application of long initial inflation times greatly increases the uniformity of lung aeration before the onset of tidal ventilation. While lung aeration continues to occur in a non-uniform pattern during the sustained inflation (SI), if the inflation is long enough, most of the lung will aerate before the inflation has ceased.33 ,34 This process has been visualised using phase-contrast X-ray imaging, demonstrating that an SI can uniformly aerate the lung and fully recruit an FRC and tidal volumes following the onset of tidal ventilation.33 ,34 This ensures that during the subsequent tidal ventilation period the incoming air is uniformly distributed across the lung, thereby reducing the risk of regional overinflation. Uniform lung aeration also avoids large ventilation-perfusion mismatch, which can occur in a partially aerated lung.36
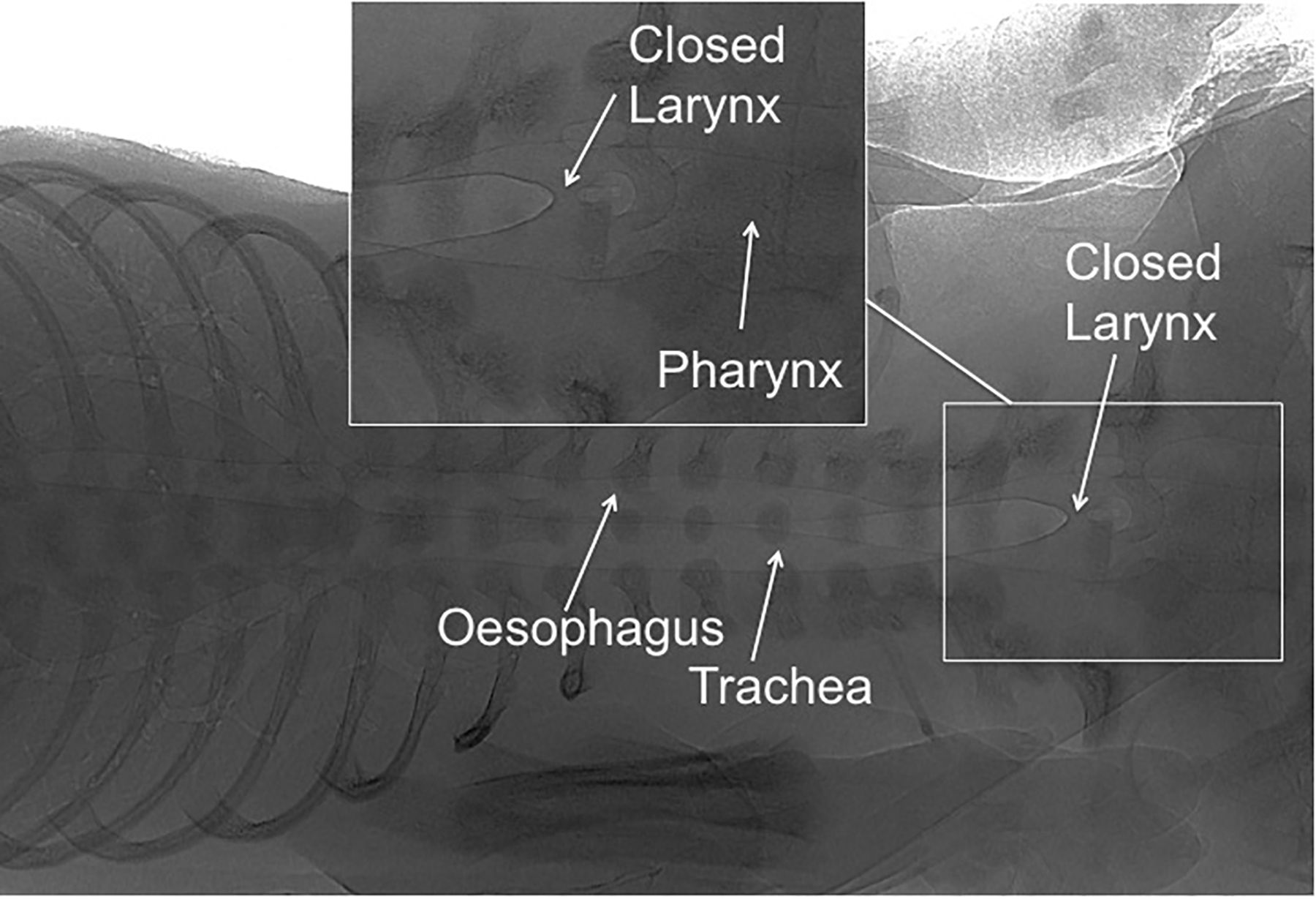
While there is considerable debate in the literature as to the efficacy of an SI at birth, recent clinical studies have failed to show a significant benefit of an SI.37 ,38 The question, therefore, arises, why are they effective in animal studies, but not in human trials? One possible answer is the method of application. In all animal studies, the SI was applied in intubated animals, whereas in humans, the SI has been applied non-invasively, mostly using a facemask.37 ,38 An analysis of the airflow and gas volume changes during the SI in humans demonstrates that airflow into the lung is greatly restricted unless the infant takes a breath, indicating the presence of an obstruction.37 While this could be a consequence of head and mask position, our recent imaging studies indicate that the glottis may be actively adducted at birth (figure 2), thereby preventing air from entering the lung during an SI. It is well established that, before birth, active glottic adduction during apnoea is an important mechanism for maintaining lung expansion and lung growth.39–41 Thus, if this pattern of activity persists into the newborn period, then we should expect apnoeic infants to have an adducted glottis.

{kind=link}
{kind=link}
Phase-contrast X-ray image of the upper chest, trachea, larynx and pharynx in a near term (30 days), spontaneously breathing newborn rabbit. The larynx is closed immediately after birth, which prevents air from entering the airways during intermittent positive pressure ventilation, applied via a facemask.
Phase 2: liquid accumulation within the lung's interstitial tissue compartment
