





Abstract
In major immigrant-receiving countries, annual foreign-born tuberculosis (TB) case counts and rates are relatively constant. Why this is so, and who might be a high-yield target for screening for latent TB infection, remain open questions.
Foreign-born TB in Canada during 1986–2002 was retrospectively examined using national TB and immigration data as well as census data. Case counts and rates were analysed in relation to demographics, immigration period and time since arrival.
Pre-1986 immigrants (n=3,860,853) and 1986–2002 immigrants (n=3,463,283) contributed 8,662 and 9,613 TB cases, respectively. Immigrants arriving ≤5 yrs ago and those arriving >10 yrs ago contributed almost equally to the annual foreign-born TB case count despite a 3.5-fold difference in in-country person-yrs. Remarkably stable and relatively low TB incidence was observed among immigrants >10 yrs post-arrival. Conversely, TB incidence within 5 yrs of arrival was dynamic, demonstrating a strong inverse association with time since arrival and higher sensitivity to changes in immigration level than shifts toward higher incidence source countries.
Relative constancy in foreign-born TB incidence is explained by a complex convergence of several factors. Immigrants born in high-incidence countries who arrived ≤2 yrs ago and were aged 15–34 yrs upon arrival constitute high-yield targets for preventive therapy.
Major immigrant-receiving countries with low tuberculosis (TB) incidence are frequently challenged by TB in their foreign-born people [1–4]. The World Health Organization (WHO) suggests that when foreign-born cases constitute 70% or more of national TB cases, one cannot anticipate more than a 2% decrease in annual national TB rates through the use of regular TB control programmes [5]. Under such circumstances, further reductions in national TB incidence and TB elimination require a rethinking of prevailing TB prevention and control strategies.
Canada, with one of the highest levels of immigration per capita internationally [6], is acutely aware of the increasing burden that TB in the foreign-born represents. Following a shift in immigration pattern from low- to high-TB-incidence countries in the 1960s and a substantial reduction in Canadian-born non-Aboriginal TB incidence, the proportion of foreign-born TB cases increased from 18% in 1970 to 67% in 2007 [2, 7–10]. In the same period, the foreign-born population nearly doubled, increasing the proportion of the foreign-born Canadian population from 15% in 1970 to 20% in 2007 [11]. Reflecting the WHO’s projections, Canada’s national TB incidence rate declined by an average of 2% annually between 2001 and 2007 [10].
That a shift in immigration pattern to high-incidence countries contributed to an increased proportion of foreign-born cases is a reasonable assumption given that country of birth/origin and time since arrival are key determinants of foreign-born TB incidence [1, 2, 12–15]. Similarly, an increase in both TB case counts and rates would seem logical following a sustained shift. However, only modest variations in annual foreign-born TB case counts and rates have been reported for several decades (with recent rate reductions being primarily attributed to denominator size) [2, 16]. This relative stability in foreign-born TB incidence in spite of high levels of immigration from regions of elevated incidence remained unexplained despite similar trends elsewhere [1, 17, 18].
There is a general consensus that TB elimination in major immigrant-receiving countries will be contingent on the successful prevention of TB in the foreign-born. However, without a comprehensive understanding of how foreign-born TB incidence is constructed, it will be exceedingly difficult, if not impossible, to effectively design and appropriately target any national TB prevention strategies. To bridge this knowledge gap, this study aimed to deconstruct foreign-born TB incidence in Canada in order to identify relative contributions and trends in TB incidence among immigrant groups. In doing so, it was anticipated that the factors related to the relative constancy in foreign-born TB incidence would be elucidated and high-yield targets for screening and treatment of latent TB infection (LTBI) be identified.
MATERIAL AND METHODS
Study population
The population of foreign-born permanent residents (“stock”) in Canada from January 1, 1986 until December 31, 2002 (study period) was divided into two groups. 1) Immigrants who arrived in 1986–2002: data from Citizenship and Immigration Canada, the federal government department responsible for immigration and settlement, was used to identify immigrants and refugees who were granted permanent residency and arrived in Canada during the study period (“1986–2002 immigrants”). Data abstraction included year of arrival, age at arrival, sex and country of birth. 2) Immigrants who arrived before 1986: Canadian census data were used to estimate the size and age–sex distribution of the foreign-born permanent resident population in 1986 [19, 20].
