Article Text

Abstract
Objective The purpose of our study was to evaluate the association between short and long sleep duration and all-cause and cardiovascular mortality among elderly individuals.
Design Systematic review and meta-analysis of population-based cohort studies.
Setting Articles were retrieved from international and national electronic databases.
Study selection Studies were identified in PubMed, EMBASE, LILACS (Latin American and Caribbean Health Sciences Literature), IBECS (Bibliographic Index on Health Sciences from Spain) and CAPES (PhD thesis repository) between 1980 and 2015. Studies which met all criteria were eligible: participants aged 60 years or over, assessment of sleep duration as 24 h, nighttime or daytime sleep, evaluation of all-cause or cause-specific mortality, population-based cohort studies conducted on representative samples. There was no language restriction and studies published as abstracts were excluded.
Data extraction Data were analysed using the Comprehensive Meta-Analysis software (V.3.3.070), and summary estimates (relative risk (RR), 95% CI) were calculated using a random effects model. Heterogeneity and consistency were evaluated through Cochran's Q and the I2 statistics, respectively, and sensitivity analyses were conducted.
Primary and secondary outcome measures All-cause and cardiovascular mortality.
Results Overall, 27 cohort studies were selected, comprising >70 000 elderly individuals, and followed up from 3.4 to 35 years. In the pooled analysis, long and short sleep duration were associated with increased all-cause mortality (RR 1.33; 95% CI 1.24 to 1.43 and RR 1.07; 95% CI 1.03 to 1.11, respectively), compared with the reference category. For cardiovascular mortality, the pooled relative risks were 1.43 (95% CI 1.15 to 1.78) for long sleep, and 1.18 (95% CI 0.76 to 1.84) for short sleep. Daytime napping ≥30 min was associated with risk of all-cause mortality (RR 1.27; 95% CI 1.08 to 1.49), compared with no daytime sleep, but longer sleep duration (≥2.0 h) was not (RR 1.34; 95% CI 1.95 to 1.90).
Conclusions Among elderly individuals, long and short sleep duration are associated with increased risk for all-cause mortality. Long sleep duration is associated with cardiovascular mortality.
- SLEEP MEDICINE
- GERIATRIC MEDICINE
- EPIDEMIOLOGY
- Meta-analysis
- Systematic review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Long and short sleep duration are associated with increased risk for all-cause mortality, but only long sleep duration is significantly associated with cardiovascular mortality.
The definition of sleep duration varied among studies.
There is scarce evidence about mechanisms to explain the association.
Sleep fragmentation is hardly accessed and is not available in most of the studies.
Meta-analysis of observational data cannot fully control for confounding factors.
Introduction
The association between sleep duration and a range of health outcomes has received growing attention. Laboratory and epidemiological-based evidence demonstrate that self-reported short and long sleep duration (often defined as <6 or 7 and >8 or 9 h, respectively) are associated with cardiovascular disease (CVD),1–6 diabetes mellitus,7–10 obesity11–15 and poor self-rated health.16 In addition, large cohort studies5 ,17–19 and systematic reviews2 ,20 ,21 have shown that sleep duration is associated with increased risk of mortality among middle-aged adults.
Health-related sleeping problems are particularly relevant for individuals aged 60 years or older, a group which is expected to reach two billion in 2050.22 Sleep problems are prevalent in the elderly population and approximately 50% have sleep-related symptoms.23 The association between sleep duration and mortality has scarcely been investigated in this population, with reports that have been inconsistent and based on limited sample sizes.21 ,24 ,25
The lack of statistical power is overcome by carrying out meta-analyses, which allows that results from different studies can be combined, increasing the statistical power and precision of estimates.8 In this systematic review with meta-analysis, we aimed to summarise the evidence from population-based cohort studies that addresses the association between short or long sleep duration and mortality in elderly individuals.
Methods
This study was carried out in accordance with the recommendations of the Transparent Reporting of Systematic Reviews and Meta-Analyses (PRISMA) guideline.26
Literature search
Retrieval of articles was based on Medical Subject Headings (MeSH) and Health Sciences Descriptors (DeCS) descriptors, which were combined using Boolean operators (table 1). We searched the electronic databases PubMed, EMBASE, LILACS (Latin American and Caribbean Health Sciences Literature) and IBECS (Bibliographic Index on Health Sciences from Spain). We also searched reference lists of original and review articles. No language restrictions were applied.
