Article Text

Abstract
Objectives To summarise and synthesise published qualitative studies to characterise factors that shape patient and caregiver experiences of chronic heart failure (CHF), chronic obstructive pulmonary disease (COPD) and chronic kidney disease (CKD).
Design Meta-review of qualitative systematic reviews and metasyntheses. Papers analysed using content analysis.
Data sources CINAHL, EMBASE, MEDLINE, PsychINFO, Scopus and Web of Science were searched from January 2000 to April 2015.
Eligibility criteria for selecting studies Systematic reviews and qualitative metasyntheses where the participants were patients, caregivers and which described experiences of care for CHF, COPD and CKD in primary and secondary care who were aged ≥18 years.
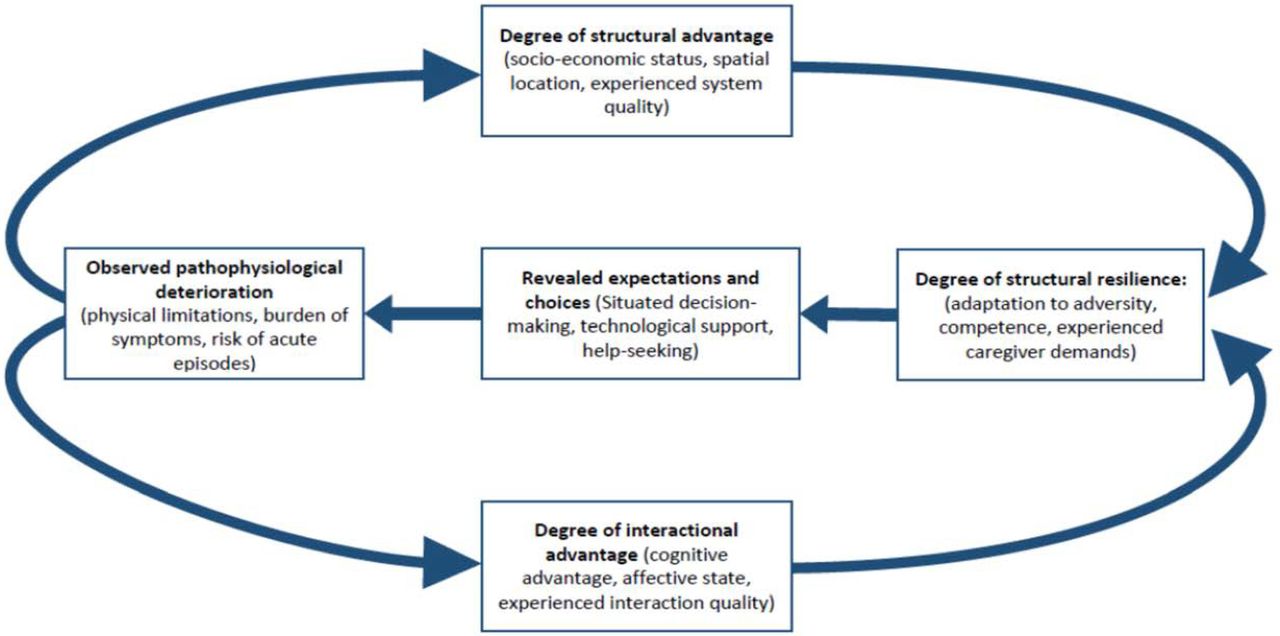
Results Searches identified 5420 articles, 53 of which met inclusion criteria. Reviews showed that patients' and caregivers' help seeking and decision-making were shaped by their degree of structural advantage (socioeconomic status, spatial location, health service quality); their degree of interactional advantage (cognitive advantage, affective state and interaction quality) and their degree of structural resilience (adaptation to adversity, competence in managing care and caregiver response to demands).
Conclusions To the best of our knowledge, this is the first synthesis of qualitative systematic reviews in the field. An important outcome of this overview is an emphasis on what patients and caregivers value and on attributes of healthcare systems, relationships and practices that affect the distressing effects and consequences of pathophysiological deterioration in CHF, COPD and CKD. Interventions that seek to empower individual patients may have limited effectiveness for those who are most affected by the combined weight of structural, relational and practical disadvantage identified in this overview. We identify potential targets for interventions that could address these disadvantages.
Systematic review registration number PROSPERO CRD42014014547.
