


Abstract
Epithelial sodium channel (ENaC) blockers have been proposed as a therapy to restore mucus clearance (MC) in cystic fibrosis (CF) airways. The therapeutic effects of the first generation ENaC blocker, amiloride, in CF patients, however, were minimal. Because the failure of amiloride reflected both its low potency and short duration of action on airway surfaces, we investigated whether the increased potency of benzamil and phenamil would produce more favorable pharmacodynamic properties. In vitro potency, maximal efficacy, rate of recovery from maximal block of ENaC, and rate of drug absorption were compared for amiloride, benzamil, and phenamil in cultured human and ovine bronchial epithelial cells. In both human and ovine bronchial epithelia, the rank order of potency was benzamil > phenamil » amiloride, the maximal efficacy was benzamil = phenamil = amiloride, the recovery to baseline sodium transport was phenamil < benzamil « amiloride, and the rate of drug absorption was phenamil > benzamil » amiloride. Based on greater potency, benzamil was compared with amiloride in in vivo pharmacodynamic studies in sheep, including tracheal mucus velocity (TMV) and MC. Benzamil enhanced MC and TMV, but acute potency or duration of effect did not exceed that of amiloride. In conclusion, our data support the hypothesis that ENaC blocker aerosol therapy increases MC. However, rapid absorption of benzamil from the mucosal surface offset its greater potency, making it equieffective with amiloride in vivo. More potent, less absorbable, third generation ENaC blockers will be required for an effective aerosol CF pharmacotherapy.
Innate defense against bacterial infection of the respiratory tract is provided in a large part by MC (Adler et al., 1973; Wanner et al., 1996; Talbot et al., 1997; Houtmeyers et al., 1999; Robinson et al., 2000; Knowles and Boucher, 2002). Clearance of pathogens and toxins from airway surfaces occurs by the continuous cephalad movement of both the periciliary and mucous layers that comprise the thin film of airway surface liquid (ASL) that lines the lumen of the respiratory tract (Matsui et al., 1998b). The kinetic energy required for the cephalad movement of the ASL is provided by the coordinated beat of the underlying cilia (Wanner et al., 1996; Matsui et al., 1998b). If the cilia are nonfunctional, e.g., in patients with primary ciliary dyskinesia (Min et al., 1995; Bush, 2000; Regnis et al., 2000), or if the periciliary layer of ASL is depleted due to reduced chloride secretion and hyperabsorption of sodium ions as manifested in patients with cystic fibrosis (CF) (Matsui et al., 1998a; Tarran et al., 2001; Puchelle et al., 2002), mucostasis develops, and persistent chronic respiratory infections result.
A proposed therapy directed at the ASL volume depletion of CF is aerosolized amiloride. Amiloride, “a potassium-sparing diuretic”, is a relatively selective ENaC blocker. The proposed mechanism of amiloride action is an open channel block in the exofacial domain of ENaC (Horisberger, 1998). Evidence supporting the sodium channel blocker ASL-rehydration paradigm has emerged from both in vitro data, measuring amiloride effects on transepithelial bioelectric correlates of electrogenic sodium absorption and on ASL height (volume) of primary cultured human bronchial epithelial (HBE) cells (Grubb et al., 1997; Tarran et al., 2001; Hirsh, 2002) and in vivo data, measuring the effect of aerosolized amiloride on ASL volume in sheep (Mentz et al., 1986) and MC in normal human airways (Sood et al., 2003). Acute studies of the effect of aerosolized amiloride on MC in CF subjects suggested amiloride was active but was of short duration (Kohler et al., 1986). The effects of chronic aerosolized amiloride therapy on pulmonary function were studied; however, no agreement regarding therapeutic effect was established (Kohler et al., 1986; App et al., 1990; Knowles et al., 1990; Graham et al., 1993; Bowler et al., 1995; Pons et al., 2000). The poor performance of aerosolized amiloride therapy in CF patients was attributed to low potency and insufficient drug delivery so that complete block was not achieved (Hofmann et al., 1997; Pons et al., 2000). Rapid absorption (Mentz et al., 1986; Noone et al., 1997; Hirsh, 2002) and rapid reversal from ENaC block (Hirsh, 2002) also limited the clinical utility of amiloride.
Two second generation amiloride analogs, benzamil and phenamil, have been considered as alternatives to amiloride for CF pharmacotherapy (Blank et al., 1997; Hofmann et al., 1998; Rodgers and Knox, 1999). Benzamil and phenamil have substituted benzyl and phenyl groups, respectively, on the terminal nitrogen atom of the guanidino moiety of amiloride (Fig. 1) and are significantly more potent than amiloride. Benzamil reportedly is 9-fold and phenamil 17-fold more potent than amiloride when tested in the same (Stutts et al., 1995) or different tissue models (Kleyman and Cragoe, 1988). The reported pKa values of benzamil and phenamil are 8.1 and 7.8, respectively, compared with amiloride at 8.8 (Kleyman and Cragoe, 1988). The pKa results indicate that both benzamil and phenamil at physiologic pH (∼7.2) are less protonated and more lipophilic (11- and 20-fold, respectively) than amiloride (Kleyman and Cragoe, 1988). This feature raises the question of whether increased absorption from airway surfaces due to lipophilicity may offset the increased potency of benzamil or phenamil.

Ground state structure of amiloride (a), phenamil (b), and benzamil (c) in their unprotanated forms.
In the present study, we tested a series of in vitro parameters in an attempt to select between benzamil and phenamil as a potential follow-on candidate to amiloride. These parameters included: potency (IC50), the rate of recovery of sodium absorption in response to wash with drug-free solution after maximal ENaC block, and the rate of absorption from HBE and ovine bronchial epithelial (OBE) cells. Based on the criteria of increased potency and maximal residency time, one compound was selected for in vivo pharmacodynamic comparison with amiloride in sheep TMV and MC assays.
