Article Text

Abstract
Objective To evaluate the effect of aerobic exercise on cognitive function in people with mild cognitive impairment (MCI).
Design Systematic review and meta-analysis of aerobic exercise intervention for cognitive function in older adults with MCI.
Data sources PubMed, EMBASE, SinoMed, China National Knowledge Infrastructure (CNKI), Wanfang and Chinese Science and Technology Periodical (VIP) databases from their inception to 31 January 2015, the Cochrane Central Register of Controlled Trials (Cochrane Library, 2015, Issue 3) and the reference lists of all retrieved articles.
Eligibility criteria Randomised controlled trials, older adults with MCI, aerobic exercises compared with no specific exercise intervention for global cognitive ability and any specific domains of cognition.
Data synthesis Meta-analysis was conducted with RevMan V.5.3 software using the fixed-effect model for the available data without significant heterogeneity, or the random-effect model was used if appropriate.
Results 11 studies were identified involving 1497 participants. Meta-analysis showed that aerobic exercise significantly improved global cognitive ability (Mini-Mental State Examination (MMSE) scores: MD=0.98, 95% CI 0.5 to 1.45, p<0.0001; Montreal Cognitive Assessment (MoCA) scores: MD=2.7, 95% CI 1.11 to 4.29, p=0.0009); weakly, positively improve memory (immediately recall: SMD=0.29, 95% CI 0.13 to 0.46, p=0.0005; delay recall: SMD=0.22, 95% CI 0.09 to 0.34, p=0.0005). No significant improvement was found in other domains of cognition.
Conclusions Aerobic exercise led to an improvement in global cognitive ability and had a positive effect with a small effect size on memory in people with MCI. However, owing to the limitations of the included studies, these findings should be interpreted cautiously.
- Aerobic fitness
- Neurology
- Elderly people
- Intervention efficacy
- Meta-analysis
Statistics from Altmetric.com
Introduction
Dementia and Alzheimer's disease (AD) are the leading causes of loss of independence in daily activities and quality of life and even increased morbidity among the elderly. Mild cognitive impairment (MCI) is a syndrome defined as cognitive decline greater than expected for an individual's age that does not notably interfere with daily activities.1 It can be considered an intermediate stage in the progression from normal ageing to dementia or AD.2 ,3 Its prevalence in adults aged above 65 years is between 3% and 19%,4 and of these people 20–46% develop AD or dementia within 3–5 years compared with 3% of healthy adults of the same age.5 MCI can thus be regarded as a strong risk factor for dementia and AD.6 Nonetheless, up to 22% of patients with MCI could be restored to normal cognitive function over time through early appropriate intervention.7 Consequently, special attention should be devoted to its management.
Medications alleviate the cognitive and behavioural symptoms of MCI in some individuals,8 ,9 but a meta-analysis showed that medications do not slow the progression of dementia.10 Moreover, individuals with MCI mainly experience memory problems along with or without other domain deficits of cognition that are usually not severe enough to substantiate a dementia diagnosis. It is therefore debatable whether treatment based solely on drug intervention is appropriate. Non-pharmacological management may thus serve to complement drug treatment.11–13
A growing number of studies indicate that physical activity/exercise may improve cognitive function. In Hamer's review of prospective studies, there was an inverse relationship between physical activity/exercise performed and the risk of cognitive decline in healthy older adults.14 This evidence is also supported by cross-sectional studies, longitudinal observational studies and prospective intervention trials.15–20
For patients with cognitive impairment, the association between physical activity/exercise and disease is less consistent. For example, a meta-analysis of 14 randomised controlled trials (RCTs) reported no significant evidence that physical activity/exercise improved cognitive function in individuals with MCI.21 However, a recent systematic review indicated that physical activity or exercise had some positive effects on cognition, mainly on global cognition, executive function, attention and delayed recall of participants with MCI.22 The limitations of these studies included the widely inclusive definition of physical activity/exercise interventions—aerobic, isometric and resistance exercise, as well as their combinations. If there is a distinct relationship between specific types of physical activity/exercise and cognitive function is not known, further clarification is necessary to determine which types of exercise interventions truly benefit cognitive function.
Several studies have primarily focused on the effect of aerobic exercise on cognition in adults with neurological disorders and a previous review reported only limited benefits of exercise.23–26 The aim of our study was to systematically evaluate the effect of aerobic exercise on cognitive function, including global cognitive ability and specific domains of cognition, in older adults with MCI.
Methods
Protocol and registration
The protocol of this study was registered at the International Prospective Register of Systematic Review, PROSPERO, under the identification CRD42015016392 and can be integrally assessed online (http://www.crd.york.ac.uk/PROSPERO/disply_record.asp?ID=CDR42015016392).
