





Abstract
Background Obesity has been associated with poor outcomes of asthma in cross-sectional studies, but long-term effect of obesity on asthma remains unknown.
Aims To study the effects of obesity, found at the time of diagnosis of adult-onset asthma, on 12-year prognosis by focusing on oral corticosteroid (OCS) use and respiratory-related hospital admissions.
Methods Patients diagnosed with adult-onset asthma (n=203) were divided into three categories based on diagnostic body mass index (BMI) (<25 kg·m−2, 25–29.9 kg·m−2, ≥30 kg·m−2) and followed for 12 years as part of the Seinäjoki Adult Asthma Study. Self-reported and dispensed OCS were assessed for the 12-year period. Data on hospital admissions were analysed based on medical records.
Results 12 years after diagnosis, 86% of the patients who were obese (BMI ≥30 kg·m−2) at diagnosis remained obese. During the follow-up, no difference was found in weight gain between the BMI categories. During the 12-year follow-up, patients obese at diagnosis reported more frequent use of OCS courses (46.9% versus 23.1%, p=0.028), were dispensed OCS more often (81.6% versus 56.9%, p=0.014) and at higher doses (median 1350 (interquartile range 280–3180) mg versus 600 (0–1650) mg prednisolone, p=0.010) compared to normal-weight patients. Furthermore, patients who were obese had more often one or more respiratory-related hospitalisations compared to normal-weight patients (38.8% versus 16.9%, p=0.033). In multivariate logistic regression analyses, obesity predicted OCS use and hospital admissions.
Conclusions In adult-onset asthma, patients obese at diagnosis mostly remained obese at long-term and had more exacerbations and respiratory-related hospital admissions compared to normal-weight patients during 12-year follow-up. Weight loss should be a priority in their treatment to prevent this outcome.
Abstract
Obese patients with new adult-onset asthma often remain obese in the long-term and have more exacerbations and respiratory-related hospital admissions during follow-up. High priority should be given to weight loss during treatment to prevent this outcome. https://bit.ly/2G5HtRZ
Introduction
Obesity has been suggested as a risk factor for adult-onset asthma [1–3]. It has been proposed to associate with poor outcomes of asthma, such as poor disease control, increased use of oral steroids, urgent visits to healthcare and lower lung function, but the results are not consistent [4–7]. In addition, adverse effects of obesity on asthma are supported by the existence of an obesity-related phenotype, identified by many cluster analyses [8–10]. This phenotype is characterised by frequent symptoms and exacerbations, use of high-dose inhaled corticosteroids (ICS), but normal eosinophil count [3, 8–10].
The vast majority of studies undertaken on the effects of obesity on asthma are cross-sectional, or have only a short follow-up. Thus, the long-term effects of obesity on asthma remain completely unknown [4, 6]. Mostly, smokers and patients with other comorbidities have been excluded [4–7]. Early- and late-onset asthma have been regarded as different phenotypes with different prognoses [3, 11, 12], but in previous obesity-related studies the age of onset is often mixed. Effects of obesity on late-onset asthma have been evaluated only in one previous study with a cross-sectional setting [6]. In this study, obese patients with late-onset asthma were suggested to present features of more severe asthma compared to leaner patients [6].
No previous study has concentrated on evaluating long-term prognosis of adult patients, who are obese at diagnosis, being the aim of this study. We focused in evaluating the effects of diagnostic obesity on the use of oral corticosteroids (OCS) and respiratory-related hospital admissions at 12-year follow-up in patients diagnosed with adult-onset asthma.
Methods
Study patients
The Seinäjoki Adult Asthma Study (SAAS) is a 12-year follow-up study in which 257 patients were diagnosed with new-onset adult asthma between October 6, 1999 and April 17, 2002. >94% of the patients diagnosed with novel asthma in the study site were recruited to the study [13]. Asthma diagnosis was made by a respiratory specialist based on lung function measurements and typical symptoms of asthma. Asthma diagnosis requirements and inclusion and exclusion criteria have been published previously [13] (supplementary table S1). The exclusion criteria were a previous diagnosis of asthma at age <15 years and inability or unwillingness to sign the informed consent. Patients were not excluded due to smoking history, comorbidities or another lung disease. Patients were recruited from the diagnostic visit and after diagnosis the patients were treated in primary care, occupational healthcare, private healthcare or in specialised healthcare according to principles of the Finnish Asthma Programme [14]. The mean follow-up time was 12.2 years (range 10.8–13.9 years), after which 203 (79%) patients returned to a follow-up visit (between December 10, 2012 and October 31, 2013) (supplementary figure S1). Written informed consent was obtained to a study protocol approved by the ethics committee of Tampere University Hospital (Tampere, Finland) (R12122). The 12-year prognosis, smoking characteristics, comorbidities and clusters of the SAAS cohort have been published previously [9, 15–17].