- long-term conditions
- patient experience
- burden of treatment
- end of life
- meta-review
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first synthesis of qualitative systematic reviews focusing on patient and carer experience of life-limiting chronic conditions that consider them against pathophysiological deterioration towards the terminal phase of illness.
The review builds on systematic review and analysis to develop a robust conceptual model of the factors that shape patient and caregiver expectations and choices about help seeking and self-care, and which shows how these are the products of rational decisions and experiential processes.
The review demonstrates the value of qualitative research that identifies and characterises important aspects of patient experience and health and healthcare-related behaviours.
The review provides proposed domains of patient and caregiver experience that may represent potential targets for new interventions to support patients and caregivers to improve capacity and better manage workload to promote improved experience of illness.
This is an overview of a heterogeneous set of papers and as such there was considerable variability in research aims, methods and perspectives which is a limitation of the study.
Introduction
Globally, health services are responding to an increasingly older population characterised by complexes of multimorbidity that include long-term life-limiting conditions.1 As the burden of disease grows, so too does another kind of problem—burden of treatment2—which occurs as the work of disease management has been shifted from formal healthcare provision to self-management at home. This shift has been a major focus of policy effort in health services that deliver care for people with long-term conditions.3 ,4 However, for a significant proportion of people with chronic and often life-limiting conditions, illness trajectories are characterised by major disruptions.5 ,6 They include increasingly frequent cycles of hospital admission and discharge, supported self-management at home and readmission as exacerbation events occur.7 Here, there is a complex balancing act to be performed around the work of being a patient. This involves managing the limiting effects of symptoms while also managing complex therapeutic regimens, self-monitoring technologies and assessment regimes, and interactions with healthcare providers and organisations.8–10 These admission–discharge–readmission cycles may lead to increasing experiences of complex workload for patients and their carers which can sometimes be overwhelming and may have important effects of quality of life.2 ,11–13
Understanding the parameters of patient workload and the experiences of complexity that stem from it has recently become an important focus of research on long-term conditions,14–20 and has led to modelling work that has focused on the relationships between treatment burden, symptom burden and healthcare systems.12 ,13 ,21–23 This has taken place against the background of a programme of policy and practice development that, internationally, focuses on reworking the sick-role and rethinking the relationship between the sick person and healthcare system,24 and understanding the dynamic role of social networks in supporting them.25 Yet problems remain in the way that researchers, clinicians and policymakers understand patients with long-term conditions. In policy terms, this group is sometimes seen as the source of inappropriate and excess demand on primary care services and emergency departments.26 These factors are becoming increasingly important as healthcare systems find themselves under significant pressure to control costs and reduce spending.
Much clinical and health services research on long-term conditions focuses on controlling symptoms or delaying their onset—achieving equilibrium, even when this may be punctuated by acute exacerbation events—but in this paper, we are concerned with the experiences of people with chronic heart failure (CHF), chronic obstructive pulmonary disease (COPD) and chronic kidney disease (CKD) as they approach the terminal phase of their illness. Here, factors leading to pathophysiological deterioration limit their capacity to participate independently in self-management and healthcare processes.27 As this happens, they experience new dependencies on health services and new demands on informal networks that provide care and social support. All of these factors must be balanced against the wider demands of everyday life,23 and we need to better understand how these problems are framed and experienced by people with long-term conditions, and this review aims to ‘identify, characterise and explain the common factors that shape patient journeys through care in CHF, COPD and CKD’28 in order to inform future intervention development.
Methods and analysis
Eligibility criteria
This is a systematic review including data from qualitative reviews and the eligibility criteria for study inclusion have been developed using the PICO (participants, interventions, comparators and outcomes) framework (box 1).
PICO criteria for including studies
▸ Population: Patients (aged >18 years and diagnosed with chronic heart failure, chronic kidney disease or chronic obstructive pulmonary disease), and formal or informal caregivers and health professionals in healthcare settings (including triage services, emergency departments, in-patient hospital care, outpatient/ambulatory care departments, primary care service/family practice doctor's offices, community nursing services or at home).
▸ Intervention: Experiences of healthcare provision.
▸ Comparator: This review not limited to comparator studies. Where comparators are present these may include: usual care or control groups.
▸ Outcomes: Qualitative data on patients and caregivers experiences of care for those with chronic heart failure, chronic obstructive pulmonary disease or chronic kidney disease.
▸ Study type: Secondary studies (qualitative or mixed method systematic reviews, qualitative meta-syntheses and meta-ethnographies).