Temporary foreign-born residents (visitors, students, workers and refugee claimants within the refugee determination process (whose status remained to be determined)) were excluded from the denominator as this information was not maintained by Citizenship and Immigration Canada.
TB cases
Foreign-born TB cases diagnosed during the study period were identified from the Canadian Tuberculosis Reporting System (CTBRS), a prospective national TB registry of all active cases. Cases were included in the study if immigration status at the time of diagnosis was reported as “permanent resident” or if immigration status was unknown. The diagnosis of active TB is based upon positive bacteriology in 80% of cases; in the remainder, it is based upon a standardised case definition [21].
WHO country groups
Countries of birth for 1986–2002 immigrants were divided into four groups based on the average country-specific WHO-estimated incidence rate of smear-positive TB in 1993–1995 [22]: <15 (group 1); 15–50 (group 2); 51–100 (group 3); and >100 (group 4) per 100,000 population (see supplementary material).
Statistical analysis
Time since arrival denotes the number of years between the year of arrival and the year of diagnosis. Cases diagnosed in the calendar year of arrival were categorised as year 0 cases (i.e. <1 yr since arrival), cases occurring in the calendar year following the year of arrival were year 1 cases, etc. Thus, cases diagnosed in year 1 could have been in Canada between 1 day and 2 yrs, or 1 yr on average.
Incidence rates per 100,000 person-yrs were calculated overall as well as for sex, age at arrival, country group and time since arrival strata. The calculation of 95% confidence intervals (CIs) for rates assumed a Poisson distribution for case counts. Standardised incidence rates were calculated using the direct method with the age and/or sex distribution of total 1986–2002 immigrants as the standard population. Rates were compared with incidence rate ratios (RR) and 95% CIs. Summary statistics consisted of the mean and standard deviation, and p-values were two-sided and considered significant if <0.05 [23].
The size of each annual cohort of immigrants for each year between their arrival and the end of 2002 was estimated with the age/sex/calendar year-specific survival rates of the total Canadian population [24–29]. Person-yrs of observation were obtained by adding annual cohort sizes over the total or partial observation period or across cohorts for a specific year. This was also performed for each sex, age at arrival and country group. In the year of arrival, each 1986–2002 immigrant was assumed to contribute 0.5 person-yrs. Person-yrs for pre-1986 immigrants were estimated with the same procedure except that each immigrant was assumed to contribute a whole year of observation in 1986.
The relative contributions of immigrants who had arrived 0–5, 6–10 and >10 yrs ago to the total burden of TB was assessed for those who arrived in 1986–2002 and for all immigrants. Of necessity, the latter group was limited to data from the 1995–2002 period, as 1995 was the earliest year in which all pre-1986 immigrants resided in Canada for >10 yrs after the arrival year.
Among 1986–2002 immigrants, the potential impact of prevalent active but unrecognised disease upon arrival on TB incidence rates in year 0–2 was explored with sensitivity analysis. Based on the assumption that a proportion of year 0–1 cases were actually active upon arrival (by inference to have developed TB between the date of the immigration medical examination (IME) and date of arrival), the absolute number of cases in year 0–1 were incrementally reduced until statistically insignificant RRs (year 0–2 compared with year 3–5) were observed.
Stata/IC 11.1 for Windows (StataCorp, College Station, TX, USA) was used for data analysis.
Ethics approval was not required as anonymous and routinely collected surveillance data were used.
RESULTS
The CTBRS received notification of 18,524 foreign-born TB cases during the study period. After excluding 1.3% of cases due to record errors, 18,275 were analysed: 8,662 (47.4%) among pre-1986 immigrants and 9,613 (52.6%) in 1986–2002 immigrants.
TB among pre-1986 immigrants
There were 3,860,853 immigrants who resided in Canada before 1986 [19]. During the study period, the TB rate in this group was 14.2 per 100,000 person-yrs. Higher rates were associated with males and those aged >64 yrs (table 1).