Use of oral corticosteroids and hospitalisations
Self-reported OCS use was defined as affirmative answer to “Have you used cortisone tablets (prednisolone, prednisone, Medrol, Solomet, dexamethasone) as short courses due to your asthma?” Information on dispensed OCS was obtained from the Finnish Social Insurance Institution. Only dispensed OCS indicated for asthma were taken into account. More detailed information is included in the supplementary material. Hospitalisations were collected from medical records.
Anthropometric measures, lung function, asthma control and inflammatory parameters
Body mass index (BMI) was calculated from measured weight in kilograms and height in metres. Lung function was measured using a Vmax Encore 22 spirometer (Viasys Healthcare, Palm Springs, CA, USA) which was calibrated daily. Patients completed the structured questionnaire AQ20 (Airways Questionnaire 20) at the diagnostic and follow-up visits [18]. The Asthma Control Test (ACT) was completed at the follow-up visit. Asthma control was based on Global Initiative for Asthma 2010 report [19]. Further information is available in the supplementary material.
Statistical analyses
Continuous data are expressed as mean±sd or median (interquartile range). Comparisons between three groups were done by one-way ANOVA, Kruskal–Wallis test or Chi-squared test. Multivariable binary logistic regression analysis was performed to find out predictors for OCS use and hospitalisation. Forward and backward methods were used in choosing the final model. Independent variables were from diagnostic time-point and for OCS use included sex, age of asthma onset, respiratory symptoms <16 years, BMI, pre-bronchodilator forced expiratory volume in 1 s (FEV1), smoking pack-years and blood eosinophils as categorised. For hospitalisations, independent variables were sex, age of asthma onset, COPD, hypertension, BMI, pre-bronchodilator FEV1 and AQ20 score as categorised. The final models contained no strong multicollinearity with r≥0.7. To estimate interaction effects between BMI and blood eosinophil levels on OCS use, we constituted a stratified analysis in groups with high and low blood eosinophil levels with a test for interaction [20]. Statistical analyses were performed using IBM SPSS statistics software (versions 22 and 25; Armonk, NY, USA). A p-value <0.05 was regarded as statistically significant.
Results
Patient characteristics
The study population consisted of 203 patients with adult-onset asthma and their baseline and follow-up characteristics are shown in supplementary table S2. The patients were mostly female, overweight, with mean±sd age of asthma onset 46±14 years. Half of the patients had a history of smoking. At diagnosis, 92% were steroid-naïve; ICS therapy was started for all patients after diagnosis; and at 12-year follow-up 76% were daily ICS users.
Diagnostic obesity and use of OCS courses during the 12-year follow-up
The patients were divided into three groups according to their BMI at asthma diagnosis (normal weight <25 kg·m−2, overweight 25–29.99 kg·m−2, obese ≥30 kg·m−2) (table 1). At the time of diagnosis, 24.1% were obese and 43.8% were overweight. After a mean follow-up time of 12.2 years, BMI was increased in all groups, with no difference in the weight gain between the groups (figure 1). Of the obese patients, 86% remained obese at the 12-year follow-up visit. At the long-term follow-up, most patients remained in their initial BMI group (figure 1). A comparison of asthma outcome between patients who remained obese and those who became non-obese until the 12-year follow-up visit is shown in supplementary table S3.
Basic demographics, medication and lung function at diagnosis and at 12-year follow-up visit in patients divided into three groups based on body mass index (BMI) at asthma diagnosis

Diagnostic body mass index (BMI) groups and development of BMI during the 12-year follow-up period. ΔBMI presented as mean±sd; p-value assessed by one-way ANOVA. n=203 at diagnosis and follow-up.