Literature search
Seven electronic databases, including PubMed, EMBASE (OVID), SinoMed, China National Knowledge Infrastructure (CNKI), Wanfang degree and conference papers database, Chinese Science and Technology Periodical Database (VIP) from their inception to 31 January 2015, and the Cochrane Central Register of Controlled Trials (Cochrane Library, 2015, Issue 3), were searched without language restrictions. Relevant keywords relating to aerobic exercise as Medical Subject Heading terms and text words (eg, ‘Aerobic Exercise’, or ‘Exercise’ and ‘Physical activity’) were used in combination with words relating to cognitive impairment (eg, ‘Mild cognitive Impairment’, ‘Mild Neurocognitive Disorder’ and ‘Cognitive decline’). Additional trials were found through the reference lists of all retrieved articles. The complete search strategy is available in online supplementary appendix 1.
Supplemental material
Inclusion criteria
The trials selected in this review met the following inclusion criteria: (1) study design: RCTs, including whether published or unpublished. (2) Participant: older adults (60 years and older) with MCI by any available diagnostic criteria, such as Petersen criteria, 2004 MCI Key Symposium criteria, US mental disorders fourth edition of the Diagnostic and Statistical Manual (DSM-IV) and other standards and consensus. Those with vascular cognitive impairment or other neurological disorders resulting from AD, dementia or Parkinson's disease were excluded. (3) Intervention: aerobic exercises regardless of the styles (eg, yoga, Tai Chi, treadmill) were practised in the experimental group for at least 4 weeks with more than one exercise session per week. (4) Control: no specific exercise intervention was used in the control group, that is, participants in the control group only maintained their usual physical activities or were administered sham exercises (eg, stretch and balance). (5) Outcomes: global cognitive ability and any specific domains of cognition, including memory, attention, language, verbal fluency, visuospatial ability or executive ability, that were measured by neuropsychological tests or other objective measurements. Those without available data were excluded.
Study identification and data extraction
Literature search, study identification and data extraction were conducted between December 2014 and February 2015. All searched records were imported into the reference management software (Note Express V.2.0) to eliminate duplicate records. The full texts of the studies that potentially met the inclusion criteria were obtained to further evaluate their eligibility. Any disagreements were resolved by discussion with the third reviewer (GZ). Data were extracted by one reviewer (RX) using the prepared form and checked for accuracy by another reviewer (GZ). The extracted information from eligible studies included participants' characteristics, sample size, study design, methodological information of study quality, experimental and control intervention, duration, frequency, intensity and style of aerobic exercise, outcomes and adverse events.
Assessment of risk of bias in individual studies
Two reviewers (RX and WZ) independently evaluated risk of bias of included studies using Cochrane Collaboration's tool for assessing the risk of bias.27 The six recommended domains involving seven items included selective bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessors), attrition bias (incomplete outcome data), reporting bias (selective reporting) and other bias. The overall judgement of each item for each study was categorised as ‘low’, ‘high’ and ‘unclear’ according to the levels of bias. Discrepancies between reviewers were resolved by the third reviewer (GZ).
Data analysis
Review Manager software V.5.3 provided by Cochrane Collaboration was used for the statistical analysis, and the statistical significance was defined as two-sided p value of <0.05. Data were summarised using relative risk with 95% CI for binary outcomes, and mean difference (MD) or standardised MD (SMD) with corresponding 95% CI for continuous outcomes. The pooled effect was calculated using the fixed-effect model if data were available and no significant heterogeneity was detected. Otherwise, the random-effect model was applied. However, when the heterogeneity among studies was high (I2>75%), the overall pooled analysis was not considered appropriate and the subgroup was considered to be performed according to the causes of heterogeneity including characteristics of measurement tools (ie, global cognitive ability being measured by Mini-Mental State Examination (MMSE), Alzheimer's Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) and Montreal Cognitive Assessment (MoCA) and measurement units (ie, executive ability being expressed by reaction time and MoCA scores). Statistical heterogeneity among the included studies was assessed using a χ2 test and Higgins I2 value, with I2>75% suggesting high statistical heterogeneity.28
Results
Study identification
1768 records were identified from preliminary searches according to the predetermined search strategy. Two reviewers (XR, ZWJ) disregarded obviously irrelevant records based on the abstract or the title. A total of 36 potential studies were further evaluated for their eligibility, and 14 studies ultimately fulfilled the inclusion criteria.29–49 However, three studies did not provide the original data.47–49 We attempted to contact the original authors by email but did not receive any responses. Therefore, we excluded these three studies. In the end, 11 studies involving 1497 participants with MCI were included in the review. The detailed screening flow used to find eligible studies is presented in figure 1.

Flow diagram for searching and selection of the included studies. CNKI, China National Knowledge Infrastructure; MCI, mild cognitive impairment; RCT, randomised controlled trial; VIP, Chinese Science and Technology Periodical Database.