Inclusion and exclusion criteria
We included papers that met the PICO criteria (box 1) and were published in English reporting qualitative reviews of patients' or caregivers' experiences of healthcare provision. Some of these studies also included the views of health professionals. Mixed methods reviews were included if analysis of primary qualitative studies could be clearly differentiated from analysis of other kinds of primary studies in the text. Papers were excluded if they were: reports of treatment; reports of healthcare organisation or delivery which were not concerned with patients' or caregivers' experience; summaries or discussions of the literature or editorials, notes, letters and case reports.
Searches and information sources
Searches were conducted in the following bibliographic databases: MEDLINE(R) In-Process and Other Non-Indexed Citations and MEDLINE(R); Embase; CINAHL Plus; Science Citation Index Expanded; Social Sciences Citation Index; Arts and Humanities Citation Index; PsycINFO; and Scopus. Searches were completed by April 2015 and identified papers published between 1 January 2000 and 31 December 2014. Full details of the search strategy are provided in figure 1.
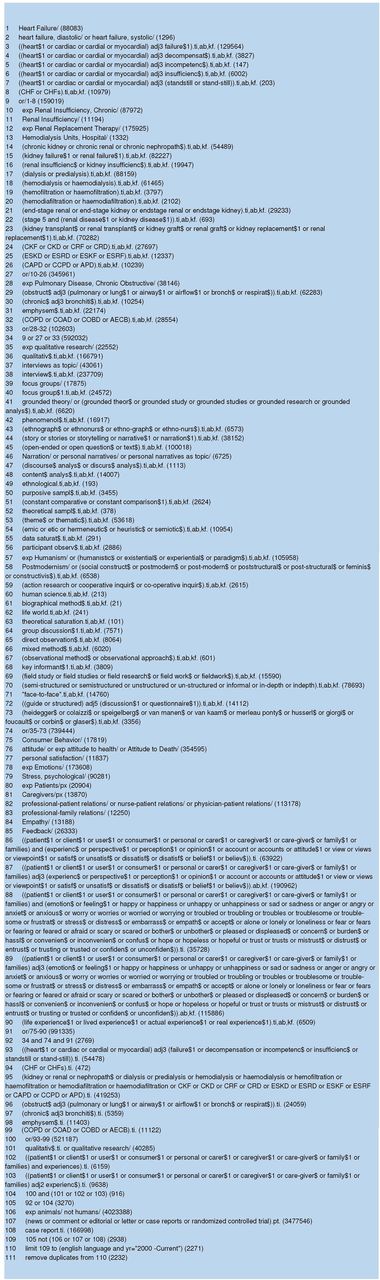
Search strategy.
Study selection and data extraction
All titles and abstracts were screened independently by AC and CRM or AC and MM. Screening of full-text articles was undertaken independently by AC and CRM with assistance from JH. Disagreements about eligibility for inclusion at title and abstract screening stage were resolved by discussion and majority vote; disagreements about inclusion at full-paper screening were resolved by discussion, or by referral (n=3) to colleagues not involved in this review.
Quality assessment
Although there are now several quality assurance frameworks for assessing primary qualitative studies,29–31 there are none that are generally accepted for meta-reviews of such studies. Quality appraisal of included papers was conducted retrospectively at the request of the journal, and was undertaken using a tool that combined elements of the AMSTAR32 and CASP33 ,34 instruments. The tool is shown in online supplementary appendix 1. Each paper was appraised independently by two researchers. Overall scores were expressed as a percentage. Papers scoring over 80% were awarded a high (H) quality rating, those between 60% and 80% a medium (M) rating and papers scoring below 60% were attributed a low (L) rating. No papers were excluded on grounds of quality, and agreement statistics were not calculated. Results of this exercise (presented in tables 1⇓–3) should be treated with considerable caution because this meta-review includes studies using integrative (mixed methods) reviews, thematic analyses and qualitative metasyntheses applied in very different ways by their authors.