During the 12-year follow-up, patients who were obese at diagnosis reported more frequent use of OCS courses (figure 2a, table 2), were dispensed OCS more often (figure 2b, table 2) and at higher doses (figure 2c, table 2) compared to normal-weight patients. Of all patients, four (2.0%) reported daily use of OCS at the 12-year follow-up visit, but only two (1%) for asthma indication (table 2). During the whole follow-up period, 77% of all dispensed prednisolone (mg) was dispensed outside the pollen season. Of those reporting any OCS use during the follow-up period, three (4.6%) out of 65 had not purchased OCS and could be considered to have recall bias.

a) Self-reported and b, c) dispensed oral corticosteroids (OCS) and d) dispensed inhaled corticosteroids (ICS) during 12-year follow-up in patients divided according to body mass index (BMI) at the moment of asthma diagnosis. a, b) statistical comparison performed by Chi-squared test; c, d) data are presented as median, 25–75 percentiles and 5–95 percentiles; medians compared by Kruskal–Wallis test adjusted by Bonferroni correction for multiple tests.
Use of oral corticosteroids (OCS) and hospitalisations during 12-year follow-up in patients divided according to body mass index (BMI) at the moment of asthma diagnosis
Considering use of other medication to treat asthma, obese patients were dispensed more ICS during the 12-year follow-up period than normal-weight or overweight patients (figure 2d). At the 12-year follow-up visit obese and overweight patients used add-on therapies (long-acting β2-agonist, leukotriene receptor antagonist, theophylline or antimuscarinic agents) more often compared to normal-weight patients (table 1).
Diagnostic obesity and hospitalisations during 12-year follow-up
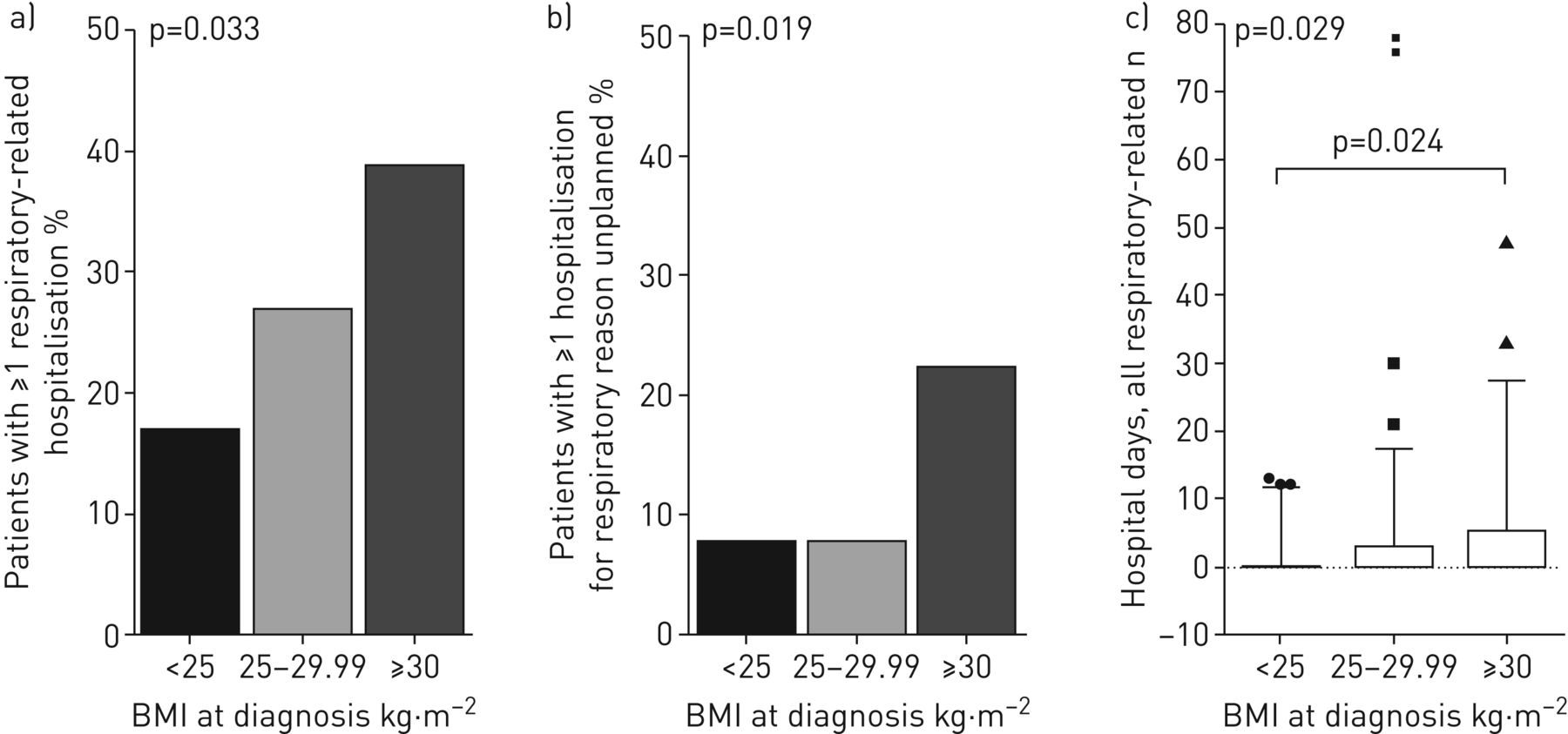
Proportion of patients having experienced any or unplanned respiratory-related hospitalisation during 12-year follow-up period was highest in the obese group (table 2, figure 3a and b). A similar finding was seen regarding total number of days in hospital (table 2, figure 3c).