TB among 1986–2002 immigrants
There were 3,436,283 individuals who immigrated during the study period. The mean±sd annual immigration was 202,134±30,418 individuals, ranging from 113,513 in 1986 to 245,927 in 1990. The majority of immigrants (49.1%) were born in countries with TB incidence rates of 15–50 per 100,000 population. Nonetheless, a shift in immigration pattern to higher-incidence countries of birth was evident and primarily involved a progressive increase in the proportion of immigrants from WHO group 3 (51–100 per 100,000 population) (fig. 1), from 17.1% in 1986–1990 to 24.9% in 1998–2002.

Percentage of foreign-born permanent residents arriving annually in Canada between 1986 and 2002 from countries of birth grouped according to the country-specific World Health Organization-estimated incidence rates of smear-positive tuberculosis per 100,000 population at mid-study period (3-yr average).
The overall rate of TB among 1986–2002 immigrants was 34.3 per 100,000 person-yrs, i.e. 2.4 (95% CI 2.4–2.5) times that of pre-1986 immigrants. Males and those aged >64 yrs at arrival also had the highest TB rates (table 1).
Rates varied substantially by WHO country group and progressively increased from group 1 (<15 per 100,000 population) to group 4 (>100 per 100,000 population) (table 2). As a result, countries of birth within groups 3–4 (>50 per 100,000 population) were associated with two-thirds of TB cases and only one-third of arrivals.
TB rates generally decreased with increased time since arrival (fig. 2a) and this association persisted in stratified analyses (sex (fig. 2b), age at arrival (fig. 2c) and WHO group (fig. 3)). Consequently, the most critical period for TB incidence was between 0–2 yrs (table 3). Moreover, the rate in year 0–2 was 2.1 (95% CI 2.0–2.2), 3.0 (95% CI 2.8–3.2) and 4.6 (95% CI 4.2–5.1) times higher than that of year 3–5, 6–10 and 11–16, respectively. Sensitivity analysis revealed that TB rates in year 0–2 remained significantly higher than those of year 3–5 until the year 0–1 case count was reduced by >60%. It is also noteworthy that immigrants aged >64 yrs at arrival maintained higher rates than younger arrivals throughout the post-arrival period (fig. 2c).

Tuberculosis (TB) incidence rates by time since arrival among foreign-born permanent residents who both arrived in Canada and were diagnosed with TB in 1986–2002. a) Crude TB incidence rates. b) Sex-specific TB incidence rates. c) Rates stratified by age at arrival.

Tuberculosis (TB) incidence rates among foreign-born permanent residents who both arrived in Canada and were diagnosed with TB in 1986–2002, by time since arrival and country of birth group. Countries of birth were grouped according to the country-specific World Health Organization-estimated incidence rates of smear-positive TB per 100,000 population at mid-study period (3-yr average).
The overall TB rate of 1986–2002 immigrants did not fall below 15 per 100,000 person-yrs until >10 yrs after the year of arrival (table 3). However, immigrants aged ≥35 yrs at arrival and those from WHO country groups 3–4 (>50 per 100,000 population) continued to have rates in excess of 15 per 100,000 person-yrs.
Deconstruction of total foreign-born TB incidence in Canada
Among combined pre-1986 and 1986–2002 immigrants, those ≤5 yrs after the year of arrival (year 0–5) contributed a mean±sd of 41.8±4.0% of total foreign-born TB cases annually in 1995–2002. This proportion was remarkably similar to that of immigrants >10 yrs post-arrival (41.1±4.7%) despite a 3.5-fold difference in the average annual person-yrs of observation (1,132,351 versus 3,910,130 person-yrs in year 0–5 and year >10, respectively).