Materials and Methods
Cell Culture. Isolated HBE and CF bronchial cells used for primary culture were provided by the Tissue Culture Core of the Cystic Fibrosis Center at University of North Carolina (Chapel Hill, NC) under the auspices of protocols approved by the Institutional Committee on the Protection of the Rights of Human Subjects. Human bronchial tissue was harvested from excess tissue from donor lungs at the time of lung transplantation from a portion of the main stem or lumbar bronchi. The OBE cells for primary culture were provided by the Mount Sinai Medical Center from animals undergoing scheduled sacrifice, which was approved by the Mount Sinai Animal Research Committee to ensure the humane care and treatment of experimental animals. Briefly, ovine or human bronchi were incubated in minimum Eagle's medium containing 0.1% protease (Sigma Type XIV) and 1 μg/ml DNase at 4°C for a minimum of 24 h. Fetal bovine serum (10%) was added to the medium, and cells were centrifuged for 5 min at 500g. Resuspended cells were seeded at a density of 0.25 to 0.4 × 106/cm2 on 12-mm, 0.4-μm porous Transwell-Col or collagen-coated (human placenta type VI Sigma) Snapwell membranes (1.13 cm2) and maintained at an air-liquid interface (ALI) in hormonally defined medium supplemented with penicillin (50 units/ml) and streptomycin (50 ng/ml) (Matsui et al., 1998b). To assay for the integrity of the well differentiated primary airway epithelial preparations, we routinely measured transepithelial resistance (Rt) and transepithelial potential difference. Primary cultures having an Rt below 100 Ω cm2 were discarded from the study.
Bioelectric Characterization. Primary bronchial epithelial cultures, at an ALI for no less than 6 days on Snapwell collagen-coated (0.75 mg/ml) permeable supports (Costar, Cambridge, MA), were mounted in modified Ussing chambers (Physiologic Instruments Inc., San Diego, CA). All Ussing chamber and drug transport experiments were performed in Krebs-Ringer bicarbonate solution (KRB), pH 7.4, containing: 140 mM Na+, 120 mM Cl–, 5.2 mM K+, 1.2 mM Ca2+, 1.2 mM Mg2+, 2.4 mM HPO42+, 0.4 mM H2PO4–, 25 mM HCO3–, and 5 mM glucose, unless otherwise specified. The epithelium was bathed on both sides with warmed (37°C) KRB circulated by gas lift with 95% O2/5% CO2, maintaining the pH at 7.4. The transepithelial voltage was clamped to 0 mV, except for 3-s pulses (+10 mV) every 60 s to calculate Rt. Short-circuit current (Isc) and Rt were digitized and recorded on a computer. Data were acquired and analyzed using Acquire and Analysis (version 1.2) software (Physiological Instruments). IC50 was calculated from apical drug additions ranging from 10–11 to 10–4 M (∼half-log increments) and analyzed using nonlinear regression (Prism version 3; GraphPad Software Inc., San Diego, CA). Stocks of amiloride, benzamil, and phenamil were dissolved in dimethyl sulfoxide at a concentration of 10 mM and stored at –20°C until use.
The percent recovery of Isc from apical sodium channel blocker exposure to HBE cells was measured using two separate protocols: the Isc 3 min after three consecutive mucosal bath replacements (KRB), following a full concentration-effect study divided by predrug Isc × 100; and Isc following a rapid perfusion (13 volumes) of the mucosal bath with KRB after a short (30 s) exposure of a maximally effective concentration of sodium channel blocker divided by predrug Isc × 100.
Amiloride, Benzamil, and Phenamil Absorption by Human or OBE Cells. Transport characteristics of amiloride, benzamil, and phenamil were measured using HBE and OBE cells grown at an ALI for no less than 14 days on Transwell collagen-coated permeable supports (Costar). An equimolar concentration of amiloride, benzamil, or phenamil (10 μM; 25 μl) was added to the apical surface, and 1-μl samples were collected from the mucosal compartment at 2, 15, 30, 90, 180, and 240 min. In parallel, 250-μl samples were collected from the serosal compartment at 0, 30, 60, 90, 120, 150, 180, 210, and 240 min. The drug concentration in each sample was measured (see below), and rates of disappearance from the apical compartment and appearance in the serosal compartment were calculated.
Reverse-Phase High-Performance Liquid Chromatography Analysis. All samples obtained from the absorption assays were applied to a 150-× 4.6-mm i.d., C18, 5-μm Prevail column (Alltech Associates, Deerfield, IL) maintained at 40°C. Elution of sodium channel blockers was achieved with a 12-min, mobile phase consisting of a 0.02% trifloro acetic acid, pH 3.0/acetonitrile linear gradient (95:5–56:64) at a flow rate of 1.5 ml/min. The column was monitored by an online fluorescence detector (λ = 362 nm, excitation; 412 nm, emission) (Waters, Milford, MA).
Permeability Coefficients for Mannitol and Benzamil. Primary HBE cells (10–20 days after forming an ALI) were mounted in modified Ussing chambers with an aperture of ∼1.13 cm2, as described above. The permeability coefficients (Pcoeff) for benzamil and mannitol were measured under voltage-clamped conditions. Following a 45-min equilibration period with [14C]benzamil and [3H]mannitol in the mucosal bath, aliquots (500 μl) from the serosal bath (sink) were collected every 30 min and replaced with 500 μl of KRB. Every 60 min, 50 μl was collected from the mucosal bath (source). The quantities of [14C]benzamil and [3H]mannitol in the source and sink side were measured using a liquid scintillation counter (Beckmen LS 6500), and the Pcoeff were calculated using an established equation (Gatzy, 1975). The units of Pcoeff are centimeters per second.
Confocal Studies of Cellular Uptake. Benzamil is an aromatic compound and is highly fluorescent, exhibiting an excitation maximum in the ultraviolet spectrum (362 nm) and an emission maximum of approximately 412 nm. Primary HBE cells were placed in an apparatus designed to position transwell membrane supports on a confocal microscope stage (Leica, Wetzlar, Germany). The glycocalyx and cilia were labeled with 3 μM wheat germ agglutinin-fluorescein (Molecular Probes, Eugene, OR) for 45 min at 37°C to visualize the apical domain of HBE cell cultures. The autofluorescence of the cells was acquired prior to apical compound addition. Images were acquired with a 63× water immersion lens in the x-z plane. Benzamil was added to the mucosal compartment (10 μM; 350 μl), and images were recorded serially from 0 to 5 min.