{kind=link}
{kind=link}
{kind=link}
All a, c) respiratory-related and b) unplanned hospital admissions during 12-year follow-up in patients divided according to body mass index (BMI) at asthma diagnosis. a, b) statistical comparison performed by Chi-squared test; c) data are presented as median, 25–75 and 5–95 percentiles; medians compared by Kruskal–Wallis test adjusted by Bonferroni correction for multiple tests.
Diagnostic obesity and other asthma outcomes
Patients who were obese at diagnosis more often had uncontrolled asthma at the 12-year follow-up visit and were more symptomatic at diagnosis and follow-up visit, as indicated by AQ20 and ACT scores compared to non-obese groups (tables 1 and 3). Blood neutrophils were higher and exhaled nitric oxide fraction (FeNO) lower at 12-year follow-up in patients who were obese at diagnosis (table 3). FEV1 and forced vital capacity were lower among obese patients at both diagnostic and follow-up visits (table 1). The number of comorbidities and number of medications used to treat comorbidities were significantly higher in the overweight and obese groups. Obese and overweight patients suffered more often from diabetes, hypertension and psychiatric diseases, while only obese patients more often had depression and treated dyspepsia compared to normal-weight patients (table 3). Airway hyperresponsiveness to histamine was evaluated for 62 (30.5%) patients at the time of diagnosis, but the provocative dose to cause a 15% fall in FEV1 showed no statistically significant difference between the BMI groups (supplementary figure S2).
Secondary asthma-related outcomes at 12-year follow-up visit in patients divided according to body mass index (BMI) at the moment of asthma diagnosis
Diagnostic predictors for use of OCS to treat asthma
To investigate diagnostic predictors for self-reported OCS use at 12-year follow-up period we performed multivariate binary logistic regression analysis. Diagnostic predictors for OCS use were female sex, obesity and overweight, low blood eosinophil level before start of treatment (<0.20×109·L−1), lower pre-bronchodilator FEV1 (% predicted) at diagnosis and respiratory symptoms during childhood (table 4). Pack-years did not predict OCS use, and age of onset >60 years was a protective factor. Asthma–COPD overlap (ACO), diabetes, hypertension and coronary heart disease, smoking status and atopy at diagnosis were tested in the model, but did not predict OCS use. When using dispensing of one or more OCS as dependent variable, female sex, diagnostic obesity and blood eosinophil level <0.20×109·L−1 before start of treatment were found as predictors (supplementary table S4).
Diagnostic predictors for use of one or more oral corticosteroid (OCS) burst during 12-year follow-up
To examine hypothesis that only obese patients with non-eosinophilic asthma at diagnosis are prone to exacerbations, we divided patients into low and high eosinophil groups (cut-point 0.20×109·L−1) based on blood eosinophil level at diagnosis. In patients with low eosinophil level, higher proportion of obese (68.8%) and overweight (50.0%) had used at least one OCS course during follow-up compared to normal-weight patients (20.0%, p=0.023). In those with high blood eosinophils, the corresponding proportions were 37.5%, 22.5% and 20.5%, respectively (p=0.198) (supplementary table S5). p-values of interaction for overweight (p=0.081) and obesity (p=0.090) showed tendency towards interaction between obesity and low blood eosinophil level.