Summary of overview of qualitative systematic reviews and metasyntheses of experiences of CHF
Summary of overview of qualitative systematic reviews and metasyntheses of experiences of COPD
Summary of overview of qualitative systematic reviews and metasyntheses of experiences of CKD
supplementary appendix
Data analysis and synthesis
Formal data for analysis consisted of the discussion and conclusions sections of each included paper, and a qualitative content analysis35 ,36 of attributions within these was undertaken. An attribution is a statement that characterises a state and that relies on a causal inference or explanation about the supposed antecedents of that state.37 Attributions were identified on (1) patient and caregivers' experiences of illness and journeys through care, (2) experiences of healthcare practices and (3) evaluations of illness and healthcare practices. Each identified attribution was matched to any causal inferences and explanations for it that were made by authors. Where such attributions were unexplained, and where explanations could not be directly linked to an attribution about patient or caregiver experience, they were traced back through the analysis presented in the results section of each review or metasynthesis. This tracing work was especially important where integrative reviews were concerned since these drew on quantitative and qualitative primary studies and we wished to exclude the former from our analysis. Related attributions and explanations were grouped together in sets and then simple explanatory propositions were formulated to characterise them. Formal analysis of textual data was undertaken by CRM and then reviewed in detail by other authors.
Results
Results of searches
The review process is shown in figure 2: 10 866 possible articles were identified, and after the removal of duplicates, 5420 were left. Of these, 847 were reviews or metasyntheses. Further screening identified 132 potentially eligible papers and full-paper reading led to 53 reviews that fully met the criteria for inclusion. These reviews consisted of 26 articles concerned with CHF38–63 (see table 1); 13 articles concerned with COPD64–76 (see table 2) and 14 studies of CKD77–90 (see table 3). Of these, most reviews focused on aspects of everyday experiences of long-term conditions with an emphasis on understanding patient and caregiver behaviours related to self-management regimens, and a subset of 10 papers explored elements of experiences of care towards end of life.44 ,48 ,52 ,53 ,69 ,76 ,77 ,82 ,86 ,89 These 53 reviews synthesised the results of 559 reports of primary qualitative studies.

PRISMA flow chart.
Three types of review method are represented in this sample of papers: integrative reviews that synthesised qualitative studies alongside other studies (often cross-sectional surveys, reviews of routinely collected clinical data and case notes);38 ,40 ,56 ,66 ,67 ,70 ,76 ,77 ,83 ,86 systematic reviews of qualitative studies that employed some kind of thematic analysis;39 ,41–44 ,46 ,48 ,49 ,52 ,53 ,55 ,60 ,64 ,72 ,78 ,79 ,84 ,85 ,87 ,88 ,90 and reviews that were identified by their authors as qualitative meta-syntheses or meta-ethnographies.45 ,47 ,50 ,51 ,57–59 ,61–63 ,65 ,68 ,69 ,71 ,73–75 ,80–82 ,89 In addition, one paper was explicitly characterised as a discourse analysis by its authors.54 Irrespective of the method that authors stated that they had employed, the body of reviews and metasyntheses included in this synthesis were largely descriptive in their approach to data analysis.
Social structure
Socioeconomic disadvantages that play a role in structuring the unequal distribution of health problems and inequalities in access to health services were often treated as ‘contextual’ factors,49 ,62 ,70 ,71 ,73 ,76 and reviews emphasised the importance of social inequalities, employing broad and inclusive definitions of disadvantage that include access to transport and other socioeconomic resources, and environmental factors such as poor air quality and exposure to other sources of environmental pollution. Other structural variables, such as gender and ethnicity, were not well represented at all.42 ,50 ,54 ,88 One demographic variable that was given consideration was age: many reviews explicitly dealt with CHF, COPD and, to a lesser extent, CKD as diseases of old age. The views of patients and caregivers were often that such diseases were a ‘natural’ consequence of ageing.
System behaviour
Experiences of poorly coordinated and organised care,43 ,45 ,48 ,52 poor communications between professionals40 ,45 ,47 ,48 ,52 and between patients and professionals42 ,47 were common. Even so, patients and caregivers had high expectations of clinicians, especially when they needed urgent assistance,76 even though clinicians were sometimes seen as lacking important expertise around coordinating care in multimorbidities.46 Treatment decisions were restricted not only by the quality and timing of information but also by dealing with the prospect of death.78 ,81 Conversations about treatment decisions were often focused on day-to-day problems of disease management,44 ,53 ,78 ,83 and seemed to be rarely oriented towards decisions about the future—especially about palliative and supportive care, and discontinuation of treatment (eg, implantable cardiac devices or dialysis).45 ,81–83 ,86 Reviews suggested that conversations about end-of-life issues rarely took place, either because of patients' poor understanding of their conditions or because professionals recognise high levels of prognostic uncertainty and the risk of sudden death. When patients were aware of disease progression and potential prognosis, they were able to discuss end-of-life issues openly,53 although the key decision-maker was the clinician.44 ,48 ,83 This may mean that the life-limiting nature of disease was not apparent to patients.41 ,75 When it was, some patients saw living wills, and advance care plans as useful decision-making tools,77 even though these could lead to conflict and discomfort.59 Experiences of poor communications seemed to be endemic in the patient groups included in all of the reviews included in this synthesis, and common to all healthcare systems.