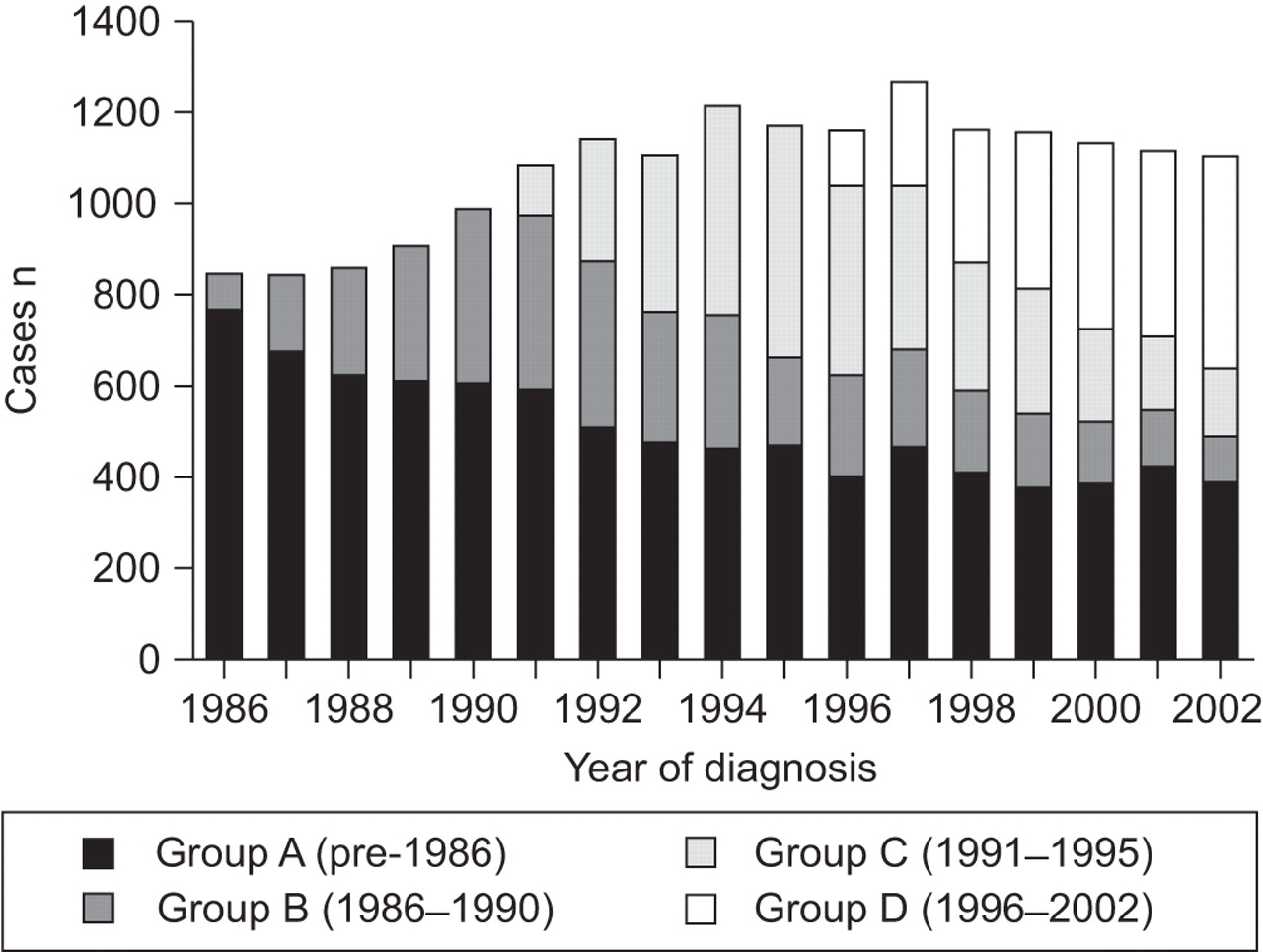
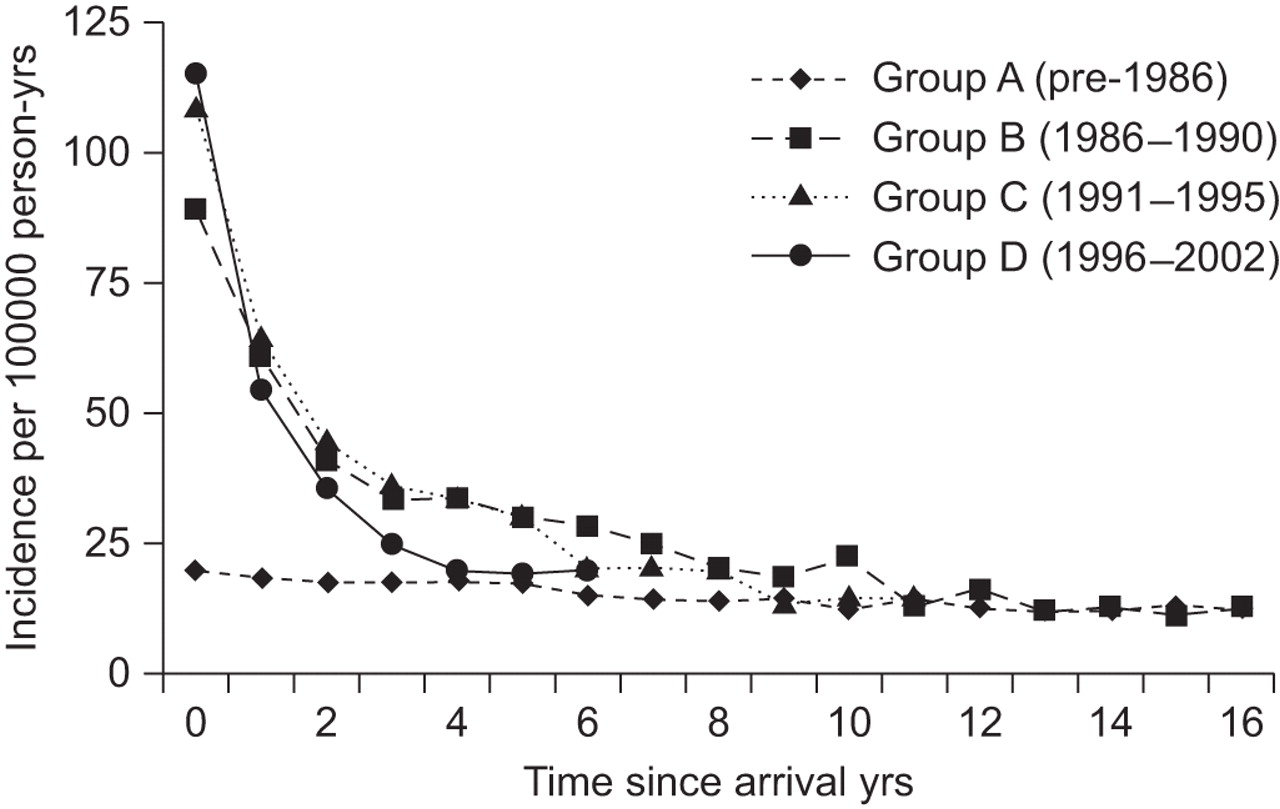
Cases were stratified into four groups (figs 4 and 5). Group A (pre-1986 immigrants) exemplifies what would have happened to foreign-born TB incidence if immigration was halted in 1986. As shown in figure 5, the rate in group A would have decreased significantly between the beginning and end of the follow-up period (RR 0.59 (95% CI 0.52–0.66); p<0.0001). Of note, however, is the relative stability in TB incidence in group A after 10 yrs (figs 4 and 5).

Annual tuberculosis case counts among foreign-born permanent residents in Canada grouped by period of arrival.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Annual tuberculosis incidence rates among foreign-born permanent residents in Canada by period of arrival and time since arrival, in 1986–2002.
The three remaining groups, composed of immigrant arrivals in 1986–2002, illustrated that newly arriving groups accounted for an increasing proportion of total cases (fig. 4). Specifically, the absolute number of cases contributed by group B (1986–1990 immigrants) progressively increased during the 5 yrs in which new members entered the cohort (“intake years”) and then progressively decreased once group B was closed to additional arrivals. As with group A, the incidence in group B was relatively stable once group B became composed exclusively of immigrants >10 yrs since the arrival year (figs 4 and 5).