The process of airway liquid clearance results in liquid movement across the distal airway wall into the surrounding tissue.9 As this mostly occurs during inspiration, the movement of liquid (∼9 mL/kg/s) across the epithelium is extremely rapid, resulting in near complete airway liquid clearance (>15 mL/kg of liquid) within 3–5 breaths (over 15–30 s) in term spontaneously breathing rabbits.9 On the other hand, clearance of this liquid from the tissue via the lymphatics and blood vessels is thought to take considerably longer (4–6 h).42 As a result, significant amounts of liquid reside within the interstitial tissue compartment for the first 4–6 h after birth, essentially resulting in pulmonary oedema42 (figure 1). As the liquid is accommodated within a compartment that has a finite volume, this must result in an increase in pressure within that compartment (figure 1). This explains why the chest wall expands9 and interstitial tissue pressures increase (to ∼6 cmH2O)43 immediately after birth. Interstitial tissue pressures then gradually decrease over the next 4–6 h to permanently become subatmospheric (at rest).43
By elevating interstitial tissue pressures,43 the accumulation of airway liquid within the lung's interstitial tissue compartment must increase the hydrostatic driving pressure for liquid to re-enter the airways.10 As a result, when alveolar pressures decrease to atmospheric pressure during expiration, liquid tends to re-enter the airways, albeit much more slowly than its clearance during inspiration due to the smaller pressure gradient (figure 1). This explains the gradual reduction in FRC that occurs between breaths in spontaneously breathing term newborn rabbits immediately after birth.10 ,30 This airway liquid is quickly recleared back into the tissue with subsequent inspirations, resulting in a continuous cycle of airway liquid clearance and re-entry during the breathing cycle.10 It is likely that this cycle continues until excess liquid is cleared from the tissue (via lymphatics and vessels) and interstitial tissue pressures become subatmospheric.42 ,43 While this may seem inefficient, as the hydrostatic pressure gradient generated during inspiration (20–80 cmH2O) in term infants44 is much greater than the reverse gradient during expiration (∼6 cmH2O),43 the potential to clear liquid from the airways during inspiration is considerably greater than the potential for airway liquid re-entry. This is one reason why the application of positive airway pressures at rest (positive end-expiratory pressure and continuous positive airway pressure (CPAP) are important in ventilated and spontaneously breathing preterm infants immediately after birth.33 ,45 That is, by maintaining a positive airway pressure at rest, these strategies not only assist the compliant chest wall in opposing lung recoil, but also reduce the hydrostatic pressure gradient for liquid to move back into the airways (figure 1). In essence, most newborns also adopt this strategy by invoking expiratory braking manoeuvres and grunting shortly after birth.10 ,26 These manoeuvres increase airway pressures during expiration, which help to oppose liquid movement back into the airways and maintain FRC.
