Article Text

Abstract
Rationale Proline–glycine–proline (PGP), a neutrophil chemoattractant derived from the enzymatic breakdown of collagen, is elevated in sputum of patients with chronic obstructive pulmonary disease (COPD) and may contribute to disease progression. Whether sputum levels of PGP respond to therapy for COPD or predict outcomes is unknown.
Objectives We conducted a study ancillary to a multicenter trial of the efficacy of azithromycin treatment for 1 year in preventing COPD exacerbations to test whether sputum levels of PGP were altered by treatment or associated with exacerbation frequency.
Methods We collected remnant sputa from trial participants and assayed them in a blinded fashion for PGP, myeloperoxidase and matrix metalloproteinase (MMP)-9 and for the ability to generate PGP from collagen ex vivo. Once the parent trial was unblinded, the results were correlated with use of azithromycin or placebo and exacerbations in participants.
Results Azithromycin treatment significantly reduced sputum levels of PGP and myeloperoxidase in patients with COPD, particularly with increased duration of therapy. We found no difference in sputum MMP-9 or PGP generation between participants taking azithromycin or placebo. Sputum PGP levels were highest around the time of an exacerbation and declined with successful treatment.
Conclusions These data support a role for PGP in the airway and parenchymal neutrophilic inflammation that drives COPD progression and exacerbations, and provide new information on the anti-inflammatory properties of macrolides. PGP may have potential as a target for novel anti-inflammatory therapies in COPD and as a biomarker for clinical trials.
- PGP
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This research was conducted ancillary to a multicenter, prospective, parallel group, placebo-controlled, double-blind study of the efficacy of azithromycin in the chronic, outpatient management of chronic obstructive pulmonary disease (COPD).
-
We demonstrate that chronic treatment with azithromycin reduces levels of proline–glycine–proline (PGP), a collagen-derived neutrophil chemoattractant, in sputum of patients with COPD.
-
This provides new information on the anti-inflammatory properties of macrolide antibiotics and supports a role for PGP in COPD pathogenesis and as a biomarker in clinical trials.
-
The number of participants included in this study is small as sputum samples were available only from a minority of participants in the parent trial.
Introduction
Proline–glycine–proline (PGP) is a tripeptide generated from the breakdown of extracellular matrix collagen and is specifically chemotactic for neutrophils in vitro and in vivo.1 PGP exerts its chemotactic effect through sequence homology with a key motif found in ELR+ CXC chemokines and binds to their receptors, CXCR1 and CXCR2.1 PGP is generated from native collagen by the action of neutrophil-derived matrix metalloproteinases (MMPs) 8 and 9, which cleave collagen into oligopeptides, followed by a secondary cleavage by prolyl endopeptidase,2 a neuronal enzyme implicated in hypertension and neuropeptide processing. Prolyl endopeptidase is also present in neutrophils where it likely participates in the generation of PGP.3 PGP is broken down in the lung by the aminopeptidase activity of leukotriene A4 hydrolase (LTA4H), an enzyme hitherto recognised only as proinflammatory through generation of leukotriene B4.4 Consequently, acute PGP-driven neutrophilic inflammation may be terminated by LTA4H. Cigarette smoke can selectively inactivate the aminopeptidase, but not the hydrolase, activity of LTA4H, thus allowing accumulation of PGP, while promoting neutrophilic inflammation.4
We have previously demonstrated that PGP is a potential sputum and serum biomarker in chronic obstructive pulmonary disease (COPD), cystic fibrosis (CF) and chronic lung transplant rejection and contributes to neutrophilic airway inflammation in these diseases.2 ,5 ,6 Sputa from patients with CF and COPD generate PGP from collagen ex vivo.2 ,5 Levels of PGP in CF sputum are higher during exacerbations and decline with successful treatment and resolution.2 Whether PGP levels are modifiable by outpatient therapy of lung diseases or whether such changes can positively impact clinical outcomes has not been tested. This is important, as no biomarker has yet been identified that can reliably aid in diagnosis and phenotyping of COPD or serve as a surrogate endpoint for clinical trials. Identifying such biomarkers is a key priority.7 ,8
Existing pharmacotherapies do not alter the neutrophilic airway and parenchymal inflammation that are at the heart of disease progression in COPD and consequently do not prevent loss of lung function. Accordingly, there is a need for new therapies. One candidate is azithromycin, a macrolide antibiotic with anti-inflammatory properties. Azithromycin and other macrolides have been proven beneficial in chronic, neutrophilic airway diseases, such as bronchiectasis, diffuse panbronchiolitis and CF.9 ,10 These effects are believed to be due, in part, to an as yet unexplained anti-inflammatory activity and not just suppression of bacterial growth.11
The National Heart Lung and Blood Institute (NHLBI) recently sponsored a multicenter trial of azithromycin in stable outpatients with COPD (the Macrolide trial).12 As macrolides have been demonstrated to reduce MMP activity in lung diseases, including COPD,11 ,13 ,14 we hypothesised that beneficial effects of azithromycin might be mediated through reducing PGP. Accordingly, we conducted a study ancillary to the Macrolide trial in which sputum collected from participants for microbial analysis was analysed for PGP and the ability to generate PGP from collagen. Once the code for the parent trial was broken, we correlated PGP levels with use of azithromycin or placebo and clinical response. The results are herein reported.