Search strategy used to locate articles in the database of MEDLINE/PubMed*
Inclusion and exclusion criteria
Eligible studies were selected among those published between 1980 and 2015, which met all of the following criteria: (1) participants aged 60 years or over; (2) assessment of sleep duration as 24 h, nighttime or daytime sleep; (3) evaluation of all-cause or cause-specific mortality and (4) population-based cohort studies conducted on representative samples. Studies published as abstracts were excluded, as well as thesis or dissertations that were also published as articles. If multiple published reports from the same study were available, we included the one with the most detailed information for exposure and outcome. The systematic review did not require ethical approval.
Study selection and data extraction
Study selection was conducted in two stages: an initial screening of titles and abstracts to identify potentially relevant papers, followed by screening of the full-length papers. Two independent reviewers (AAdS and CWS) assessed eligibility using a standardised protocol (available under request). The assessors appraised all studies for internal validity, using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, and a qualitative assessment of its items was held: ascertainment of population, exposure, comparison group, outcome of interest that was not present at the start of the study (which is obvious since the outcome is death), comparability of cohorts on the basis of the design or analysis, assessment of outcome by independent blind assessment (for CVD deaths), follow-up long enough for outcomes to occur, and adequacy of follow-up of the cohort studies. We found that all studies provided enough information to ensure the quality of reporting.
Data were extracted using a pretested spreadsheet. Agreement beyond chance among reviewers (interassessor reliability) was assessed by the κ statistic at the pilot phase, and subsequent disagreements were resolved by consensus with an independent reviewer (RGBdM). The extraction of data included information to identify the authors, population (place, time and demographic characteristics), study design, year of publication, baseline and follow-up periods, number and cause of deaths, types of sleep (24 h sleep, nighttime sleep or daytime sleep), measurement of sleep duration, categories of ‘short’ and ‘long’ sleep duration, reference category used in the analysis, outcomes assessment, point estimate used in the studies—relative risk (RR) or HR—and 95% CI, and covariates used in the multivariate analysis.
Statistical analysis
Studies were assessed for selection, information, measurement and confounding biases, based on the STROBE guideline.27 Summary estimates (RR, 95% CI) were calculated using the random effects model for short and long sleep categories. The RR and 95% CI were extracted for all-cause and cardiovascular mortality, and adjusted estimates were presented in preference to crude estimates. Results, reported separately for men and women or age groups, were entered into the analysis as different cohorts. For articles reporting multiple categories of short and long sleep duration (eg, <6.0 and 6.0–6.9 for short sleep; 8.0–9.9 and ≥10 h for long sleep), the shortest and the longest categories (eg, <6.0 and ≥10.0 h for short and long sleep, respectively) were used. Heterogeneity and inconsistency index were evaluated through Cochran's Q test and the I2 statistics, respectively, using the Comprehensive Meta-Analysis software (V.3.3.070).
Subgroup analysis was performed to assess sources of heterogeneity and to check for the potential impact of the following factors on the association between sleep duration and mortality: sleep duration assessment (24 h or nighttime sleep), gender, geographic location, duration of follow-up, reference category and definition of sleep duration. Further, since there are several potential confounders and multivariate analyses were performed in individual studies, subgroup analyses were also conducted according to the adjusted variables. The influence of individual studies on the magnitude of the pooled estimate was examined by omitting one study at a time and examining the extent to which inferences were dependent on a particular study (sensitivity analysis).
Funnel plots were used to detect publication bias, and Egger’s regression test was applied to measure the funnel plot asymmetry. Combined risks were recalculated after estimating from the asymmetry of the funnel plot the number of ‘missing’ studies and their effect sizes and SEs—a method known as ‘trim and fill’.28
Results
Overall, 27 cohort studies were selected (figure 1), comprising >77 000 elderly individuals. Authors of studies, which also included participants younger than 60 years, whose corresponding author was available, were contacted to request a reanalysis of data, restricted to elderly individuals. Five authors29–33 did a reanalysis and sent additional data. Those studies were included in the meta-analysis.

Flow chart of records retrieved, screened and included in the systematic review.
Table 2 summarises characteristics of the studies from 13 different countries, including two studies that recruited only women,33 ,34 and one with men only.35 Six authors reported outcomes separately for men and women.30 ,32 ,36–39 The number of participants in the studies varied from 16740 to 11 39541 and the follow-up period ranged from 3.435 to 3529 years.