Animal Preparation for in Vivo Studies. The procedures used in this study were approved by the Mount Sinai Animal Research Committee to ensure the humane care and treatment of experimental animals and were similar to Sabater et al. (1999). Briefly, adult ewes weighing 25 to 35 kg were placed in a restraint and positioned upright using a specialized body harness. The heads of the animals were immobilized, and local anesthesia of the nasal passage was provided (2% lidocaine) prior to nasal intubation [7.5-mm i.d. endotracheal tube (ETT); Mallinckrodt, St. Louis, MO]. The cuff of the ETT was placed just below the vocal cords. After incubation, the animals were allowed to equilibrate for approximately 20 min before either TMV or MCC measurements began.
TMV Measurement. Eight to 10 radiopaque Teflon disks (∼1 mm in diameter, 0.8 mm thick, and weighing between 1.5–2 mg) were introduced into the trachea via the ETT. The particles were insufflated by a catheter connected to a source of compressed air (flow rate of 3–4 ml/min at 50 psi). The catheter was removed following insufflation without contacting the tracheal surface. To minimize the ETT effects on TMV, the cuff was deflated throughout the study except for the period of drug delivery. The disk movements were recorded using videotaped fluoroscopy, and individual disk velocities were calculated by measuring the distance traveled by each disk over a 60-s period. A collar containing radiopaque markers of predetermined length was placed around the animal's neck, which was used as a standard to correct for magnification effects intrinsic to the fluoroscopy unit. The mean value of disk velocities was calculated for each time point. To avoid dehydration, the sheep were periodically gavaged with tap water via a nastrogastric tube. To avoid desiccation of the tracheal mucosa caused by sustained intubation, the inspired air was warmed and humidified by a Bennet Humidifier (Puritan-Bennett, Lenexa, KS).
The protocol was a randomized crossover design. The study solutions were aerosolized from a 4-ml volume via a Pari LC Jet Plus nebulizer (Pari Respiratory, Richmond, VA) to free-breathing sheep. The nebulizer had a flow rate of 8 L/min (compressed air), which produced a droplet with a median aerodynamic diameter of ∼5 μm. The time to deliver the solution was 10 to 12 min. A baseline measurement was initially obtained, followed by aerosolization of either 4 ml of sterile H2O (vehicle), amiloride (3 mM), or benzamil (3 mM). The TMV measurements were made immediately after aerosolization and at 15, 30, and 45 min and 1, 2, 3, and 4 h after administration of the test agent.
MC Measurement. Aerosols of human serum albumin radiolabeled with technicium (99mTc-HSA 3.1 mg/ml, ∼20 mCi) were generated by a raindrop nebulizer (Nellcor Puritan Bennett, Pleasanton, CA) that produces a median aerodynamic droplet diameter of 3.6 μm. The nebulizer was connected to a dosimeter system consisting of a solenoid valve and a source of compressed air (20 psi). The output of the nebulizer was directed into a T piece, with one end attached to a respirator (Harvard Apparatus Inc., Holliston, MA). The system was activated for 1 s at the onset of the respirator's inspiratory cycle. The tidal volume was set at 500 ml, with an inspiratory/expiratory ratio of 1:1 and a rate of 20 breaths/min to maximize central airway deposition. The sheep breathed the 99mTc-HSA aerosol for a total of 5 min. Following tracer deposition, a gamma camera was used to measure the clearance of 99mTc-HSA from the airways. The camera was positioned above the animal's back with the sheep in its natural upright position in the harness. The field of the image was perpendicular to the animal's spinal cord. External radiolabeled markers were placed on the sheep to facilitate proper alignment of the gamma camera. A region of interest was traced over the image corresponding to the right lung of the sheep, and counts were recorded. The counts were corrected for decay and expressed as a percentage of radioactivity present in the baseline image. The left lung was excluded from the analysis because the outline of the lung was superimposed over the stomach, and counts could be affected by swallowed 99mTc-HSA-labeled mucus. All deposition images were stored on a computer hard drive interfaced to the gamma camera. The protocol included a baseline deposition image obtained immediately postradio aerosol administration. After acquisition of baseline images, 4 ml of H2O (vehicle), amiloride (3 mM), or benzamil (3 mM) was aerosolized using the Pari LC JetPlus nebulizer to free-breathing sheep. The nebulizer had a flow rate of 8 L/min. The time to deliver the solution was 10 to 12 min. On the completion of compound administration, the animal was immediately extubated to prevent false elevations in counts due to aspiration of excess 99mTc-HSA-labeled mucus from the ETT. Serial measurements of 99mTc-HSA retained in the lung were obtained over a 4-h period at 20-min intervals for the first 2 h and then every hour. A washout period of at least 7 days (half-life of 99mTC = 6 h) separated studies with the different agents.
Materials. Cell culture media, bovine serum albumin, fetal bovine serum, bovine pituitary extract, epidermal growth factor, penicillin, retinoic acid, DNase, human placenta collagen VI, streptomycin, amiloride, benzamil, phenamil, and lidocaine were purchased from Sigma-Aldrich (St. Louis, MO). d-[1-3H(N)]-mannitol and [14C]-benzamil were purchased from PerkinElmer Life and Analytical Sciences (Boston, MA). The 99mTc-Human Serum Albumin was purchased from Mallinckrodt. Salts and solvents were of analytical or high-performance liquid chromatography grade and purchased from VWR (West Chester, PA).
Statistical Analysis. All values are depicted as the mean ± S.E.M. unless otherwise specified. Paired and unpaired Student's t tests were performed on in vitro data to identify significant differences between paired and unpaired data sets, respectively. A one-way ANOVA followed by a Newman-Keuls multiple comparison test was used to determine significant differences for reversibility data. TMV and MC in vivo data were fitted using a cubic spline curve fit and nonlinear regression, respectively, and analyzed using a paired two-way ANOVA with repeated measures, followed by a paired Student's t test to identify differences between specific pairs at specific time points. To indicate differences in the rapid clearance phase (initial to approximately 90 min) among vehicle, amiloride, and benzamil in MC data, we used linear regression analysis and applied a one-way ANOVA followed by a Newman-Keuls multiple comparison test. Linear regression and curve fits were performed using the program GraphPad Prism (version 3.0).