Methods
Patient recruitment
This research was carried out as an ancillary study to the Macrolide trial of the NHLBI COPD Clinical Research Network (CRN). This was a prospective, parallel group, placebo-controlled, double-blind study of the efficacy of azithromycin in the chronic, outpatient management of COPD with a primary outcome of time to first exacerbation.12 Patients with COPD, selected to be at high risk of acute exacerbation, were randomised to receive either azithromycin 250 mg daily or placebo for 12 months. Nasopharyngeal swabs were obtained from participants at various points during the trial (at randomisation, after 1, 3, 6, 9 and 12 months of treatment and 1 month after completion) to screen for colonisation by macrolide-resistant pathogens. In a limited number of participants, sputum samples were also obtained for microbial analysis. For the current study, we obtained remnant sputum from these participants for measurement of biomarkers.
Measurement of PGP, myeloperoxidase and MMP-9 in sputum
Sputum was diluted 1:1 with normal saline, filtered through a 10 kDa filter, washed with 40 µL of 1 N HCl and assayed for PGP by electrospray ionisation-liquid chromatography-mass spectrometry/mass spectrometry (ESI-LC-MS/MS) as previously described.2 ,5 The detection limit was 10 pg/mL.
Myeloperoxidase was measured in sputum using a commercially available activity assay (Calbiochem, San Diego, California, USA). Samples and standards were added to wells coated with a polyclonal antibody to human myeloperoxidase and incubated for 2 h. The detection reagent (tetramethylbenzidine and hydrogen peroxidase) was added, and after 1 h the absorbance was read at 450 nm. Activity was converted to ng/mL active myeloperoxidase using a standard curve.
The concentration of total and pro-MMP-9 was determined in sputum using commercially available ELISA kits (R&D Systems, Minneapolis, Minnesota, USA). Samples and standards were added to wells coated with a monoclonal antibody to MMP-9 and incubated for 2 h at room temperature. A fluorogenic substrate (Fluor-Pro-Leu-Gly-Leu-Ala-Arg-NH2) was added and the plate was incubated for 18 h at 37°C. Activity was quantified using a spectrophotometer with excitation and emission wavelengths of 320 and 450 nm, respectively, and converted to ng/mL active MMP-9 using a standard curve.
Generation of PGP ex vivo
One hundred microlitre of sputum was incubated with extensively dialysed (against dH2O with pH adjusted to 4.5 by addition of glacial acetic acid) intact type I or II collagen (10 µL, 1 mg/mL, Sigma-Aldrich, St Louis, Missouri, USA) for 24 h at 37°C and 5% CO2. The samples were filtered through a 10 kDa filter, washed with 40 µL of 1 N HCl and analysed using ESI-LC-MS/MS for levels of PGP. Amounts of PGP generated by each sample were determined by comparison with PGP generated by sputum incubated without collagen.
Data analysis
Sputum samples were identified as coming from participants taking azithromycin or placebo once the Macrolide trial was completed and unblinded. The number of exacerbations for each participant and the date of onset of symptoms for each exacerbation were recorded. Data are presented as means±SEM. Sputum biomarker levels and activities were compared between groups using Students t test. All p values <0.05 were considered significant.