Characteristics of included studies
The characteristics of each of the included studies are summarised in table 1. Eleven RCTs involving 1497 participants with MCI (male 565 and female 932, mean age 74.1) were included for review. The majority of included studies were conducted in America and Europe, and three came from China. Most participants were recruited from community or elderly care centres.29–33 ,35–46 All of the included studies reported clear diagnostic, inclusion and exclusion criteria for their participants.
Characteristics of included studies in this systematic review
The styles of aerobic exercise in the included studies were diverse. The most commonly used aerobic exercise was regular walking,34–44 but handball training,46 Tai Chi,31 ,32 jogging combined with Tai Chi,30 cycling,45 dance-based aerobics29 and multicomponent aerobic exercises33 were also practised. The frequency of aerobic exercise varied from two to five sessions weekly and 30–60 min per session. The duration of the intervention was 6 months or 1 year, with the exception of two studies which were 640 and 12 weeks, respectively.29 Of these 11 studies, three compared aerobic exercise with non-intervention (ie, usual physical activity).30 ,39 ,41–44 Although other studies compared aerobic exercise with stretching and/or tone exercise, social activities or health education, since the lower intensity of those activities did not significantly alter the exercise habits of the participants, we believed that those activities did not differ from non-intervention. A heart rate reserve of 40–60%, 60–80% maximum heart rate or their metabolic equivalents was applied to control the intensity of aerobic exercise in six included studies,29 ,35–39 ,41–46 and only ‘moderate intensity’ was described in others. The intervention in the control group was usual physical activity, or very low intensity of activity/exercise such as social activities, recreational activities or stretching, balance and tone exercise. There was a wide variety of cognitive measurement tools used in the studies, including MMSE, ADAS-Cog, MoCA, Rey Auditory Verbal Learning Test (AVLT) and verbal fluency test, with different tools applied to evaluate the same cognitive domain within a study or among studies.
Risk of bias of included studies
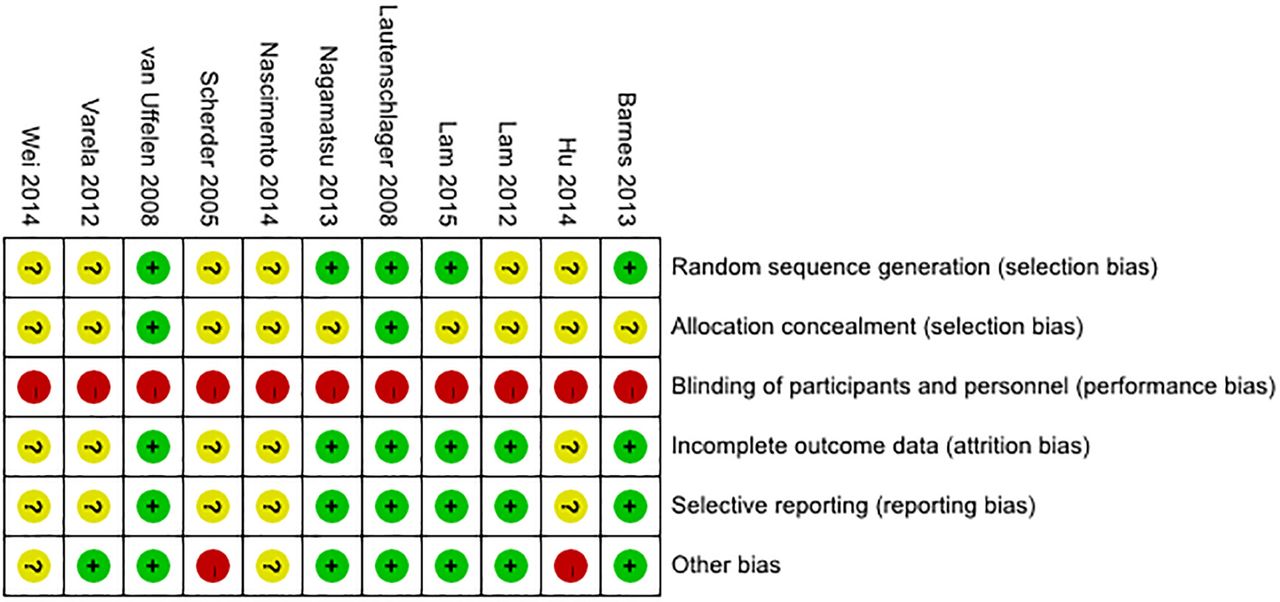