To further evaluate whether high or low blood eosinophil levels at diagnosis in obese patients result in different outcomes of asthma, we compared these groups. In addition to the increased OCS use, obese patients with low eosinophil levels tended to be older, have poorer FEV1 and had lower high-sensitivity C-reactive protein (hsCRP) at 12-year follow-up compared to obese patients with higher eosinophil levels (supplementary table S6).
Diagnostic predictors for hospitalisation for respiratory reasons
Our next goal was to evaluate diagnostic predictors for respiratory-related hospitalisations. Predictors for one or more hospitalisations during the 12-year follow-up period were obesity, hypertension, ACO and AQ20 score ≥12 (indicating very high symptoms) at diagnosis (table 5).
Diagnostic predictors for at least one hospitalisation during 12-year follow-up
Discussion
In this study we examined prognosis of patients who were diagnosed with adult-onset asthma and who were obese at diagnosis. Of those patients, 86% were still obese 12 years after diagnosis. The patients who were obese at the time of diagnosis more often used OCS courses and were more likely to be hospitalised during the 12-year follow-up period compared to normal-weight patients. Considering that long-term studies have been lacking on the effects of obesity on asthma and age of asthma onset has rarely been considered in previous studies, our study gives important and unique perspective regarding long-term effects of obesity on adult-onset asthma.
In previous studies, obesity has been associated with incident asthma [1, 2]. However, information has been conflicting regarding effects of obesity on asthma outcomes such as asthma control, and longitudinal studies have been lacking [4, 7, 23]. Furthermore, we found no studies assessing long-term prognosis for an obese patient with new asthma or long-term effects of obesity on adult/late-onset asthma. Therefore, our study has a unique setting. In our study almost nine out of 10 obese patients at diagnosis were still obese 12 years after diagnosis, the proportion being closely similar to that found in general population [24, 25]. Based on our material of limited size, migration between BMI categories in patients with asthma seems roughly similar or shows slightly more progression towards obesity compared to the general population [24, 25]. Of those who were obese at diagnosis, 47% reported use of at least one OCS course due to asthma during the following 12 years and 82% had purchased OCS, both 1.4- to two-fold compared to patients who were normal weight at diagnosis, and the results remained after adjustments (OR 4.15 for obese versus normal-weight; table 4). Furthermore, median dose of prednisolone dispensed over the follow-up period in obese patients was more than twice that in normal-weight patients. Poor use of controller treatment is not likely to explain the increased risk of exacerbations, because obese patients had purchased more ICS during the follow-up period than normal-weight patients. Proportion of OCS users differed in self-report versus dispensed data (47% versus 82%), which may be due to recall bias or purchasing OCS for reserve. However, because diagnostic obesity was associated with self-reported OCS use as well as with dispensed OCS in adjusted analysis, recall bias is unlikely to be playing a significant role in our main result. No similar studies with long-term follow-up in patients with confirmed diagnosis of asthma were found, but in previous short follow-up studies based on electronic records [26, 27], obesity at baseline year (not diagnosis) in patients with asthma was reported as a risk factor for two or more asthma attacks (OR 1.27) [26] or for at least one OCS dispensing linked to asthma encounter (OR 1.36) [27] in the following 1–2 years. In our self-report based data, overweight was a risk factor for increased OCS use, being supported by the previous studies [26, 27]. In total, our results add to previous ones by showing that being overweight or obese at diagnosis and remaining so in the long term is a significant risk factor for exacerbations in patients with confirmed diagnosis of adult-onset asthma.
Only one cross-sectional study [6] has assessed OCS use in early- and late-onset phenotypes of obese asthma and found that only obese subjects with early-onset, but not late-onset asthma, had more asthma exacerbations requiring OCS than non-obese subjects in the corresponding age of onset category. The patient materials in our study and the previous Severe Asthma Research Program (SARP) study differ in many ways: by setting (longitudinal versus cross-sectional), definition of late-onset asthma (SAAS ≥15 years, SARP ≥12 years), patient selection (unselected versus exclusion of smokers), proportion of severe asthma (5.6% versus 26%) and average age of asthma onset (46 years versus 27 years) [6]. Therefore, our studies may contain partly different phenotypes of asthma, which may explain the inconsistency in the results.