Results
Azithromycin reduces sputum PGP and myeloperoxidase compared with placebo in a time-dependent fashion
We obtained a total of 46 sputum samples from patients with COPD recruited to the Macrolide trial and assayed them in a blinded fashion for levels of PGP. Unblinding of the parent trial revealed that there were 18 sputum samples from 13 placebo-treated participants and 14 sputum samples from 8 azithromycin-treated participants collected at months 1 through 12 of treatment. Clinical characteristics of our study participants were similar to those of the parent trial (age=67.6±8.4 years, 30% female, postbronchodilator FEV1=1.36±0.47 L, mean±SD).
Sputum PGP levels were significantly higher in participants taking placebo compared with those taking azithromycin during the trial (5.15±1.54 vs 2.27±0.87 ng/mL, p<0.05; figure 1). The difference in sputum PGP was greatest at months 9 and 12, indicating a cumulative effect of azithromycin treatment (figure 2). Given the limited data set, effects of azithromycin treatment on PGP levels are reported for groups. However, there was a progressive decline in sputum PGP with duration of treatment in five of six azithromycin-treated participants whose sputum was assayed at more than one time point.

Azithromycin treatment decreases proline–glycine–proline (PGP) levels in sputum of patients with chronic obstructive pulmonary disease compared with placebo. Inset: values represent the mean±SEM PGP concentrations for sputa (*p<0.05 vs placebo).
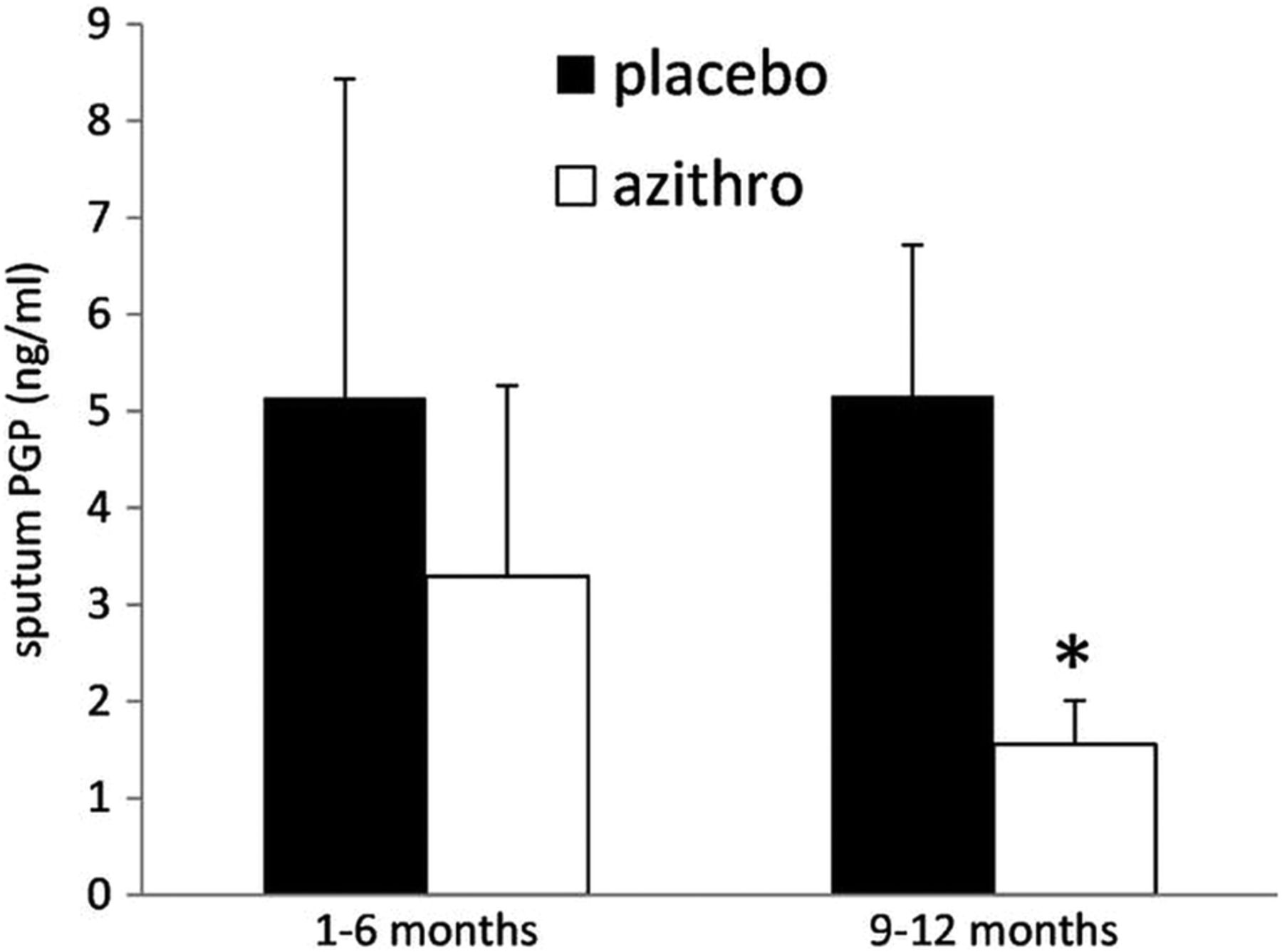
Sputum proline–glycine–proline (PGP) levels decline with increased duration of azithromycin therapy. PGP levels were significantly higher in participants treated with placebo compared with azithromycin at months 9 and 12 of therapy (*p<0.02) but not at months 1 through 6 (p=0.32).