Results
Sodium Channel Blocker Potency, Maximal Efficacy, and Recovery. To measure the potency and maximal efficacy of sodium channel blockers in both HBE and OBE cells, we measured the ΔIsc in response to increasing concentrations of apical amiloride, benzamil, or phenamil (10–11-10–4 M.) In both HBE and OBE cells, active sodium transport was the dominant component of Isc as evidenced by the observation that maximal effective concentrations of each blocker decreased the Isc to approximately 9% of the baseline value (Fig. 2A). The residual Isc likely reflects the induction of chloride secretion (Boucher, 1994).

A, representative Isc concentration-effect relationships for amiloride (•), benzamil (▴), or phenamil (□) (0.01 nM–62 μM) in HBE cells. Inset, raw data describing concentration-effect relationship of amiloride, benzamil, and phenamil on HBE cells. B, representative Isc concentration-effect relationship of amiloride (•), benzamil (▴), or phenamil (□) (0.01 nM–16 μM) in OBE cells. The epithelia were equilibrated for 10 to 20 min in drug-free KRB prior to compound administration to allow for a steady basal Isc. The OBE cells were slightly more sensitive (Isc response) to vehicle (dimethyl sulfoxide) administered at the highest dose (62 μM), so this dose was not included in constructing a concentration-effect relationship. Values plotted are those collected 1 min postadministration of each dose of compound to the mucosal bath.
For OBE cells, the sodium channel blockers were less potent (up to 2-fold) compared with HBE cells (Table 1). However, a slightly greater maximal efficacy (Isc decreased to 0–1% of the initial baseline value) was measured in OBE cells (Fig. 2B). Similar to the human data, the shape of the concentration-effect curve was sigmoidal and similar to a drug-receptor binding complex curve exhibiting saturable binding. The fold difference compared with amiloride was 13.2 and 5.2 greater for benzamil and phenamil, respectively, and the rank order of potency paralleled that observed in HBE cells (benzamil > phenamil » amiloride) (Table 1). When measuring Isc after maximal sodium channel block (maximal efficacy), a zero to slightly negative current was monitored. We suspect that this negative current is due to a small rate of cation secretion, likely a potassium current, due to its sensitivity to barium (Burleigh, 2003).
Mucosal concentration of sodium channel blockers required to inhibit 50% of short-circuit current by HBE and OBE cells
Values represent mean ± S.E.M.; n equals the number of observations. The IC50 value was calculated fitted to a nonlinear regression sigmoidal dose-response curve with no weighting.
For HBE cells, the shape of the concentration-effect curve using a four-parameter fit is similar to a drug-receptor binding complex curve (Fig. 2A). The rank order of potency was benzamil > phenamil » amiloride, and the fold difference compared with amiloride was 7.9 and 3.8 for benzamil and phenamil, respectively (Table 1). To determine whether CF bronchial epithelia respond similarly to HBE cells, we measured the potency of benzamil on CF bronchial epithelia and calculated an IC50 of 38 nM. The qualitative difference of Isc when exposed to phenamil from both HBE and OBE cells over the full concentration range was significantly different when compared with amiloride and benzamil (Fig. 2A, inset). The inhibition of Isc exhibited a markedly different step-wise pattern as compared with benzamil or amiloride.