Figure 2 is a summary of the risk of bias of included studies. All included trials reported randomisation allocation but only five of them described the method of randomisation sequence generation by specifically using a random number generator on a computer,29 ,34 PI (LCWL),33 website,35–38 or SPSS statistic software.41–44 Two studies clearly reported allocation concealment, specifically ‘allocation numbers were kept in sealed containers’,34 or set key.41–44 The risk of potential performance bias was high in all included studies because it was difficult to blind participants and blind personnnel and staff in the trials to the exercise intervention. Six studies blinded the outcome assessors; therefore, their risk of detection bias was judged as low.29 ,31–38 ,41–44 The risk of attrition bias was low in six studies because the research data are complete or the number of missing data and the reasons they were missing were described.29 ,31–38 ,41–44 The selective reporting bias in six studies was judged as low risk by checking their available protocol.29 ,31–38 ,41–44 The risk of other bias was high in two studies because of the limited sample size,39 and unclear comparison of baseline characteristics between the intervention and control groups.30

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Effect of interventions
Global cognitive function
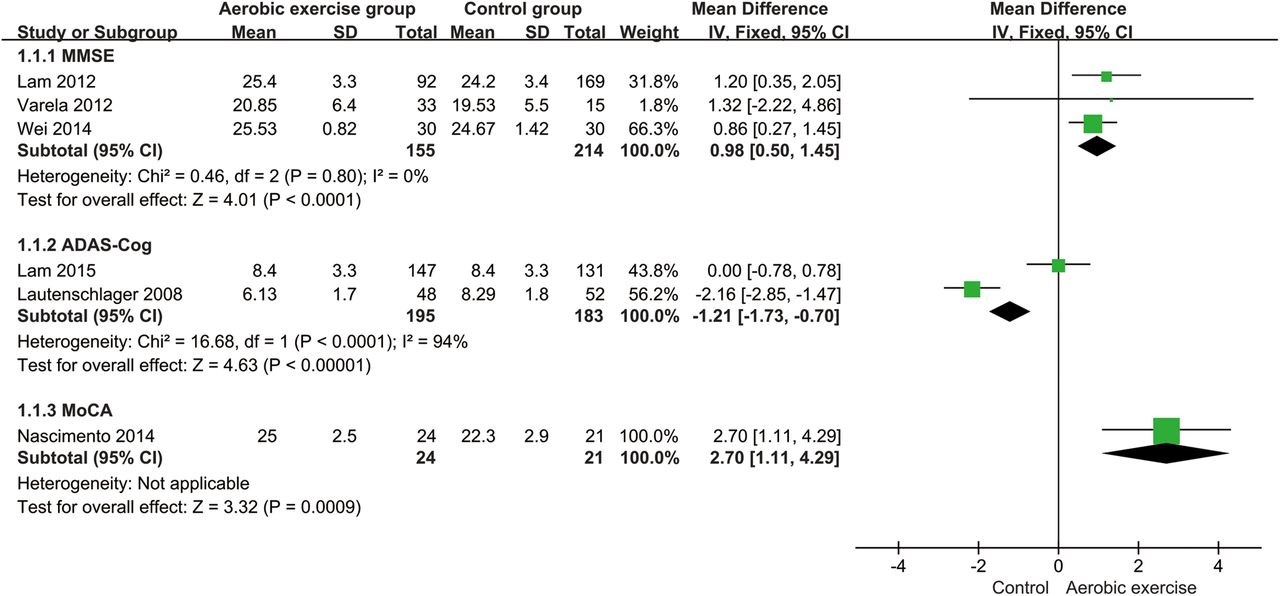
Six studies31–34 ,39 ,45 ,46 reported the effects of aerobic exercise on global cognitive ability in participants with MCI measured by using MMSE, ADAS-Cog and MoCA. However, an overall pooled analysis was not appropriate because the measured results using different tools among studies were incompatible. The results of the subgroup analysis showed that aerobic exercise had a significant effect on improving global cognitive ability among participants with MCI by significantly increasing MMSE scores (n=369, MD=0.98, 95% CI 0.50 to 1.45, p<0.0001, I2=0%, the fixed-effect model) and MoCA scores (n=45, MD=2.70, 95% CI 1.11 to 4.29, p=0.0009). Two studies reported ADAS-Cog scores, but their subgroup analyses were not appropriate because of substantial heterogeneity (I2=94%), and one study showed that aerobic exercise significantly improved global cognitive ability by decreasing ADAS-Cog scores (MD=−2.16, 95% CI −2.85 to −1.47, p<0.0001), while another reported no significant changes (figure 3).