The difference in sputum myeloperoxidase activity between participants taking placebo or azithromycin over the 12 months of the trial was not statistically significant (3391±353 vs 2884±349 ng/mL, p=0.16). However, sputum myeloperoxidase was lower in participants taking azithromycin from months 6 through 12 (3321±430 vs 2398±290 ng/mL, p<0.05), indicating a cumulative effect of azithromycin treatment on neutrophilic airway inflammation.
There was no difference between participants taking placebo or azithromycin in sputum MMP-9 activity (11.18±3.98 vs 8.39±2.42 ng/mL, NS) or PGP generation from collagen ex vivo (3.28±2.25 vs 2.94±1.73 ng/mL, NS) during the trial.
Fall in sputum PGP is associated with reduced exacerbation frequency in patients with COPD
In the Macrolide trial, treatment with azithromycin significantly reduced exacerbation frequency in high-risk patients with COPD compared with placebo (1.48 vs 1.83 exacerbations per patient year, p=0.01) and increased the time to first exacerbation.12 We saw a similar reduction in exacerbation frequency in participants taking azithromycin in our ancillary study although this was not significant due to the small size of our study group (0.91±0.37 vs 1.93±0.62 exacerbations per patient year, p=0.08).
Sputum PGP rises during COPD exacerbations and declines with resolution
We obtained the dates of exacerbations experienced by our participants during the Macrolide trial, including placebo and azithromycin-treated groups, and correlated sputum PGP with time in days from the closest exacerbation. This resulted in an interesting pattern that suggested that PGP levels precipitously rise in advance of an exacerbation and rapidly decline thereafter (figure 3). Indeed, sputum PGP was higher around the time of an exacerbation (18±4 days before or after, 12.8±4.53 ng PGP/mL; n=9) than long before (103±37 days, 1.10±0.411 ng PGP/mL, n=6; p<0.02) or after an exacerbation (141±11 days, 2.15±0.80 ng PGP/mL, n=11, p<0.02; figure 3 inset). There was a trend towards higher sputum PGP after an exacerbation than before (p=0.133).

{kind=link}
{kind=link}
{kind=link}
Sputum proline–glycine–proline (PGP) levels are highest around the time of a chronic obstructive pulmonary disease exacerbation. Values represent PGP levels at various days relative to the onset of an exacerbation (time 0). Inset: values represent the mean±SEM PGP concentrations for sputa collected 103±37 days before an exacerbation (pre), 18±4 days before or after an exacerbation (peri) or 141±11 days after an exacerbation (post). *p<0.02 (pre vs peri), #p<0.02 (post vs peri).
Discussion
PGP is a neutrophil chemoattractant in vitro and in vivo and contributes to airway inflammation in chronic lung diseases with a prominent neutrophil component including COPD and CF.2 ,5 ,6 Chronic instillation of PGP into mouse lungs results in emphysema and right ventricular hypertrophy1 and inhibition of PGP by a complementary peptide (arginine–threonine–arginine) reduces acute cigarette smoke-induced neutrophil influx into mouse lungs and prevents emphysema and right ventricular hypertrophy in a mouse model of COPD.15 ,16 However, direct evidence implicating PGP in COPD pathogenesis in humans is lacking. In the limited number of sputum samples available to us due to the design of the Macrolide trial, we demonstrate that PGP is reduced in the airways of patients with COPD taking azithromycin, particularly with longer duration of therapy and is accompanied by reduced neutrophil burden, measured as sputum myeloperoxidase. Reduction in sputum PGP is accompanied by a positive clinical response to azithromycin (reduced exacerbation frequency). Our subgroup had a similar therapeutic response to that seen in the parent trial, suggesting that our findings could be generalised to the entire Macrolide group.