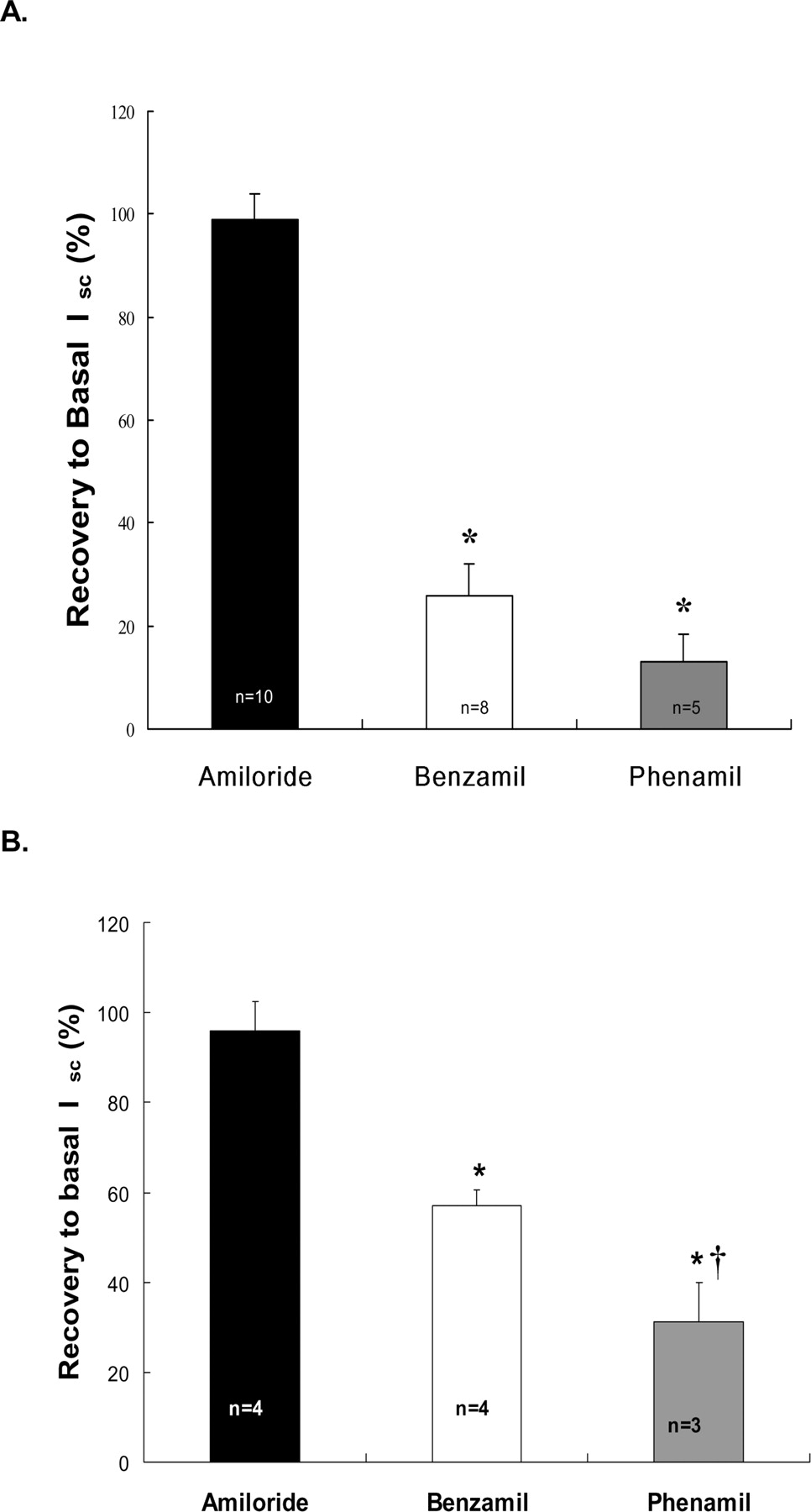
Besides potency, the off rate of the blocker from the targeted protein (ENaC) likely would affect durability in vivo. As a macroscopic estimation of off rates, we measured the reversibility of block (with wash) after achieving maximal sodium channel inhibition. After a full concentration-effect curve (∼40 min) and three apical washes (Fig. 3A), full recovery to basal values was observed for amiloride (99 ± 5.3%), whereas benzamil and phenamil only recovered partially, 26 ± 6.3 and 13 ± 5.3%, respectively. A second protocol was used on a separate set of HBE cells to test for the effects of duration of drug exposure on reversibility. In this protocol, basal Isc measurements were obtained, cells exposed to a short (30 s) pulse of a maximal concentration (100 μM) of a blocker, following which the apical surface was washed exhaustively (13 volumes), and Isc was continuously recorded. The amiloride block was again totally reversible (96 ± 6.7%). Benzamil and phenamil again recovered only partially (57 ± 3.4 and 31 ± 8.8%, respectively; Fig. 3B), but the reversal was greater than after prolonged drug exposure. Using both protocols, no significant decay in basal current was noted over the duration of exposure or recovery intervals for control (untreated) tissues. To determine whether the partial benzamil or phenamil reversibility of Isc reflected toxicity, a further rigorous mucosal washing was performed (39 volumes). With time, the Isc recovered to near basal levels (92 ± 4.7 and 84 ± 7.5%, respectively).

A, percent reversal of Isc block postconcentration-effect relationship to baseline value (see Fig. 2A) following three consecutive mucosal bath replacements (5 ml). Values reported are the mean ± S.E.M. n, number of observations, where 100% represents complete reversal, i.e., recovery to the starting basal current prior to compound administration. B, percent reversal Isc after a 30-s, 100 μM exposure to amiloride, benzamil, or phenamil with rapid 13-volume mucosal bath replacements in HBE cells. *, significance (P < 0.001) compared with values obtained with amiloride; †, significance (P < 0.05) between benzamil and phenamil.
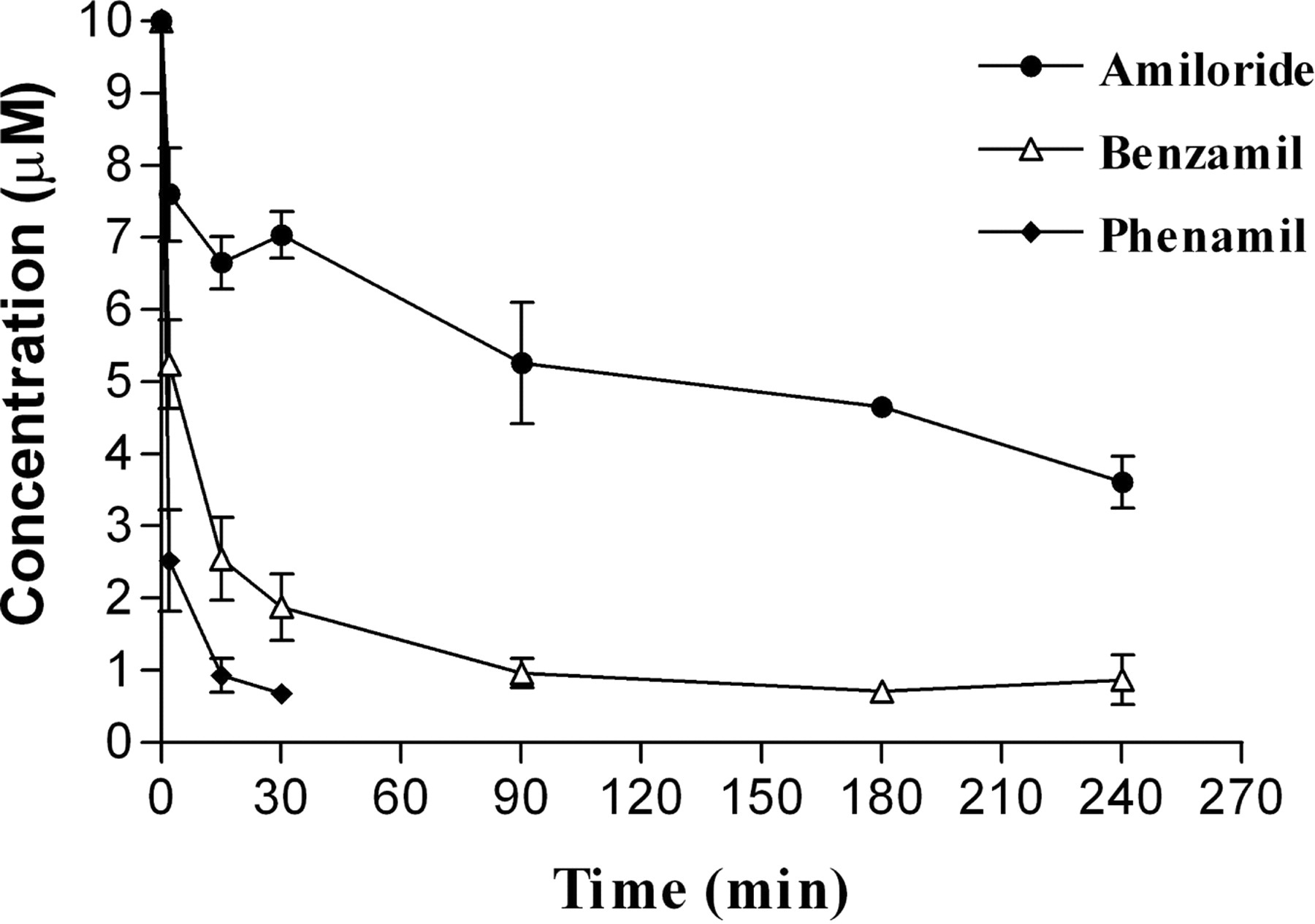
Drug Absorption by Bronchial Epithelia. The retention of sodium channel blockers within the surface liquid bathing the epithelial surface will be a major parameter contributing to the durability of pharmacological effect in vivo. The total soluble fractions of amiloride, benzamil, and phenamil remaining in the apical surface liquid of HBE cells over a period of 0 to 4 h are shown in Fig. 4. The rank order of free concentration of drug remaining in the ASL was amiloride » benzamil > phenamil.