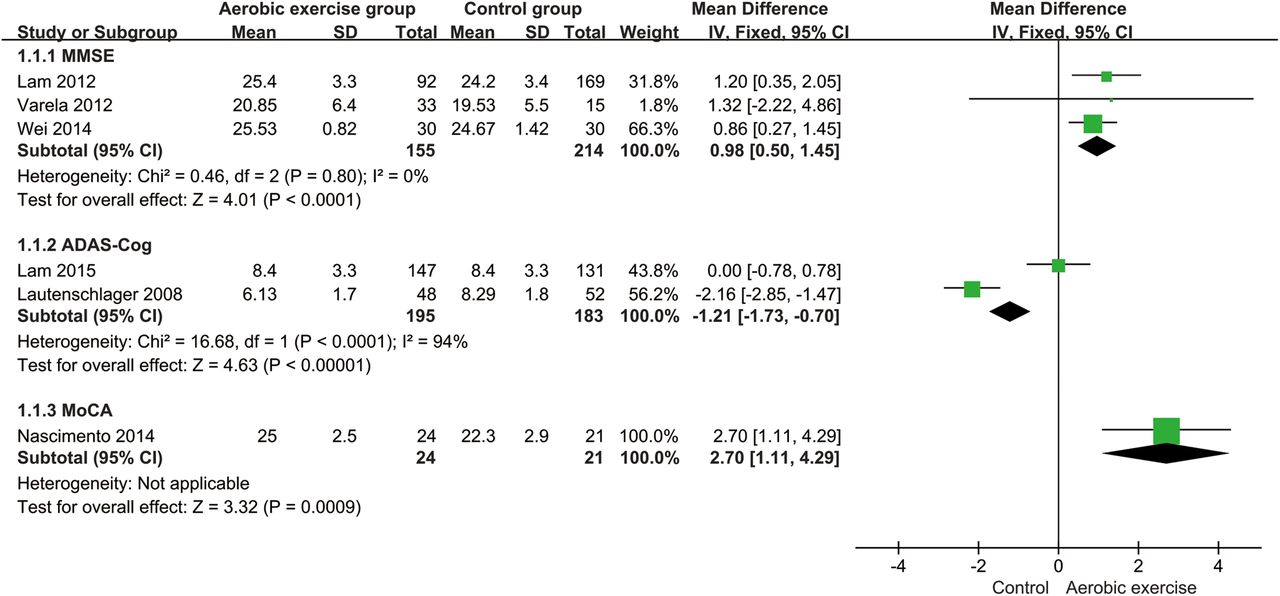
Forest plot for aerobic exercise on global cognitive ability. ADAS-Cog, Alzheimer's Disease Assessment Scale-Cognitive Subscale; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment.
Memory
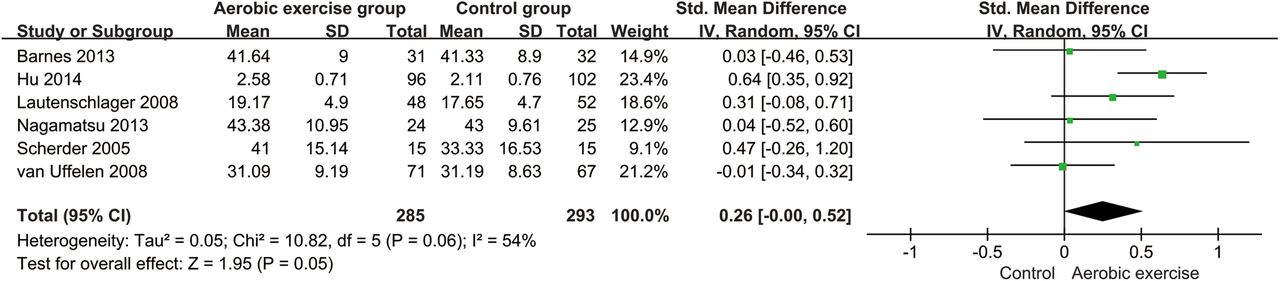
Six studies with a total of 578 participants reported the effects of aerobic exercise on immediate recall ability measured by AVLT,29 ,35–38 ,40–44 word list34 and MMSE (immediate recall ability).30 Results showed that participants in the aerobic exercise group had a significant improvement in SMD scores of the immediate recall ability compared with controls (n=578, SMD=0.26, 95% CI 0.00 to 0.52, p=0.05, I2=54%, the random-effect model; figure 4).
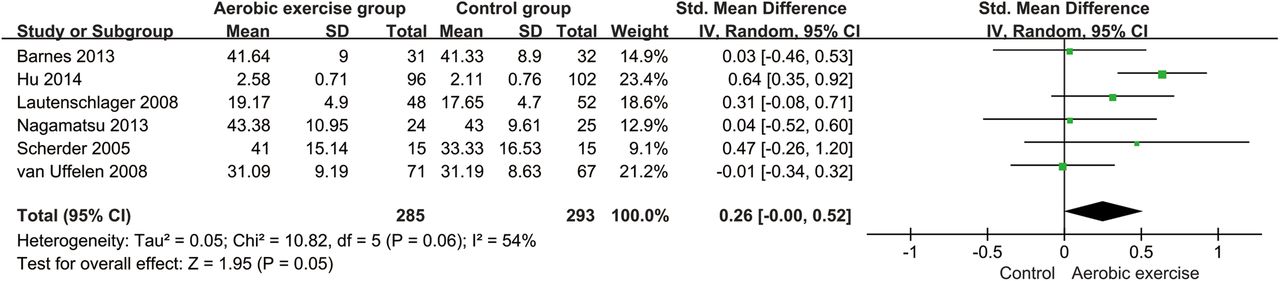
Forest plot for aerobic exercise on immediately recall ability.