Description of the studies included in the meta-analysis (in order of baseline year)
Table 3 summarises additional characteristics, including definitions of ‘short’ and ‘long’ sleep duration, which were adopted in the studies, and describes the methods used in each study. All-cause mortality was reported in 27 studies24 ,29–54 and cardiovascular mortality in 9 studies.29 ,31 ,34 ,36 ,37 ,40 ,41 ,52 ,53 Nighttime sleep duration was reported in 16 studies,24 ,29 ,30 ,33 ,34 ,37–40 ,42–46 ,48 ,53 and 24 h sleep in 11 studies,31 ,32 ,34 ,35 ,40 ,41 ,47 ,49 ,50 ,52 ,54 while daytime sleep was evaluated in 4 studies.36 ,37 ,45 ,51 Sleep duration was assessed by self-report using a single survey question in almost all studies, and cause of death was based on death certificates, although a few studies used additional sources of information.24 ,29 ,32 ,33 ,35 ,38 ,40 ,44 ,46 ,52 One included study assessed sleep duration objectively by actigraphy.35 Kripke et al33 and Zuurbier et al32 assessed sleep duration using a questionnaire in addition to actigraphic studies.
Characteristics of the studies included in the meta-analysis (in order of baseline year)
Eighteen of the 27 studies adjusted for or stratified for age and sex in the analyses.30–32 ,36–40 ,41 ,43 ,45 ,47–50 ,52–54 Seventeen studies adjusted for demographic and lifestyle characteristics plus comorbid conditions,24 ,30–32 ,34 ,35 ,37–39 ,41 ,45 ,48 ,49 ,51–54 and 10 included sleep-related medications as confounders.24 ,30 ,32 ,34 ,35 ,38 ,46 ,51 ,53 ,54 Only two studies adjusted for functional status (activities of daily living)48 ,54 and frailty.35 ,38
Long sleep duration and mortality
Figure 2 shows that long sleep duration was associated with a greater risk of death (RR 1.33; 95% CI 1.24 to 1.43), with moderate heterogeneity among studies (I2=61.9%, Q=73.55, p<0.001; random model). Despite the evidence of publication bias, the adjusted effect provided by the trim and fill method remained statistically significant (RR 1.27; 95% CI 1.18 to 1.36). Sensitivity analysis, by omitting one study at a time, showed similar results with no statistically significant differences. However, the removal of the study performed by Mallon et al30 reduced the risk of long sleep duration on mortality to RR 1.22 (95% CI 1.18 to 1.26).

Forest plot of mortality risk associated with long sleep duration compared with reference group. DNA, data not available.
The association between long duration of sleep and cardiovascular mortality was also statistically significant (RR 1.43; 95% CI 1.15 to 1.78). Daytime napping ≥30 min was associated with risk of all-cause mortality (RR 1.27; 95% CI 1.08 to 1.49), compared with no daytime sleep. However, in separate analysis, longer sleep duration (≥2.0 h) was not significantly associated with risk of death (RR 1.34; 95% CI 1.95 to 1.90).
Short sleep duration and mortality
Figure 3 shows the association between short sleep and all-cause mortality. Pooled analysis showed that short sleep duration was significantly associated with risk of death (RR 1.07; 95% CI 1.03 to 1.11). There was no evidence of publication bias (p=0.45) or heterogeneity among studies (I2=4.7%, Q=27.28, p=0.39; fixed model). The trim and fill method detected three missing studies, but the revised estimate remained the same. Sensitivity analysis, by omitting one study at a time, showed similar results with no statistically significant differences. Pooled analysis remained statistically significant after excluding Kronholm et al's29 study, which had the largest influence (relative weight: 31.6%) in the overall pooled estimate, as well as with the exclusion of Mallon et al's30 study. The association between short duration of sleep and cardiovascular mortality was not statistically significant (RR 1.18; 95% CI 0.76 to 1.84).

Forest plot of mortality risk associated with short sleep duration compared with reference group. DNA, data not available.