Respiratory-related hospitalisation was another important end-point of this study that was found to be twice as common in patients with asthma who were obese at diagnosis compared to leaner patients. Previous studies with similar setting were not found, but in study based on electronic records, obese and overweight patients with asthma had larger risk for asthma-related emergency room visits or hospitalisation (OR 1.40 for both) [27]. In our study, COPD and hypertension comorbidities were additional risk factors for respiratory-related hospitalisation. In a Taiwanese population-based study, patients with ACO according to diagnostic codes experienced more respiratory-related hospital visits than patients with asthma, supporting our results [28], but we could not find previous studies on hypertension as a risk factor for respiratory-related hospitalisations, constituting a new finding.
What are the plausible mechanisms behind obesity-related worsening of asthma, and what is the role of inflammation? Obesity has been associated with reduced corticosteroid responsiveness [29, 30] and non-eosinophilic asthma [31]. In our study, blood eosinophil levels were similar between diagnostic BMI groups, but our results suggest that the most plausible OCS users were those who were both obese and had low blood eosinophil level at diagnosis (<0.20×109·L−1), in a steroid-naïve situation. This implies that non-eosinophilic asthma and related reduced corticosteroid responsiveness [32] are important factors leading to exacerbations in obese patients. Besides OCS use, we noted only a few differences in long-term asthma outcome between obese patients with eosinophilic or non-eosinophilic asthma at diagnosis. However, it should be noted that our sample size was relatively low in the stratified analysis and the results should be confirmed in larger patient populations. According to our regression model, diagnostic low blood eosinophil level as such (suggesting non-eosinophilic asthma) predisposed for future OCS use. This is also a novel finding, given that previous studies have concentrated on predicting role of blood eosinophils in the ICS-treated situation. Overall, we show preliminary evidence that obese patients with new asthma and low blood eosinophil levels are the ones at highest risk for exacerbations and these patients need more careful follow-up and more effective interventions.
In addition, obesity has been proposed to worsen asthma control by affecting pulmonary mechanics, production of adipokines (e.g. leptin) and pro-inflammatory cytokines (e.g. interleukin (IL)-6, tumour necrosis factor-α) by adipose tissue and systemic inflammation [33], and via comorbidities such as depression [34] and gastro-oesophageal reflux disease [35]. Our cohort is predominantly female and on average middle-aged at asthma onset; in this and other previous studies female sex increased risk of exacerbations [26, 36]. Therefore, female sex hormones and menopause could play a role in worse outcome of asthma. Menopause has been associated with increased risk of asthma and respiratory symptoms [37, 38], the effect being stronger in those with higher BMI [38]. In our study, blood neutrophil level, IL-6 and hsCRP were higher in obese patients at 12-year follow-up, proposing a role for neutrophilic and systemic inflammation in obese asthma as previously suggested [39, 40], even though we cannot exclude the possible role of high corticosteroid use in provoking neutrophilic inflammation. In addition, lower FeNO levels in our obese patients indicates a lesser role for type 2 T-helper mechanisms in obese, late-onset asthma. Thus, our results suggest the concept of obese asthma involving non-type 2 mechanisms such as neutrophilia and systemic inflammation.
Our findings suggest that OCS use is more likely in patients with low FEV1 at diagnosis before the start of treatment. This finding is unique, since previous studies have concentrated on the predictive role of lung function in the treated situation [26, 41]. Two previous studies support the significance of better baseline FEV1 (<12 months from diagnosis) in predicting better asthma outcome: remission [42] and better control [15] of adult-onset asthma. We found no studies with exacerbations as an end-point. In our model, childhood respiratory symptoms were found to predict OCS use, but this was not repeated when dependent variable was dispensed OCS, leaving the finding unclear.
The major strengths of this study are the use of an unselected population with confirmed diagnosis of adult-onset asthma representing true adult asthma patients in clinics and a long follow-up period, considering that previous long-term follow-up studies on the effects of obesity have been lacking. Moreover, the two parameters of OCS used, self-reported and true dispensed, made the results more reliable. As limitation, BMI was used as measure of obesity, even though it does not describe the distribution of body fat. However, BMI has been used in the majority of asthma studies, making the results more comparable. Changing of BMI at long-term may affect the results, even though there was no statistically significant difference in the weight gain between the diagnostic BMI groups. Our results can be applied to a situation where an obese patient is encountered at diagnosis and obesity continues: what will be the prognosis for asthma? The results would be different if the obese group had lost weight and become normal-weight during the follow-up. Therefore, it is important to interpret the results in the light of long-term obesity.