Apical surface liquid concentration of amiloride (•), benzamil (Δ), or phenamil (♦) on HBE cells with time. Amiloride, benzamil, or phenamil (10 μM; 25 μl) were added to the apical surface, and samples were collected from both the apical and the serosal compartment from 0 to 4 h. Phenamil values after 30 min were below the lower limits of detection and, therefore, are not displayed (values are the mean ± S.E.M., n = 8).
The rates of mucosal disappearance and serosal appearance of free, unbound compound are presented in Table 2. The rate of mucosal disappearance of benzamil and phenamil were approximately 3.3 and 4.5 times faster than amiloride in HBE cells, respectively. Furthermore, the rate of appearance in the serosal bath maintained the same rank order (phenamil » benzamil > amiloride) found for the mucosal disappearance rate; however, the rate of appearance of benzamil and phenamil compared with amiloride was lower (1.3 and 3.2, respectively) than the mucosal disappearance rate. No evidence of biotransformation of any compound was detected in either the apical or serosal compartments after incubation with HBE or OBE cell cultures. Interestingly, all sodium channel blockers appeared to be absorbed much more rapidly from the apical surface of OBE than HBE cell cultures. Mucosal disappearances, however, could not be accurately measured due to the induction of liquid secretion by OBE cells following addition of sodium channel blockers. However, a similar rank order of absorption as in HBE cells (phenamil > benzamil = amiloride) was observed, and based on estimates from the secretion rate, the absolute rates of absorption by OBE cells of each compound was greater than (approximately 2.6-fold) HBE cells. More quantitative evidence for greater compound absorption is apparent for the greater rates of serosal appearance of compounds in OBE cells as compared with HBE cells.
The rates of sodium channel blocker transport (pg/cm2/min) by HBE and OBE cells
Mucosal disappearance values are initial rates from 0 to 30 min; serosal appearance values are initial rates from 0 to 150 min for HBE cells and 0 to 90 for OBE cells. OBE cell mucosal disappearance values were not included due to substantial dilutions caused by continuous basal secretions. Values represent mean ± S.D.
Mucosal to Serosal Pcoeff of Benzamil and Mannitol by HBE Cells. To test whether benzamil was absorbed via a transcellular pathway, we measured the rates of permeation of [14C]benzamil and [3H]mannitol, a paracellular marker in HBE cells. As shown in Fig. 5, benzamil exhibited a markedly greater rate of permeation as compared with mannitol (Pbenz/Pmann ratio of 15.2:1), suggesting that benzamil is likely transported transcellularly by diffusional and/or carrier-mediated mechanisms.

Mucosal to serosal permeation of benzamil and mannitol across HBE cells. [14C]Benzamil (5 μM) and the paracellular marker [3H]mannitol were added to the mucosal bath of HBE cells, and samples were collected over 120 min to calculate the benzamil and mannitol Pcoeff. *, significance (P < 0.05) compared with mannitol (values are the mean ± S.E.M., n = 4).
Confocal Images of Benzamil Absorption by HBE Cells. To test further whether benzamil was absorbed transcellularly, we visualized benzamil (red color) in the surface liquid bathing HBE cell cultures (Fig. 6). The glycocalyx and cilia were labeled with wheat germ agglutinin (green color) to demarcate the apical membrane. Within 30 s, benzamil penetrated the apical membrane. The merged color (yellow) indicated that benzamil perhaps is also binding to the glycocalyx and cilia (30–300 s). After a 5-min apical exposure to benzamil, the cytosol had accumulated and concentrated benzamil.

Transepithelial transport of benzamil by HBE cells. Confocal images in the x-z plane from the same area of HBE cells before and after the addition of benzamil (10 μM) to the mucosal surface. To provide orientation, the cilia and glycocalyx were labeled with wheat germ agglutinin fluorescein (3 μM) (green color). The permeable support membrane is indicated by the white horizontal line. Benzamil is depicted in red. Images were captured at the time indicated (in seconds).
Ovine TMV and MC. Benzamil demonstrated the more favorable ratio of potency versus absorption as compared with phenamil. Therefore, we tested whether benzamil is more effective than amiloride at enhancing airway mucus clearance using two in vivo assays, TMV and MC.
The TMV response for amiloride, benzamil, and vehicle are illustrated in Fig. 7. Aerosolization of sterile H2O (vehicle) produced a small increase in tracheal mucus velocity 5.0 ± 1.1% above baseline (100%) at 15 min, which was followed by drift below baseline thereafter. In contrast to control values, statistically significant increases in TMV were observed 15 min following the administration of equimolar amounts of either amiloride or benzamil, where the maximum stimulation of TMV was observed. After 15 min, TMV declined for all groups including vehicle control (most apparent in the 1- to 4-h interval); however, statistically significant differences for amiloride and benzamil versus vehicle were apparent throughout the remainder of the 4-h observation period. The rate of decline in TMV for all groups was comparable. No differences were found by comparing the effect of treatment with benzamil to amiloride on TMV at any time point.