Sources of heterogeneity
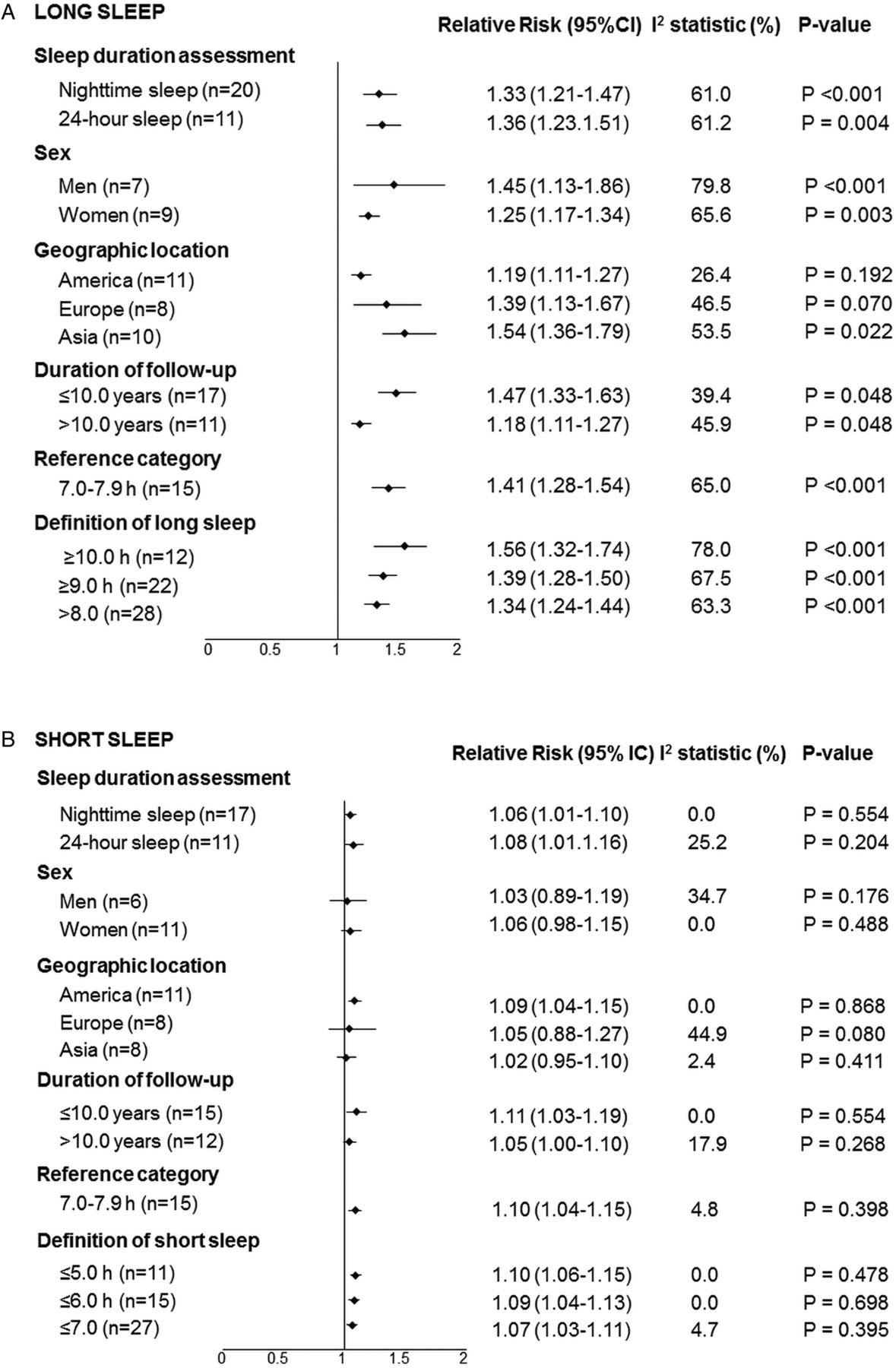
The risk due to the long duration of sleep was detected for nighttime sleep and 24 h, between men and women in cohorts conducted in America, Europe and Asia, and for different definitions of long sleep (figure 4A). It progressively increased as the definition of long sleep changed from >8.0 to ≥10.0 h. The association tended to be weaker in studies carried out in American countries compared with Asian population studies. There was a stronger effect for studies with a length of follow-up ≤10 years in analysis of long sleep. In subgroup analysis of short sleep duration, the effect did not differ among sleep evaluation methods or according to the definition of short sleep (figure 4B). The association between short sleep and mortality from all causes was significant only in studies conducted in North America. We were unable to perform the analysis by age subgroups, once one study40 included only elderly aged [more than equal to symbol] 80 years and other studies did not provide analysis by age groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup analyses to explore sources of heterogeneity in (A) long and (B) short sleep duration.