Seven studies involving 1068 participants assessed the effects of aerobic exercise on delayed recall ability of memory measured by AVLT,29 ,40–44 word list,33 ,34 10 min delayed recall31 ,32 and MMSE scores.30 Meta-analysis showed that aerobic exercise significantly improved delayed recall ability in patients with MCI (n=1068, SMD=0.25, 95% CI 0.05 to 0.45, p=0.01, I2=57%, the random-effect model; figure 5).

Forest plot for aerobic exercise on delayed recall ability.
Attention
Four studies31 ,32 ,34 ,40–44 compared the aerobic exercise and control groups in terms of attention measured by visual span31 ,32 ,40–44 and digit symbol coding.34 The results of meta-analysis showed no significant difference between the aerobic exercise and control groups (n=529, SMD=0.14, 95% CI −0.04 to 0.31, p=0.76, I2=0%, the fixed-effect model; figure 6).

Forest plot for aerobic exercise on attention.
Executive ability
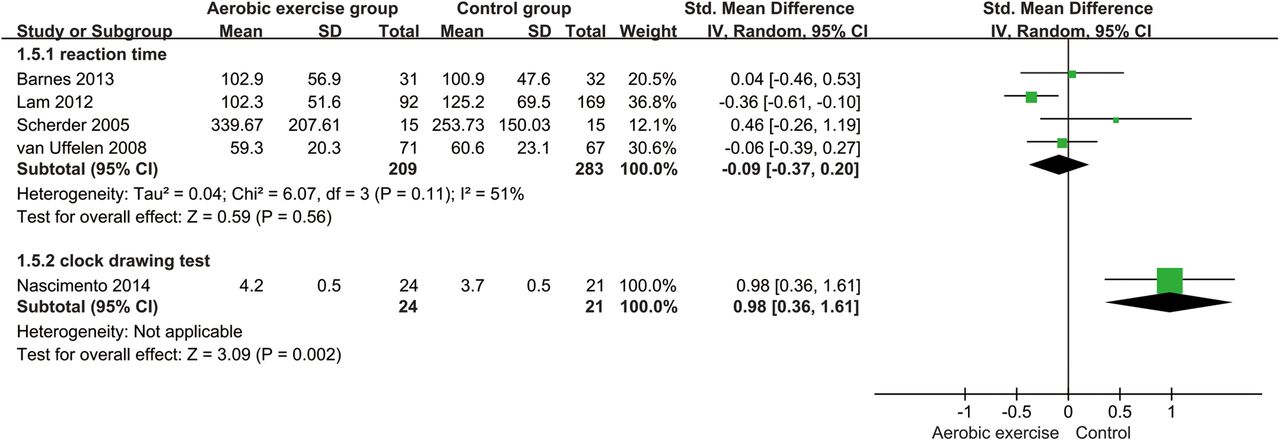
The effects of aerobic exercise on executive ability were evaluated in five studies using the complete Trail-Making Test40 or only the Trail-Making Test part B (ms),29 ,31 ,32 Stroop colour word test-abridge task 3 (s)41–44 and MoCA (clock drawing test).39 Owing to the different tools, we used subgroup analysis. Meta-analysis showed that aerobic exercise did not significantly decrease reaction time (n=492, SMD=−0.09, 95% CI −0.37 to 0.20, p=0.56, I2=51%, the random-effect model). However, another study39 reported that aerobic exercise significantly increased MoCA (clock drawing test) scores (n=45, MD=0.98, 95% CI 0.36 to 1.61, p=0.002; figure 7).