Effect of aerosolized amiloride (3 mM) (○), benzamil (3 mM) (▾), or vehicle [H2Osterile (ddd)] (4 ml) (▪) on sheep TMV. Values are mean ± S.E.M. for four animals. Data were fitted with a cubic spline curve fit. *, significance (P < 0.05) of amiloride and benzamil from vehicle control.
MC was expressed as the relative percent of inhaled radiolabel retained in a specific region of the lung over time. Aerosol dosing of vehicle or equimolar concentrations of amiloride or benzamil increased the rate of MC and were significantly different (P < 0.001) (Fig. 8A). In Fig. 8B, a comparison in the rapid clearance phase (initial to 90 min) from vehicle, benzamil, or amiloride from the MC data using linear regression analysis indicated that the decrements of MC were similar for amiloride and benzamil (–23.5 ± 2.0 and –20.0 ± 1.4), respectively; however, both rates of MC were significantly enhanced (P < 0.001) compared with vehicle control (–9.6 ± 1.7; Fig. 8B). The slopes approximated vehicle thereafter (Fig. 8A).

Effect of aerosolized amiloride (3 mM), benzamil (3 mM), or vehicle [H2Osterile (ddd)] (4 ml) on sheep MC. A, effect of vehicle (▪), amiloride (○), or benzamil (▾) on MC over the duration of the experiment (4 h). A decrease in percent retention for the MC plot indicates an enhanced rate of clearance. Data were fitted with nonlinear regression curve fit. *, where the change in retention was significantly different (P < 0.05) from vehicle at selected time points. B, data from initial to 90 min taken from A, fit using linear regression analysis. Values are mean ± S.E.M. for four animals.
Discussion
In contrast to the kidney, sodium transport by the lung is not important for overall body sodium homeostasis but is critical in regulating ASL height and MC. This relationship was revealed in patients with pseudohypoaldosteronism. From a respiratory systems perspective, patients with this syndrome, which is a homozygous genetic disorder associated with loss of function in ENaC, exhibit no airway epithelial sodium transport, increased ASL volume, and very high basal rates of MC (Kerem et al., 1999; Prince et al., 1999). The pathogenesis of CF, appears to reflect the opposite sequence, i.e., raised sodium transport, diminished ASL volume, and reduced MC and ineffective cough clearance (Matsui et al., 1998a; Puchelle et al., 2002; Mall et al., 2004). Accordingly, an effective therapy for patients with CF will be a chemical entity that will restore ASL volume and MC in the respiratory tract for extended periods of time. To produce a long-acting enhancement of MC in CF, a drug will require properties that maintain activity at the target protein. Because the rate-limiting element for sodium transport, ENaC, is expressed at the lumenal surface, it is likely that drugs that block ENaC will be efficacious if delivered by the aerosol route. Accordingly, potency, absorption, and metabolism are all parameters that will contribute to the duration of action of a compound delivered by aerosol to the airway surface and, hence, predict therapeutic efficacy.
Amiloride specifically inhibits sodium entry across the apical membrane of many epithelia of the body at submicromolar concentrations. One reason for the poor performance of amiloride as an aerosolized drug for CF lung disease is that the compound does not exhibit the durability required to be an effective CF therapeutic agent (Graham et al., 1993; Hirsh, 2002). Amiloride was originally designed to be delivered orally and act primarily as a potassium-sparing diuretic. The data in this study illustrate why amiloride was not effective as a topical agent on the airway surfaces. Amiloride is the least potent and the most reversible of the three ENaC blockers tested (Figs. 2 and 3; Table 1). Amiloride exhibited a rate of absorption (mucosal to serosal transfer) (Fig. 4; Table 2), predicted to deplete the ASL of an effective concentration of drug in vivo rapidly. Indeed, the relatively rapid absorption correlates well with the short t1/2 (∼20–30 min) of drug in ASL measured using (14C)-labeled amiloride in vivo (Noone et al., 1997). The low potency on ENaC, rapid recovery from maximal block, and the short period of time that amiloride is present at concentrations that are significantly in excess of the EC50 projects a short duration (∼60 min) of pharmacodynamic effect (MC) (Sood et al., 2003). These features of the drug, combined with the inability to deliver a sufficient mass of drug (due to poor drug solubility in aqueous solution; Hofmann et al., 1997) likely account for minimal therapeutic effect of amiloride in patients with CF.
We next evaluated two second generation amiloride analogs, benzamil and phenamil, in vitro for potency, reversibility, and duration of action. With respect to potency on ENaC, our finding that benzamil is more potent than phenamil is not in agreement with early studies performing similar structure-activity relationships with similar tissues (Stutts et al., 1995) or different tissue models (Kleyman and Cragoe, 1988). One study (Blank et al., 1997), however, reported that phenamil was not as potent as benzamil at blocking ENaC in human airway epithelia. The differences in rank order likely reflect variations in raw data collection. Phenamil exhibited a slower onset of action and markedly different concentration-effect relationship on Isc compared with amiloride and benzamil (Fig. 2A, inset). A likely scenario is that the rapid effect of phenamil is to block ENaC followed by the slower phase of Isc reduction through a secondary block of other ion channels possibly K+ or Ca+ (Guia et al., 1995, 1996) or inhibiting the sodium/potassium pump (Kleyman and Cragoe, 1988), which is likely a consequence of intracellular accumulation of phenamil. We based our data collection time for phenamil on the equilibration of maximal inhibition on ENaC exhibited by both amiloride and benzamil, which achieved rapid equilibration (approximately 40–100 s). Although the CFTR regulatory component of EnaC is absent in CF airway epithelia, the relative potencies (IC50) of amiloride (Knowles et al., 1983) and benzamil on ENaC were similar to normal nasal and HBE cells, respectively. These observations suggest that the interactions of these blockers with ENaC using normal HBE cells likely reflect what would be achieved in CF tissue, and amiloride and analogs affect the nasal epithelia (CF or non-CF) in a similar manner.
We further compared phenamil and benzamil to amiloride with respect to reversal of block and absorption. Both benzamil and phenamil exhibited less reversal of block than amiloride that, in part, may reflect the stronger interactions of these compounds with the targeted protein. In contrast, both were more rapidly absorbed than amiloride, with the rank order of phenamil > benzamil > amiloride for HBE cells. The high rate of benzamil absorption compared with a paracellular path tracer, mannitol, suggested a transcellular route for benzamil absorption.