TTN; is it consequence of large airway liquid volumes at birth?
As the majority of liquid residing in the airways at birth is cleared into the surrounding tissue, the greater the volume of liquid in the airways, the greater the volume of liquid that must be temporarily accommodated in the interstitial space immediately after birth (figure 1). Logically, greater liquid volumes within the tissue must result in higher interstitial tissue pressures and, therefore, a greater driving pressure for airway liquid re-entry. The question of whether there are situations in which infants are born with larger (or smaller) volumes of liquid in their airways is an interesting one and is most probably applicable to infants born by CS. It is widely considered that term infants delivered by CS without labour have a higher incidence of TTN or ‘wet lung’ because they have not experienced the stress of labour and the adrenaline-induced activation of Na+ (and liquid) reabsorption.4 ,29 While this is a convenient explanation that fits nicely with previous concepts for airway liquid clearance,5 it assumes that Na+ reabsorption is the primary mechanism involved, which is unlikely (see above). This explanation also ignores other birth-related mechanisms for reducing airway liquid volumes and cannot explain why millions of infants born by CS are able to clear their airways of liquid without any respiratory-related issues.
We suggest that TTN is primarily the result of being born with larger volumes of airway liquid, resulting in larger volumes of liquid accumulating in the tissue and a greater potential for airway liquid re-flooding. We propose that delivery by CS bypasses the mechanisms detailed above for airway liquid clearance during birth, particularly the postural changes. This increases the likelihood of an infant being delivered with larger volumes of airway liquid than would otherwise occur if it was born vaginally. As this liquid has to eventually be accommodated in the tissue,42 this will result in higher interstitial tissue pressures43 and increase the potential for liquid re-flooding back into the airways. This, in turn, increases the need for increased inspiratory activity (larger and faster rate) to re-clear the airways and facilitate gas exchange. This suggestion is consistent with the finding that infants born by CS and who develop TTN also display increased grunting and expiratory braking.4 It is also not surprising, therefore, that CPAP, which maintains a positive pressure on the airways to oppose liquid re-entry into the airways, is an effective treatment for TTN.
It is interesting that, compared with near term infants, preterm infants do not appear to share the same risk of increased respiratory morbidity (eg, TTN) when delivered by CS as opposed to vaginal delivery. Perhaps, this reflects the structural immaturity of the preterm lung, whereby preterm infants have lungs with relatively more interstitial tissue and smaller gas exchange surface areas. A relatively larger interstitial tissue compartment allows larger volumes of liquid to be accommodated with only small increases in pressure, whereas a smaller surface area will restrict the bidirectional movement of liquid across the epithelium. Indeed, a reduced distal airway surface area will not only restrict airway liquid clearance, but will also restrict liquid re-flooding back into the airways. Logically, a reduced surface area will mainly affect airway re-flooding due to the lower transepithelial pressure gradients driving liquid movement in that direction. As such, it is possible that preterm infants can cope with both higher liquid volumes and interstitial tissue pressures, without resulting in airway re-flooding.