Understanding disease progression and symptoms
Reviews emphasised the importance of patients' and caregivers' poor understanding of disease, disease progression and the significance of symptoms.40 ,41 ,43 ,45 ,50 ,52 ,58 ,59 ,69 ,75 ,76 ,88 Women and older people were presented as being particularly vulnerable to a lack of correct knowledge;39 ,50 ,54 and most patients were seen as ill-prepared to face their disease45 and symptoms.88 Symptom recognition was particularly challenging, in the context of comorbidity, for patients, caregivers and clinicians.43 ,45 ,57 Poor understanding of disease mechanisms and progression was characterised as a key source of distress for patients and caregivers.64 It was sometimes attributed to low levels of health literacy56 and to fragmented, limited and ineffective educational resources.57 ,83 It led to negative consequences that included failure to understand the life-limiting nature of disease; wrong beliefs about the causes of acute exacerbations of symptoms; incorrect assumptions and actions that follow from these;41 ,46 ,64 ,69 feelings of powerlessness over disease progression74 and low expectations of clinical interventions.76 These factors were seen to interfere with symptom management and help seeking,65 ,66 and adherence to self-management regimens.57 ,61 They were especially important where patients needed to understand how comorbidities ‘fitted’ with each other46 ,70 and needed to manage complex polypharmacy.64 Unpredictable disease progression made planning daily and longer term activities difficult and either meant that threat to life was not explicitly acknowledged, or that if it was, uncertainty interfered with planning for end of life and the initiation of palliative care.39 ,42 ,76 ,82
Self-management regimes
Self-management regimes include participating in pulmonary and cardiac rehabilitation programmes; adhering to instructions about exercise and diet; adhering to often complex therapeutic regimens; operating and monitoring medical devices (such as implantable cardiac devices, or home oxygen equipment) along with other technologies and assessment regimes. Self-management also includes significant administrative and organisational work, as people with long-term conditions interact with healthcare providers and organisations.8–10 Reviews suggested that the performance of self-management tasks was valued by patients, who actively invested in them and displayed considerable resilience as they did so.58 ,61 ,73 ,84 They sought to overcome the disruptive effect of illness on their lives and to assimilate self-management strategies into everyday life.63 However, negative changes in self-identity, self-esteem, social functioning, physical capacity and experiences of social loss were common.41 ,43 ,79 ,84 Fear, anxiety, isolation and discomfort were consistently characterised as consequences of disease49 ,57 ,60 ,82 that interfered with participation in self-management.77 Experienced symptoms and physical limitations led to attempts to avoid physical activities53 ,71 ,80 in case they precipitated (potentially fatal) acute episodes.42 ,47 ,57 ,71 ,74 Adherence to self-management programmes was adversely affected by disruption to everyday activities and routines,40 ,67 and by conflicts with competing self-management regimes or treatment regimens for comorbidities.43 ,45 ,46 ,55 ,58 ,87
Reviews also offered evidence of adaptive processes in the face of disease progression and the disruptions that stem from this.63 Such adaptations included the accumulation of expertise and associated self-management strategies developed over time.43 ,61 Patients sought to develop strategies that would ensure better symptom control, and that increased the duration of periods between acute episodes and reduced the impact of acute episodes.67 ,87 Poor quality self-management instruction or interactions with health professionals could have adverse effects,51 especially because patients were sensitive to evidence of clinicians' doubts about the value of different self-management strategies.67
Burdens for patients and caregivers
Inequalities of access to informal support and material assistance from family and social network members71 and health professionals,40 ,70 and problems of continuity of care,76 figured prominently across all three conditions. Experiences of symptom burdens (eg, breathlessness, fatigue and anxiety) were characterised as leading to affective responses. These included psychological responses to limitations on everyday activities and relationships that led to social isolation, loss of hope and fear of death.43 ,50 ,66 ,80 ,87 Feelings of worthlessness and burdensomeness60 ,89 were commonly experienced. Some reviews suggested that they were experienced more acutely by women.41 ,50 ,54 Against this background, social support was characterised as important,38 ,84 especially when it was connected with practical contributions to self-management that might include symptom monitoring and management, information gathering and interaction with health professionals and help seeking at moments of crisis.55 Although social support was often marked by shared experiences of solidarity and collective engagement, patients appreciated the disruptive and demanding effects of their illness on caregivers and their wider social networks.47 ,81 ,89 These included increased workload, and economic consequences—as well as stress, anxiety and isolation—as disease progressed.38 ,39 ,77 ,90