We utilized the high degree of fluorescence of benzamil to further characterize the absorption of benzamil by HBE cells using confocal microscopy. As depicted in the x-z scans (Fig. 6), benzamil was rapidly accumulated in the cytosol, suggesting possible carrier-mediated and diffusional components. An organic cation transport protein has been proposed to mediate amiloride transport across renal brush-border membrane (Wright and Wunz, 1989). Furthermore, studies have shown that organic cation transporters are expressed in respiratory tissues (Tamai et al., 1998; Wu et al., 1998). Thus, it is likely that all three compounds are transported by organic cation transporters to some degree, and the enhanced absorption of benzamil and phenamil in part reflects increased transepithelial diffusion due to their greater lipophilicity.
Based on its greater potency, slower absorption, and uncertainty of phenamil regarding specificity, we selected benzamil over phenamil for comparison with amiloride in vivo in sheep TMV and MC assays. We administered equimolar amounts of amiloride or benzamil via aerosol to the sheep lung with a clinical jet nebulizer. Amiloride significantly raised TMV rates (Fig. 7A). Mucus clearance, as measured as the clearance of radiotracer from the distal to proximal airways of sheep (Fig. 8), was also significantly enhanced by aerosolized amiloride similar to effects reported in healthy human and in some CF subjects (Kohler et al., 1986; Knowles et al., 1990; Sood et al., 2003). Benzamil also produced an increase in TMV and an increase in MC as compared with vehicle but in both assays did not exceed the effects of amiloride (Figs. 7 and 8). One experimental possibility for not observing differences in TMV and MC in response to amiloride versus benzamil is a limited dynamic range in the two in vivo assays. Arguing against this possibility are reports of a greater TMV with chloride secretogogues (Yerxa et at., 2002). Thus, we conclude that amiloride and benzamil are equieffective in vivo, with the greater intrinsic potency of benzamil compared with amiloride being offset by its more rapid absorption from sheep airway surfaces.
We compared the relevant parameters of drug action in OBE and HBE cells in vitro to describe species variation that may allow us to extrapolate the sheep MC and TMV data to human MC. The observation that the ranking of the sodium channel blockers for each parameter in each species was similar makes the in vivo ovine TMV and MC measurements valid for comparing relative initial activity and durability of different sodium channel blockers. The reduced potency and increased absorption in OBE as compared with HBE cells would predict that sheep data underestimate the magnitude and duration of the effect of equimolar doses of specific compounds in humans. The data from the sheep studies that benzamil was equieffective with amiloride in TMV or MC differ from two reports of human studies using a superfusion technique on human nasal epithelium (Hofmann et al., 1998; Rodgers and Knox, 1999). In these studies, superfusion or aerosol delivery of very high concentrations of benzamil (1.7–7 mM) or amiloride (1–10 mM) suggested that benzamil had a prolonged effect on inhibiting the nasal transepithelial potential difference correlate of Na+ absorption compared with amiloride in the nasal cavity. One difference between our findings in the sheep and the human nasal studies is that both nasal delivery techniques administered relatively (compared with aerosolization in sheep) large volumes and, hence, greater mass of drug to the nasal surface. Accordingly, we speculate that the relative greater mass of drug delivered to the nasal surface was accumulated within the nasal epithelium (refer to Fig. 6) and recycled to the surface (unpublished observations), which achieve a more prolonged block. It is unlikely a similar mass of drug could be delivered to the pulmonary surfaces without promoting renal potassium retention.
In summary, our data suggest that blocking airway ENaC using aerosol sodium channel blocker therapy increases MC and TMV in sheep. Benzamil was found to be more potent than phenamil and amiloride in blocking transepithelial sodium absorption, absorbed to a greater extent than amiloride but to a lesser degree than phenamil from airway surfaces, and was no more effective than amiloride on enhancing TMV and MC when aerosolized in sheep. Thus, we predict that second generation amiloride analogs will not be therapeutically more active than amiloride. However, from this study, we can formulate an algorithm to identify airway epithelial selective sodium channel blockers that would outperform amiloride in accelerating MC. The novel compound would have to be at least as, or more potent than, benzamil, have a similar or slower recovery rate than benzamil, and exhibit a decreased rate of transepithelial absorption to the extent that supratherapeutic concentrations of the analog would be maintained in the ASL greater than what was seen for amiloride. Additional features that would also increase safety (diminish renal side effects) would be to have a compound that is susceptible to epithelial, plasma, or liver biotransformation either be converted to a less potent or inactive analog or excreted, unlike amiloride, nonrenally.
Acknowledgments
We thank Troy Lee from the University of Miami, Dr. M. J. Cho from the University of North Carolina-Chapel Hill, and the University of North Carolina Tissue Core (Chapel Hill, NC) for technical contributions.
Footnotes
-
A.J.H. was a recipient of a Canadian Institute of Health and Research fellowship during the period of this study. This study was supported in part by a Pilot and Feasibility Grant from the Cystic Fibrosis Foundation and the Canadian Institute of Health and Research (to A.J.H.) and by Grant 34322 from the National Institutes of Health (National Heart, Lung, and Blood Institute) (to R.C.B.). A portion of this work was presented in abstract form: Hirsh AJ and Boucher RC (2000) Absorption of Na+ channel inhibitors by cystic fibrosis airway epithelium. Pediatr Pulmonol (Suppl 20):267.
-
doi:10.1124/jpet.104.071886.
-
ABBREVIATIONS: MC, mucus clearance; ASL, airway surface liquid; CF, cystic fibrosis; ENaC, epithelial sodium channel(s); HBE, human bronchial epithelial; OBE, ovine bronchial epithelial; TMV, tracheal mucous velocity; ALI, air-liquid interface; Rt, transepithelial resistance; KRB, Krebs-Ringer bicarbonate; Isc, short-circuit current; Pcoeff, permeability coefficient(s); ETT, endotracheal tube; ANOVA, analysis of variance.
- Received May 28, 2004.
- Accepted July 22, 2004.
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}