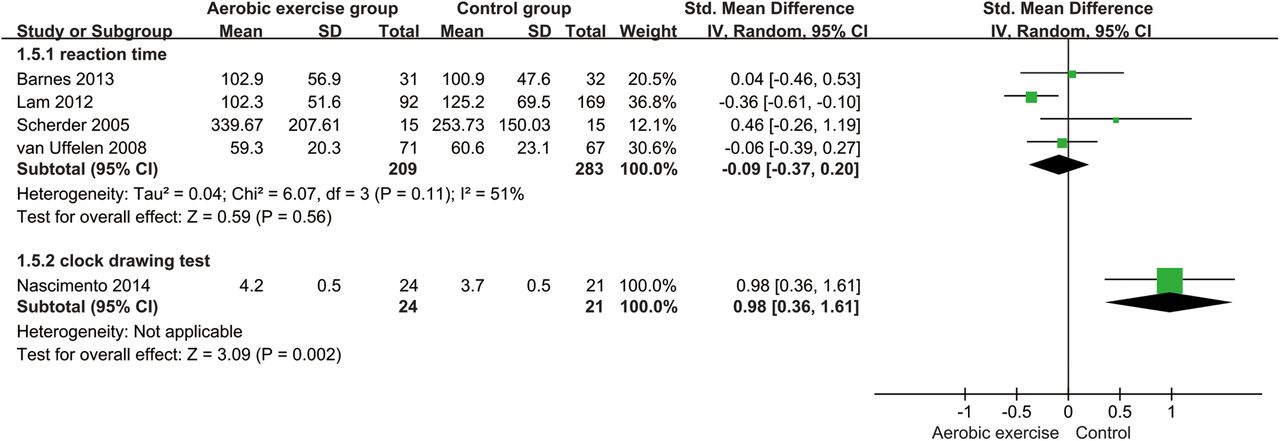
Forest plot for aerobic exercise on executive ability.
Verbal fluency
Five studies with 840 participants assessed verbal fluency using the verbal fluency test.29 ,31–34 ,41–44 Meta-analysis showed no significant difference between the aerobic exercise and control groups (n=870, SMD=−0.16, 95% CI −1.74 to 1.42, p=0.84, I2=43%, the random-effect model; figure 8).

Forest plot for aerobic exercise on verbal fluency.
Visuospatial function
One study examined the effects of aerobic exercise on visuospatial function using useful field of view (ms),29 which was divided into three different parts including processing speed, divided attention and selective attention. The results showed no significant difference between the aerobic exercise and control groups (processing speed: n=63, SMD=2.99, 95% CI −19.15 to 25.13, p=0.79; divided attention: n=63, SMD=13.76, 95% CI −46.98 to 74.50, p=0.66; selective attention: n=63, SMD=−21.56, 95% CI −72.79 to 29.67, p=0.41; figure 9).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for aerobic exercise on visuospatial function.
Adverse effects
No serious adverse events were reported during aerobic exercise training in the included studies. Only one study reported two people with shortness of breath and four falls without any physical injury.35–38
Discussion
This systematic review and meta-analysis provides some findings that aerobic exercise has positive benefits in improving the cognitive ability of older adults with MCI. Regarding global cognitive function, the pooled result showed that aerobic exercise significantly improved global cognitive function in older adults with MCI. Within the specific domain of cognition, aerobic exercise had weak significant benefits on memory, including immediate recall and delayed recall ability, and potentially positive effects on executive ability. However, no significant improvement was found in the attention, verbal fluency or visuospatial domain. No adverse events related to aerobic exercise was reported in any of the included studies.
Strengths and limitations
The strengths of this review relate to its systematic approach in which methodologically stronger study designs were used than in previous reviews. First, we focused on types of aerobic exercise rather than physical activity/exercise. Although ‘physical activity’, ‘exercise’ and ‘aerobic exercise’ are often used interchangeably in the studies, their concepts are different.50 ‘Physical activity’ refers to any bodily movement and includes a broader range. ‘Exercise’ instead refers to planned or structured physical activity that can include aerobic exercise, resistance training or their combination. ‘Aerobic exercise’ refers to a use of oxygen that adequately meets the demands of exercise.51 In the current review, we also included some body-mind exercises such as Tai Chi and yoga because those exercise types have been demonstrated to belong to aerobic exercise.52 ,53 The evidence from basic and population-based studies indicates that aerobic exercise may be an important protective factor of cognitive health by changing chemical factors such as neurotransmitters and brain-derived neurotrophic factors in the brain, increasing haemodynamics within the brain, regional brain volume and brain activation patterns, as well as warding off diseases or risk factors related to cognitive impairment, such as diabetes, hypertension and inflammation.54 ,55 ,20 The majority of included studies controlled the intensity of the aerobic exercise intervention by 60–80% maximum heart rate, 40–60% heart rate reserve29 ,35–39 ,45 ,46 or by their metabolic equivalents (over three metabolic equivalents).41–44
Second, only RCTs were included in this review, and there implied that those included studies had prospective observation and rigorous study design. For participants, we paid more attention to the community of older adults with MCI. In an attempt to reduce potential confounding bias and allow for generalisability at a population level, those participants who suffered from secondary cognitive impairment, such as vascular dementia, or severe cognitive impairment, such as AD, were excluded. All of those approaches were helpful in supporting the causal hypotheses related to aerobic exercise and its outcomes.