Groups C (1991–1995 immigrants) and D (1996–2002 immigrants) had similar incidence patterns to group B (figs 4 and 5). Relative to group B however, the case count during the intake years of group C was 45.3% higher than that of group B (fig. 4). This coincided with an 11.5% increase in immigration levels in group C. Similarly, group D had a simultaneous 6.4% decrease in immigration level and 17.4% decrease in case count within its intake years compared with group C.
The proportion of immigrants from WHO groups 3–4 (>50 per 100,000 population) increased by 1.7% and 6.0% between groups B–C and groups C–D, respectively. While these shifts to higher incidence countries of birth coincided with progressively increased rates in year 1 (fig. 5), they appeared to have less of an influence on case counts than changes in immigration level.
DISCUSSION
In the present analysis of foreign-born TB incidence in Canada, immigrants’ greatest risk for active TB was within the first few years of arrival. Despite a 3.5-fold difference in annual person-yrs of observation, the pool of immigrants arrived ≤5 yrs ago and those arrived >10 yrs ago contributed almost equally to the annual foreign-born TB case count (42% and 41%, respectively). Clearly, events preceding and immediately following arrival of the foreign-born are critical for TB prevention and control.
As demonstrated in this study and others, there is a characteristic inverse relationship between foreign-born TB rates and increased time since arrival that persists regardless of demographic or country group [13–15]. The interval between the arrival year and the second year following the year of arrival (year 0–2) is of particular importance given a TB rate that is 2–3 times that of year 3–5 despite completion of immigration medical screening for pulmonary disease within a year of departure. Before permission for arrival is granted, all foreign nationals aged ≥11 yrs applying for permanent residency must undergo radiographic screening for pulmonary disease as part of the Canadian immigration medical screening process. Medical decisions rendered on the basis of the examination are valid for a period of 12 months, after which a repeat examination is required [21].
Although the existence of prevalent active disease upon arrival (and before departure) may contribute to high TB rates shortly after arrival, sensitivity analysis indicates that the TB rate in year 0–2 would remain significantly higher than that of year 3–5 even if only 40% of cases in the year of arrival and the year following the year of arrival were incidence cases. Similarly, it is unlikely that the described incidence trends were significantly altered by referral of high-risk immigrants (i.e. those diagnosed with inactive pulmonary TB during the IME) to medical surveillance programmes, due to the limited effectiveness of such programmes in preventing future TB cases [30, 31].
In contrast to TB incidence among immigrants arrived ≤5 yrs ago, TB incidence among those arrived >10 yrs ago is characterised by remarkably stable and relatively low TB case counts and rates (14 per 100,000 person-yrs). Nevertheless, these immigrants have a rate of TB that is 20 times that of Canadian-born non-Aboriginal persons [10].
Immigration is a dynamic process, with host countries frequently adjusting annual immigration targets and source countries of new immigrants in response to political, social and international factors [7]. In the current study, shifts in immigration pattern had a more subtle influence on TB incidence than that of changing immigration levels. That shifts in immigration pattern only had a minimal impact on TB rates after the arrival year presumably relates to the majority (>60%) of immigrants in Canada being born in countries with relatively low TB incidence (≤50 per 100,000 population). With continued shifts to higher-incidence source countries and immigration projected to represent an increasing proportion of population growth for the foreseeable future [6, 32], it is speculated that more marked increases in foreign-born TB case counts and rates are imminent.
That immigrants aged >64 yrs at arrival maintained substantially higher TB rates than younger arrivals throughout the post-arrival period is reasonably explained by ageing. In sub-group analyses, TB rates of pre-1986 immigrants aged >64 yrs in 1986 and 1986–2002 immigrants aged >64 yrs at arrival were found to progressively increase with each consecutive 5-yr increase in age (data not shown). The increasing likelihood of TB with the ageing of older arrivals emphasises the need for timely screening for LTBI, especially when immigrants originate from high-incidence countries and/or have other high-risk factors for the development of active disease.