Table 4 shows estimates, obtained from random effects models, for sleep duration and all-cause mortality according to the variables included in the multivariate analysis. The inclusion of covariates resulted in the attenuation of the association between long sleep duration and mortality, with moderate heterogeneity among studies.
Analysis of subgroups for the association between sleep duration and all-cause mortality according to the models of multivariate analysis carried out for control of confounding factors in the individual studies
Risk of bias
In most of the included studies, sleep duration was self-reported and this method does not differentiate time asleep from time in bed. Although we have included risk assessments carried out in multivariate analyses, three studies did not provide adjusted analyses,29 ,33 ,44 one study adjusted only for age,36 and for other studies, this was done for a few confounders.42 ,46 ,47 In an attempt to control for confounding, additional analyses were carried out including studies which had similar adjustment for confounding factors. Nevertheless, adjustments for health conditions resulted in attenuation of the association between long sleep and mortality. Another limitation of the primary studies is the lack of assessment of sleep quality, which can interfere with sleep duration.
Discussion
To the best of our knowledge, this is the first systematic review with meta-analysis that investigated the relationship of sleep duration with mortality in the elderly population. Pooled analyses of data from 29 cohort studies indicate that sleep duration exceeding 8, 9 or 10 h, compared with an average sleep duration of 7–8 h, was associated with an approximately 33% increased risk of all-cause mortality. Additionally, data from eight cohorts provided an estimated 43% increased risk for cardiovascular mortality in the long sleep duration group. Similar analysis for short sleep duration (<7 h) extracted from 27 cohort studies also showed a statistically significant association with all-cause mortality, with a 6% higher risk. Statistically significant association with mortality was not observed for long daytime sleep (>2 h).
There is a particular need to analyse the association between sleep duration and health outcomes in the elderly population. Sleep physiology undergoes significant changes across the lifespan and the distributions of sleep duration vary with age.55 ,56 Sleep disorders, including sleep apnoea, insomnia and periodic limb movement disorders, are prevalent in older individuals; each may impact sleep quality and duration.57 ,58 Numerous health problems prevalent in the elderly may also influence sleep duration or may influence physiological responses to altered sleep.55 For these reasons, the relationship between sleep duration and mortality may differ for older compared with middle-aged and younger adults.
Studies conducted in young individuals have identified a U-shaped relationship between sleep duration and all-cause mortality.20 ,21 The association was weaker for short in comparison to long sleep duration. A meta-analysis conducted among adults and the elderly population showed an increased risk of dying for both short and long sleep duration. For short sleep duration, the magnitude of the effect was greater than the observed risk in this meta-analysis, but for long sleep duration the risk was similar.21 Our findings are in accordance with such studies, including similar estimates regarding the association of long sleep duration and cardiovascular mortality in the adult population.21 It has been postulated that the adverse health outcomes associated with prolonged sleep might be a consequence of underlying diseases, frailty and worse health status, or be a part of the dying process.19 ,59 ,60 In addition, an increase in sleep duration that occurs during the last few weeks or months of life61 might be a consequence of the disease and not its cause.
Castro-Costa et al24 addressed reverse causality by repeating their analyses after excluding mortality data in the 2 years following the baseline assessment and observed similar results. Moreover, Mesas et al54 found that long sleep duration was associated with greater mortality, even in those with better health status and with no cognitive impairment, depression or functional limitations. These findings suggest that mortality associated with long sleep duration is not entirely due to a worse health status, and that long sleep duration itself may be an independent predictor. Several mechanisms have been suggested to explain the association between long sleep and mortality, including sleep fragmentation and sympathetic nervous system activation,25 ,62 ,63 changes in cytokine levels,64 ,65 and physiological reduction of the photoperiod (ratio of daylight to darkness),66 ,67 among others.68–70 However, there is scarce solid evidence64 and long sleep duration could be a marker of physiological deviation from normal ageing.46 Nevertheless, if these mechanisms actually participate in the axis of causality, they may be linked and not mutually exclusive.25
In addition to residual confounding, misclassification of sleep duration should be considered as an alternative explanation. Sleep duration did not allow one to differentiate time asleep from time in bed—unless explicitly built as additional questions.46 Prolonged time in bed per se may be harmful through metabolic effects including insulin resistance and deconditioning.25 ,63 While actigraphy can provide objective measures of sleep duration,71 it also has its limitations and may systematically misclassify sleep duration in individuals with sleep apnoea, depression and neurological disorders. Moreover, sleep duration was assessed at one point in time in all studies, and a single measurement of exposure may not capture the sustained effects of sleep duration over time,8 mostly if the reported period was shortly before death.37
Although there are several cut-offs for the duration of sleep, we did not have a hypothesis a priori on a specific cut-off for short or long sleep. The decisions taken before starting the analysis were to analyse the extreme cut-offs for long and short sleep, where several cut-off points were available, keeping the reference category as presented in the individual articles. Recognising the diversity of cut-offs, subgroup analyses were performed using all available cut-off points. All cut-offs for long sleep duration were associated with mortality, but there was no association with the cut-offs for short sleep duration.