Although seen with only a few specimens, sputum PGP was strikingly elevated as long as 35 days before the onset of symptoms of an acute exacerbation of COPD and briefly afterwards. It declined sharply with successful treatment and resolution (figure 3). Seemungal et al17 described a 7-days prodrome where respiratory symptoms worsened before the onset of an exacerbation but failed to predict exacerbations with spirometry. Our data suggest that airway inflammation may worsen weeks in advance of this and that PGP may predict the onset of an exacerbation long enough before symptoms appear to permit early intervention. Although many biomarkers of COPD have been described, to our knowledge, none has been shown to herald exacerbations.18 The persistence of elevated sputum PGP long after exacerbations in some individuals may contribute to continuing neutrophilic airway inflammation and promote the ‘frequent exacerbator’ phenotype.19–21
We cannot determine from our data whether the reduction in exacerbations due to azithromycin was secondary to reduced sputum PGP or whether the reduction in sputum PGP was due to fewer exacerbations in azithromycin-treated participants. Answering this question definitively would require a larger, longitudinal study of PGP in patients with COPD. Nevertheless, these data support the idea that PGP plays a significant role in COPD pathogenesis, particularly exacerbations, and may provide important clues as to the mechanism of azithromycin's anti-inflammatory properties. PGP predicted a positive response to azithromycin within 6 months of starting therapy and was superior in this respect to other biomarkers studied as part of the Macrolide trial.22
We are uncertain as to the mechanism of PGP reduction by azithromycin. Macrolide antibiotics have been reported to have numerous anti-inflammatory properties, including inhibiting MMP activity.11 ,13 ,14 As MMP-8 and MMP-9 are essential to extracellular PGP generation from collagen by neutrophils,2 this would provide an attractive potential mechanism. However, we could find no difference in sputum MMP-9 activity between treatment groups. We did not examine other MMPs which we have previously implicated in PGP generation, such as MMP-1 and MMP-8.2 ,5 We measured PGP generation ex vivo from collagen by sputum but could find no difference between treatment groups. Subsequent to the current study, we have identified a neutrophil-derived enzyme, LTA4H, which generates leukotriene B4 and rapidly degrades PGP.4 We have recently found that LTA4H is markedly elevated in COPD sputum compared to controls.23 Breakdown of PGP by LTA4H in our sputum samples could have confounded the PGP generation assay. As PGP is derived from neutrophil activity, reduced sputum PGP might reflect reduced recruitment of neutrophils to the airways due to other effects of azithromycin. The decline in sputum PGP was greater than the decline in myeloperoxidase, suggesting that PGP may have other effects in COPD aside from recruiting neutrophils. Addressing these questions was outside the scope of this study.
In conclusion, the results of our study support the idea that PGP plays an important role in COPD pathogenesis and provide clues as to the anti-inflammatory mechanism of azithromycin. PGP shows promise as a predictor of acute exacerbations and may serve as a useful biomarker for response to therapy in future studies of COPD and other chronic, neutrophilic lung diseases.
Acknowledgments
The authors would like to thank the National Heart Lung and Blood Institute chronic obstructive pulmonary disease clinical research network for their assistance in providing sputum samples and clinical data for this study.
References
Footnotes
-
Contributors PJO designed the study, acquired and interpreted the data and drafted the manuscript. PLJ and JMW acquired and interpreted the data. MTD and PDS provided sputum samples. JEB designed the study and supervised the project. All authors contributed to revision and final approval of the manuscript.
-
Funding Funding for this research came from grants HL090999, HL110950, HL077783 (to JEB) and HL092296 (to PJO) from the National Heart and Blood Institute of the National Institutes of Health.
-
Competing interests None.
-
Ethics approval Ethics approval for this study was provided by the Institutional Review Board at the University of Alabama at Birmingham. Approval for this study was also provided by the Steering Committee of the NHLBI COPD Clinical Research Network which conducted the original trial. Registration for the original trial is at clinicaltrials.gov, identifier: NCT00325897.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.