The relative constancy seen in foreign-born TB incidence in Canada is the result of the convergence of all the factors discussed above. Clearly, strategies designed to reduce LTBI prevalence in the foreign-born will be critical to address the burden of TB within this vulnerable population, given this complex interplay of factors and previous findings suggesting that the majority of foreign-born TB cases in low-incidence countries result from reactivation of LTBI [33–35]. Although routine screening and treatment for LTBI in the foreign-born was previously discouraged due to poor cost-effectiveness [36], this strategy may emerge as a high priority and cost-effective reality in the near future due to technological advances. In particular, interferon-γ release assays, which add specificity to the tuberculin skin test [37, 38], have recently received approval in national guidelines and promising short-course LTBI treatment regimens on the horizon offer to improve acceptance and completion of treatment of LTBI [39–42].
Presumably, the cost-effectiveness of routine screening for LTBI is increased by targeting those at highest risk for TB. This study identified the highest-yield targets as being permanent residents ≤2 yrs post-arrival who were aged 15–34 yrs at arrival and born within countries with TB incidence rates >50 per 100,000 population. Although arrivals aged >64 yrs are at higher risk, they are not ideal targets for systematic screening due to higher rates of serious adverse effects of standard treatment for LTBI (9 months of daily isoniazid) [21, 43, 44]. Current guidelines for systematic screening of LTBI in the foreign-born should also be maintained to ensure that other high-risk, albeit lower-yielding, groups are appropriately managed. In Canada, this includes arrivals referred for medical surveillance by immigration authorities, children aged <15 yrs who are ≤2 yrs post-arrival from high-incidence countries (>15 per 100,000 population), and those foreign-born with high-risk medical conditions [21].
Should expanded LTBI screening and local public health responsibility emerge as a critical component of foreign-born TB control, it should not be undertaken to the exclusion of strategies aimed at reducing TB incidence in source countries. Enhanced national TB control programmes not only constitute the most cost-effective health intervention in resource-limited settings [45], but modelling also demonstrates that high-income countries can achieve cost-effective reductions in foreign-born TB morbidity and mortality by funding efforts to expand TB control in selected high-incidence countries [46].
The methodological strength of this study was the use of data from national TB and immigration databases. This methodology provided precise denominator and demographic information on a large study population over a prolonged period. Additionally, it eliminated the impact of post-immigration (secondary) migration within Canada and other jurisdictional limitations encountered with province-specific studies [14, 33, 47, 48], making it the most comprehensive report of foreign-born TB incidence in Canada to date.
This study had some limitations. Availability of year of arrival only, without day and month, for 59% of 1986–2002 immigrants necessitated an assumption about the person-yrs contributed. The resulting assumption of each immigrant contributing 0.5 person-yrs in the year of arrival reflects the distribution of arrivals with complete date of arrival information. Rate calculations may have been limited by mortality estimates and the assumption of no out-migration from Canada. An evaluation of TB among temporary foreign-born residents was beyond the scope of this study as the study population was limited to foreign-born permanent residents. This notwithstanding, incomplete data on immigration status within the CTBRS may have resulted in the inclusion of TB cases among temporary foreign-born residents. The overestimation in rates from such inclusions would be negligible, however, as temporary foreign-born residents account for only 5–9% of total foreign-born TB cases as per national [10] and province-specific data (S. Chorney, Database Manager, Alberta Health Services, Edmonton, AB, Canada; personal communication).
An area for future study is the potential impact of migrant type (economic, family reunification, refugee, skilled worker, etc.) on the distribution of TB in foreign-born populations. Immigration to highly developed economies is a dynamic process and migrants may not equally reflect the TB incidence rates of their place of origin.
With immigration being the single most important determinant of TB dynamics within high-income countries [5] and a demonstrated inability to make substantive reductions in foreign-born TB incidence using current guidelines [2, 9, 10, 16], the status quo is no longer acceptable if progress toward TB elimination is to be made in major immigrant-receiving countries.
Acknowledgments
The authors thank V. Gallant, Database Manager at the Public Health Agency of Canada (Ottawa, ON, Canada), for assistance with data retrieval.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support Statement
This work was funded, in part, by Citizenship and Immigration Canada and the Public Health Agency of Canada.
Statement of Interest
A statement of interest for B. Gushulak can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received December 20, 2010.
- Accepted February 20, 2011.
- ©ERS 2011
REFERENCES