The pooled effect sizes seem small, but evaluation of health issues in the general population, compared with an individual study cohort, requires a different interpretation—even small shifts are of significant population value.72 Data were analysed using the random effects model, resulting in more conservative summary estimates, in comparison to the fixed effect model. However, these analyses are likely to be fully generalised.73 Furthermore, the direction of the associations is consistent in different populations, allowing one to assume that they are not dependent of lifestyles and hours of exposure to the sun, which influence sleep duration.8 ,74 Although meta-analysis detected significant heterogeneity among studies, further sensitivity analysis was in favour of consistent effects across populations.
Study limitations
There are limitations with using these findings to infer that long sleep duration is detrimental to the health of elderly individuals. The quality of the data cannot go beyond the quality of the individual studies included.75 A meta-analysis of observational data, though prospective, cannot fully control for confounding factors.8 Geriatric syndromes, including functional disability, immobility, frailty, cognitive impairment—especially dementia and depression—and use of sleep, antidepressant or antipsychotic medications predict mortality in older persons46 ,76 ,77 and could also be associated with long sleep duration.64 ,78 ,79 In most of the studies, these covariates were not included as potential confounding factors. Sleep quality remains a hypothesis to be addressed in future research.
The evidence of publication bias in the long sleep meta-analysis means that the results can only be representative of the studies that have been included and are unable to provide a representative inference of all studies published, but not included.8 Given the updated extensive search of articles, the use of conservative random effect models, and the results of subgroup and sensitivity analyses, it is unlikely that any addition to the reviewed studies would have generated summary estimates outside the reported 95% CIs, which are supported by the results of the trim and fill method.
Finally, studies included in this review used different categorical cut-off points in the analyses, some of them considering nighttime sleep and others 24 h sleep (including daytime sleep), hence precluding our ability to examine the associations between sleep duration and mortality at individual hour or smaller sleep duration categories. In this meta-analysis, long sleep duration did not include napping, but daytime included. In two meta-analysis published recently, statistically significant associations were found with all-cause mortality, but in a limited number of studies.80 ,81 While the inconsistency reduces the generalisability of the conclusions, the convergence of findings strengthens the reliability of the association between long sleep duration and mortality. We attempted to combine categories into overall short and long sleep categories and, in subgroup analysis, we performed separate analysis according to the cut-point used and sleep duration assessment (24 h sleep or nighttime).
Conclusions
This meta-analysis indicated that both long and short sleep duration are significantly associated with all-cause mortality in elderly individuals. Additionally, long sleep duration was also significantly associated with an increased risk for cardiovascular mortality. These findings suggest that sleep duration can be regarded as an additional behavioural risk factor or an adverse prognosis marker. The results must be considered in the context of the inherent limitations of observational studies, related to misclassification of sleep duration and potential residual confounding, especially due to geriatric syndromes. Future studies should be designed to address if modifying sleep duration could produce changes in health outcomes and mortality.
References
Footnotes
Contributors AAdS, FDF and SCF conceived the study aims and design. AAdS, CWS and RGBdM contributed to the systematic review and data extraction, performed the analysis, interpreted the results, and drafted the manuscript. RGBdM, SCF and FDF contributed to the revision of the data extraction, interpretation of results, and to the review of the manuscript. FDF and SR were important contributors to the interpretation and presentation of the manuscript. All the authors reviewed and approved the final version of the manuscript. SCF is the guarantor.
Funding This study was partially supported by the National Council for Scientific and Technological Development (CNPq), Brazil and Postgraduate Studies Program in Epidemiology, School of Medicine, Universidade Federal do Rio Grande do Sul (UFRGS). SCF and FDF have research scholarships from the CNPq, Brazil.
Disclaimer CNPq and HCPA did not take part in the study design, analysis, results interpretation or drafting of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.