Our results indicate that weight loss and weight control are important goals for obese patients with asthma. In support of this, in a large population-based database study the risk for emergency department visit or hospitalisation due to exacerbation decreased by half in a 2-year follow-up after bariatric surgery in obese asthma patients [6, 43]. Furthermore, previous results suggest that exacerbations can be reduced by a supervised weight reduction programme and low-energy diet for 8 weeks, which resulted in an average weight loss of 11.3% after 1 year [44]. However, more studies should be undertaken with exacerbations as an end-point. Overall, weight loss of 5–10% by lifestyle intervention has improved symptom control and quality of life in obese asthmatics [33, 45], but whether 5–10% weight loss is enough to reduce exacerbations in the long term remains unclear.
Our study, for the first time, produced long-term data on the effects of obesity on asthma. We showed that, without intervention, obese patients with new adult-onset asthma often remain obese. They have more exacerbations and hospital admissions, despite having been dispensed ICS in addition in higher amounts in the long term. This is a patient group with a poor outcome of asthma and a high burden to healthcare. In addition, our study suggests that low diagnostic blood eosinophil level may be used to identify obese patients with the highest exacerbation risk. As current treatments are less effective in obese patients, and as weight loss has many beneficial effects, weight loss should be prioritised in the management of asthma in obese patients.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-01209-2020.SUPPLEMENT
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-01209-2020.Shareable
Acknowledgements
Aino Sepponen (Dept of Respiratory Medicine, Seinäjoki Central Hospital, Seinäjoki, Finland) is gratefully acknowledged for her help through all the stages of this work.
Footnotes
This article has supplementary material available from erj.ersjournals.com
This study is registered at www.ClinicalTrials.gov with identifier number NCT02733016. All data generated or analysed during this study are included in this published article (and its supplementary files). According to ethical permission and patient data-protection laws of Finland, single patient data cannot be made available.
Author contributions: P. Ilmarinen, A. Pardo, L.E. Tuomisto and H. Kankaanranta designed the study. P. Ilmarinen and A. Pardo wrote the report with input from the other authors. P. Ilmarinen performed the statistical analyses and O. Niemelä contributed to laboratory analyses, respectively. I. Vähätalo assembled dispensed data. P. Nieminen contributed to statistical analyses. All authors contributed to interpretation of the data. All authors made critical revisions of the manuscript and approved the final version of the manuscript.
Conflict of interest: P. Ilmarinen reports grants and personal fees for lectures from AstraZeneca, personal fees for lectures from Mundipharma, GlaxoSmithKline and Novartis, outside the submitted work.
Conflict of interest: A. Pardo has nothing to disclose.
Conflict of interest: L.E. Tuomisto reports personal fees for lectures and meeting attendance from Boehringer Ingelheim and AstraZeneca, outside the submitted work.
Conflict of interest: I. Vähätalo has nothing to disclose.
Conflict of interest: O. Niemelä has nothing to disclose.
Conflict of interest: P. Nieminen has nothing to disclose.
Conflict of interest: H. Kankaanranta reports grants, personal fees for lectures and consultancy, and non-financial support for meeting attendance from AstraZeneca, personal fees for lectures and consultancy from Chiesi Pharma AB, Novartis and GlaxoSmithKline, personal fees for lectures from Mundipharma, personal fees for lectures and consultancy, and non-financial support for meeting attendance from Boehringer Ingelheim and Orion Pharma, personal fees for consultancy from SanofiGenzyme, outside the submitted work.
Support statement: Supported by Tampere Tuberculosis Foundation and the Finnish Anti-Tuberculosis Foundation, the Competitive State Research Financing of the Expert Responsibility Area of Tampere University Hospital (Tampere, Finland), and the Medical Research Fund of Seinäjoki Central Hospital (Seinäjoki, Finland), the Research Foundation of the Pulmonary Diseases (Helsinki, Finland), the Ida Montini Foundation (Kerava, Finland), the Pirkanmaa Regional Fund of the Finnish Cultural Foundation (Helsinki, Finland), Allergy Research Foundation (Helsinki, Finland). None of the sponsors had any involvement in the planning, execution, drafting or write-up of this study. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received April 16, 2020.
- Accepted September 21, 2020.
- Copyright ©ERS 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