Reviews also pointed to the importance of life-sustaining interventions (eg, dialysis and implantable devices) and patient and caregiver preferences for those interventions that promoted self-efficacy and delayed disease progression.45 ,73 They provided opportunities to gain some control and establish a limited degree of normality.84 ,90 However, some patients reported heightened vulnerability, feelings of dependence and unpreparedness, along with anxiety about their capacity to perform procedures and the risks of treatment failure or complications.85 ,90 Using health technologies of different kinds brought only ‘temporary mastery’ over disease, and required continuous attention.85 This led to a constant tension between managing disease and technological supports, and the other demands of everyday life.58 ,65 ,79 Technologies could be intrusive because of the demands that they made on patient and caregiver time and effort.81 Assistive technologies could also have the paradoxical effect of leaving patients and caregivers feeling isolated from clinical help and that their homes had been ‘medicalised’.90 When technological supports were no longer effective or needed to be withdrawn for other reasons, patients and caregivers often felt abandoned.81
Hospital admissions
Patients valued self-management and care at home, but did not always have full confidence in primary or community care services. They also sometimes found self-management limiting, isolating and frightening.70 In this context, help seeking was a problem because of difficulties in recognising and interpreting symptoms.51 The security of hospital care is therefore an important element of their experience and they may therefore seek it out.67 Experience of acute and uncontrollable exacerbations is frightening and distressing, but patients and caregivers often experience service provision that categorises them as anxious when anxiety is a consequence, rather than a cause, of exacerbation episodes.64 Here, patients regarded unscheduled and emergency care as one of a number of sensible options among a range of possible destinations for help seeking.73 They therefore regard accessing such care as a rational response to acute disease episodes.73
Discussion
Overcoming individual deficits
Key features of the literature included in this study are assumptions about the presence and importance of two kinds of deficits. First, there is a patient deficit rooted in poor understanding and non-adherence to treatment regimens, and that is expressed through lack of motivation to participate. Second, there is a professional deficit rooted in poor communications and coordination and that is expressed in reluctance to engage in end-of-life planning. An important finding of our synthesis, however, is that these individual behaviours are linked to structural factors (eg, socioeconomic status, spatial location) and system qualities that are much more than mere ‘context’. They may act as causal mechanisms that have important determining effects on the experiences of patients and caregivers. Their role, however, is underinvestigated. Against the background of these effects, patients and caregivers value resilience, functional performance and social support that make practical contributions to self-management, and they develop cumulative expertise in negotiating self-management tasks and in navigating healthcare systems. They also carry significant burdens. The burden of symptoms—the inevitable consequences of pathophysiological deterioration—may include frightening and potentially lethal acute episodes of disease. The burden of treatment includes additional moral responsibilities, affective and cognitive demands, increased workload and economic consequences of participation in self-management and formal healthcare. Once again, these factors are underinvestigated but may also include mechanisms that likely shape patient and caregiver behaviours.
The effects of pathophysiological deterioration mean that patients and caregivers experience cognitive, affective and interactional disadvantages derived from prognostic uncertainty. They also experience poor communications among health professionals and uncoordinated services, and they have an increasingly limited capacity to make sense of their illness and its effects. Although self-management practices, technological investments and clinical interventions are valued, they may bring only temporary gains. Their benefits are ultimately overwhelmed by disease progression and do not change its final outcome.
Process tracing model
An important secondary aim of this synthesis was to identify potential targets for interventions. In table 4, we identify and characterise a set of constructs that form a framework for the development of coordinated interventions that could act together to relieve the weight of structural, systemic, relational and individual disadvantages that are conferred on patients and caregivers experiencing these diseases and their comorbidities. Reducing these burdens is likely to improve patient outcomes and thus reduce system costs. However, it makes no sense to isolate them from each other. The constructs that are defined in table 4 represent phenomena that already are, or are in principle, measurable. In figure 3, we offer a logic model of the processes that link them: proposing that patient expectations and choices in the face of pathophysiological deterioration are mediated by their personal attributes (eg, socioeconomic status) as well as their experiences of healthcare, and moderated by the extent of resilience that they together with their caregivers and wider social support networks possess which may be influenced by a myriad of circumstantial factors.25 We need to better understand the design and implementation of interventions that might mitigate some of the key system and behavioural factors that negatively affect patient and caregiver experiences and outcomes, and that modify the chains of causation that are implicated in them.