Liquid accumulation within lung tissue is likely to have consequences other than an increased potential for liquid to re-enter the distal airways. Indeed, it is likely to substantially alter tissue mechanics, potentially making the lung significantly less compliant and thereby increasing the pressures required to inflate it. While this could also act as an inbuilt protective mechanism that reduces the potential of overinflation-induced lung injury, unequal distribution of this liquid within different regions will greatly alter compliance differences across the lung. This may contribute to inhomogeneous ventilation of the lung and increasing the risk of overinflation injury in more compliant lung regions, particularly non-dependent lung regions. To fully comprehend the significance of tissue liquid accumulation, it is important to determine the extent to which accumulation differs in different lung regions and whether the liquid is mobile. That is, can it move between lung regions through the tissue due to gravity-related pressure gradients that are known to exist in the lung, for example, between dependent and non-dependent lung regions?
Phase 3: respiratory gas exchange and metabolic homeostasis
Following lung aeration and the clearance of liquid from the tissue, the infant has passed through the immediate birth transition phase. While some fetal characteristics may persist (eg, patent duct), the approaches used to assist lung function and respiratory gas exchange at this time are more akin to the traditional approaches that are commonly practised by caregivers in neonatal intensive units. It is possible that pulmonary oedema and increased interstitial tissue pressures may reoccur in response to problems such as pulmonary hypertension. However, in the absence of these morbidities, ventilation can be more focused towards gas exchange and maintaining respiratory gas homeostasis. In this situation, the success of establishing adequate gas exchange will depend on overcoming the structural and functional deficiencies of the lung as well as the immaturity of the respiratory muscles and the high compliance of the chest wall. The mechanisms and approaches of this respiratory phase have been extensively described previously and will not be discussed here. Instead, we suggest that the priorities of this phase should not overly dominate the focus of respiratory support provided to preterm infants as they transition to newborn life. Indeed, the optimal management of preterm infants during the early phases will include a variety of considerations in addition to these traditional approaches.
Summary
We propose that at birth the lung passes through three distinct, but overlapping phases as it transitions into the primary gas exchange organ at birth. As the physiological state of the lung during each phase is distinctly different, we suggest that the respiratory support given to infants should be optimised to suit the lungs underlying physiological state during each phase. During the first phase, pulmonary gas exchange cannot occur as the terminal airways are liquid-filled and so respiratory support should be focused on clearing liquid from the gas exchange regions. Due to the absence of gas exchange, little or no CO2 will accumulate within the airways and so the need to exhale the CO2 is unnecessary. As such, it is logical to consider sustaining the initial inflation pressures to allow the lung to fully aerate before being deflated. However, we need to await the outcomes of current clinical trials to assess the efficacy of this treatment in humans. During the second phase, although the gas exchange regions are mostly cleared of liquid, this liquid resides within the perialveolar interstitial tissue, which increases hydrostatic pressures and the risk of liquid re-entry back into the airways. As a result, respiratory support should be optimised to minimise alveolar re-flooding during expiration, which can be achieved by applying an end-expiratory or continuous positive pressure. The third and final phase occurs when the liquid is eventually cleared from lung tissue. Although gas exchange may be restricted by lung immaturity, injury and inflammation during this phase, considerations of how fetal lung liquid can adversely affect lung function has less relevance.
References
Footnotes
Contributors SBH wrote the initial draft, which was modified and edited by ABtP and MJK.
Funding This research was supported by an NHMRC Program Grant (606789) and the Victorian Government's Operational Infrastructure Support Program.
Competing interests SBH is supported by an NHMRC Principal Research Fellowship, ABtP is supported by a Veni-grant from The Netherlands Organisation for Health Research and Development (91612027). MJK is supported by an ARC Australian Research Fellowship (grant DP110101941).
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Fantoms