This study has several limitations. First, the type and frequency of aerobic exercise used in the included studies ranged from walking programmes, dancing, jogging, and cycling, handball training and even Tai Chi, as well as their combinations, which varied from 30 to 90 min per session and from three to five sessions per week. Given the variability in types of aerobic exercise intervention and measures of cognitive outcome, it was difficult to determine a distinct relationship between specific types of aerobic exercise and improvement in specific cognitive domains. The intervention duration of the included studies ranged from 6 weeks to 1 year and over two-thirds lasted up to 6 months or 1 year. It is possible that improvements in some cognitive domains may occur after completion of the 6–12 month exercise intervention, but other domains may take a longer time to develop. For example, when using MMSE as the outcome measure, two studies showed significant positive effects after 6 months,31 ,32 ,46 whereas another study with a 3-month intervention period did not find a significant difference.45 No significant positive effects were found in two studies with a 6-week or 12-week intervention period.29 ,40 As such, better standardisation of the types of aerobic exercise and appropriate intervention duration could have more effectively determined the specific causal relationships.
Similarly, the outcome measures related to cognitive function in the included studies were wide-ranging. Most of the measurement methods, such as MMSE and MoCA, were objective and had high validity and reliability.56 ,57 Although 6 of the 11 included studies evaluated the effect of aerobic exercise on global cognitive function and showed significant positive effects, the effect sizes could not be accurately calculated because of the variety of non-compatible measurement tools used. Future studies should make use of more objective testing methods or instruments (eg, event-related potential and functional MRI). The effect of aerobic exercise on different cognitive domains was also evaluated in some included studies, but few studies measured the same cognitive domain using the same measurement tools. Furthermore, most cognitive domains other than memory and executive function included small numbers of studies and samples. Thus, the measurement methods and data heterogeneity may prevent us from ascertaining an association between aerobic exercise and specific cognitive domains, even though the outcomes were standardised.
In addition, it is impossible to blind participants in an exercise intervention trial; therefore, performance bias may be inevitable. Publication bias was not observed by funnel plot analysis because of the insufficient number of included studies.58 In some case, the included studies were also limited by the small participant numbers. Seven of 11 included studies had sample sizes under 100, which most likely inflated type I error and caused low statistical power. Thus, the overall strength of the evidence in this review should be interpreted with caution.
Clinical implications and recommendations for future studies
In patients with MCI, aerobic exercise appears to ameliorate global cognitive function and memory. The meta-analysis shows that low-to-moderate training intensity, with realistic frequency and duration of training, produces virtually no adverse effects and suggests that aerobic exercise could be a feasible intervention for patients with MCI. We provide clinicians with positive evidence of an effective option to recommend those patients with MCI who would benefit from increasing aerobic exercise.
Future studies in this field should use appropriate training intensity and frequency such as the exercise training principles suggested by Campbell59 or the global recommendations on physical activity for health provided by the WHO; if possible, duration of training should be at least 6 months or longer. Global cognitive ability as well as specific domains of cognition such as memory, attention and executive function should be assessed, and more sensitive and objective measurement tools should be used. In addition, authors should follow the CONSORT guidelines when reporting their studies to allow better evaluation of the quality.
Conclusion
Aerobic exercise may benefit older adults with MCI in improving global cognitive function and has a weak positive benefit on the memory domain. However, considering the discrepancies in the types, frequencies and durations of aerobic exercise interventions, as well as the limitations in the number of included studies and their small sample size, the findings must be interpreted cautiously. Larger scale trials using more rigorously designed and standardised training protocols are needed to draw specific and accurate conclusions.
What are the new findings?
Aerobic exercise significantly improved global cognitive function in older adults with mild cognitive impairment.
In the specific domain of cognition, aerobic exercise had weak significant benefits on memory, including immediate recall and delayed recall ability, and potentially positive effects on executive ability.
No significant improvement was found on attention, verbal fluency or visuospatial domain.
No adverse events related to aerobic exercise were reported in any of the included studies.
How might it impact on clinical practice in the future?
It provides positive evidence that the patients with MCI could benefit from increasing aerobic exercise.
It a useful recommend that aerobic exercise with low-to-moderate training intensity could be a feasible and effective intervention to ameliorate cognitive function for patients with MCI.
References
Footnotes
GZ and RX contributed equally.
Contributors LC, GZ and JT conceived and designed the study. RX and WZ performed the search, extraction of data and methodological assessment. RX and GZ analysed the data and wrote the paper. All authors read and approved the final manuscript.
Funding This study is supported by the National Natural Science Foundation of China (http://www.nsfc.gov.cn, grant no.81574045), and the Collaboration Innovation Center for Rehabilitation Technology (X2015001-Collaboration), Fujian provincial rehabilitation industrial institution, and Fujian Key Laboratory of Rehabilitation Technology.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.