Factors affecting patient and caregiver experience of long-term life-limiting conditions
{kind=link}
{kind=link}
{kind=link}
Factors that shape patient and caregiver expectations and choice.
Limitations
Like all evidence syntheses, ours is subject to a number of important limitations. This is an overview of a heterogeneous set of reports. There was considerable variability in research aims, perspectives and methods. There were also very significant differences in authors' underlying assumptions about patient and professional motivation and behaviour. A limitation of syntheses of qualitative work is that these variations in assumptions and perspectives, and methodological heterogeneity, are often difficult to tease out. It is therefore not clear to what extent reviews continuously reproduce a particular set of ideas about why and how patient experiences and behaviours are a problem. Using an analytic approach that focuses on identifying, characterising and explaining sets of attributions brings these factors into the foreground and helps us to detect underlying conventional assumptions. We also identified all of the underlying qualitative studies covered by these reviews. It was clear that some reviews had interrogated very similar sets of primary research papers. This may also introduce problems of publication bias.
Results in context
To the best of our knowledge, this is the first synthesis of qualitative systematic reviews focusing on patient experience of life-limiting chronic illness. Previous primary qualitative systematic reviews about the experiences of treatment burden in those with stroke and CHF excluded carer accounts and focused on developing taxonomies of treatment burden, excluding illness burden issues and did not seek to explain factors that shape patient journeys through care.17 ,52 ,91 We have explored long-term life-limiting conditions from the perspective of pathophysiological deterioration. Its point of departure was a consideration of patients' experiences of healthcare and burden of treatment in three long-term life-limiting conditions. This was situated against a background in which good decision-making about treatment, engagement with self-management and other treatment regimens, as well as conversations about end of life, are often regarded as problems of individual motivation and adherence. Many of the reviews included in this synthesis were aimed at informing professional practice and the development of interventions to support patients and caregivers with these illnesses. However, very few made concrete proposals in this regard. An analysis of this kind may be better placed to inform such work. A key finding of this synthesis is in its emphasis on what patients and caregivers value. This is not simply a matter of preferences. It also suggests that there are attributes of healthcare systems, relationships and practices that make experiences of pathophysiological deterioration worse.
Conclusion
An important implication of this review is that patient and caregiver expectations and choices are not random or arbitrary but are the outcome of an experiential process. A paradigm shift is called for in service development and research in this area. Interventions that seek to empower individual patients may have limited effectiveness for those who are most affected by the combined weight of structural, interactional and resilience factors identified in this synthesis. There are likely causal interactions between these different factors that need to be better characterised and understood, but linking service and intervention development with robust theoretical models and rigorous practically oriented research ought to be the strategic direction for this. As a start in this direction, we have proposed domains of patient and caregiver experience that may represent good targets for new interventions that respond to the combined disadvantages that they may face.
Acknowledgments
The authors thank Dr Susi Lund for acting as impartial arbiter in cases of disagreement about inclusion in this review; Dr Michael Bracher for his help with setting up the screening databases; Margaret Bush, Trisha Durrant and Zena Galbraith for their assistance with data preparation; and Christine May for her helpful and perceptive comments on the manuscript.
References
Footnotes
Twitter Follow Carl May at @CarlRMay and Frances Mair at @FrancesMair
Contributors CRM drafted this paper; CRM, AR, KB and FSM developed the conceptual framework informing this study; CRM, PG, MM, CP, PR and AR designed the review; MA performed database searches; AC, MM and CRM screened titles, abstracts and full papers with assistance from JH; CRM performed first-line content analysis; MA, KB, AC, PG, JH, FSM, MM, CP, AR and PR critically reviewed the manuscript for important intellectual content; all authors approved the final version of the paper. CRM is guarantor.
Funding This work was supported by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC) Wessex which is a partnership between Wessex NHS organisations and partners and the University of Southampton. Funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests CP declares consultancy payments from National Institute for Health and Care Excellence and the Department of Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.