Article Text

Abstract
Background In addition to N-terminal pro-brain natriuretic peptide (NT-proBNP), red cell distribution width (RDW), growth differentiation factor (GDF)-15, interleukin (IL)-6 and creatinine are all potential circulating prognostic biomarkers in pulmonary arterial hypertension (PAH).
Objective To establish the relative prognostic utility of these biomarkers in patients with idiopathic PAH (IPAH) and to identify independent prognostic markers in this disease.
Main outcome measures Circulating RDW, GDF-15, IL-6, creatinine and NT-proBNP levels were determined in 139 patients with IPAH (mean follow-up 4.0±2.4 years) and 40 age- and sex-matched healthy volunteers. Coincident clinical data and baseline haemodynamic measurements were also analysed.
Results All the biomarkers except creatinine correlated with a 6 min walk distance (6MWD; p<0.05), and all but NT-proBNP correlated with WHO functional class (p<0.01). GDF-15, creatinine and NT-proBNP correlated with mean right atrial pressures and cardiac index. RDW outperformed other biomarkers in receiver operating characteristic (ROC) analysis (area under the curve 0.820). Sensitive (>80%) ROC-derived cut-off points of RDW (15.7%, p=0.001), GDF-15 (779 pg/ml, p<0.001), IL-6 (2.5 pg/ml, p=0.019), creatinine (80.5 μmol/l, p=0.010) and NT-proBNP (491 fmol/ml, p<0.001), all predicted survival in patients with IPAH over time. All the plasma biomarkers analysed predicted survival in Cox regression analysis, as did clinical and haemodynamic parameters. However, only RDW predicted survival independently of NT-proBNP and 6MWD.
Conclusions Circulating RDW, GDF-15, IL-6, creatinine and NT-proBNP levels are all related to disease severity and may be used to predict survival in patients with IPAH. RDW added significant prognostic value to measurements of NT-proBNP and exercise capacity and may prove valuable in a multiple biomarker approach to disease stratification.
- Prognostic biomarkers
- NT-proBNP
- growth differentiation factor-15
- creatinine
- interleukin-6
- renal disease
- pulmonary arterial hypertension (PAH)
- pulmonary vascular disease
- growth factors
- inflammation
Statistics from Altmetric.com
- Prognostic biomarkers
- NT-proBNP
- growth differentiation factor-15
- creatinine
- interleukin-6
- renal disease
- pulmonary arterial hypertension (PAH)
- pulmonary vascular disease
- growth factors
- inflammation
Introduction
Circulating proteins have considerable potential to inform the clinical management of patients with pulmonary arterial hypertension (PAH).1 Currently, only brain natriuretic peptide (BNP) and its N-terminal propeptide (NT-proBNP) are recognised as clinically useful in idiopathic PAH (IPAH).1 Other biomarkers that report different pathogenic mechanisms or involvement of different tissues may add utility, particularly when determined and interpreted in combination with established clinical measures and predictors of mortality. Recently identified biomarkers that show promise include red cell distribution width (RDW),2 growth differentiation factor (GDF)-15,3 interleukin (IL)-64 and creatinine.5
RDW is measured as part of the full blood count in standard hospital analyses and quantifies the variability in red blood cell size. Anisocytosis, indicated by increased RDW, is seen in iron-deficiency anaemia, thalassaemias and myelodysplastic syndromes. RDW predicts survival in left heart failure,6 coronary disease7 and in older adults8 with hazard ratios of 1.14–1.17 per percentage increase. RDW has also recently been reported to predict survival in patients with pulmonary hypertension of mixed aetiologies, where it outperformed NT-proBNP.2
GDF-15 is a member of the transforming growth factor‐β superfamily responsive to various stimuli, including inflammation and chemical, mechanical and hypoxic stress.9 Circulating levels are raised in patients with ischaemic heart disease and chronic heart failure.10 11 Increased GDF-15 levels have been seen in patients with acute pulmonary embolism, possibly reflecting changes in right ventricular function,12 and in treatment-naïve patients with IPAH.3 GDF-15 is sensitive to hypoxia, anoxia and iron depletion,13 14 and thus GDF-15 levels may report two signalling pathways implicated in PAH: transforming growth factor‐β and hypoxia-iron sensing.
Inflammation has long been known to be a facet of IPAH15 and several data have implicated IL-6 in the development of pulmonary hypertension in in vivo models.16 17 Patients with pulmonary hypertension secondary to connective tissue disorders generally exhibit a poorer prognosis. Recently it has been shown that levels of several inflammatory molecules are raised and predict survival in IPAH, including IL-6,4 which performed strongly, predicting survival independently of haemodynamic measurements. However, the usefulness of IL-6 measurements in combination with other biomarkers such as NT-proBNP has not been assessed.
Renal dysfunction is linked to mortality in cardiovascular diseases and specifically in patients with pulmonary hypertension.18 Serum creatinine is a relatively crude but practical measure of kidney function and a large study of 500 patients with PAH has previously demonstrated its use as a prognostic biomarker.5 Renal dysfunction may also affect other biomarkers; impaired renal clearance of NT-proBNP could lead to accumulation unrelated to ventricular dysfunction, RDW is inversely related to kidney function19 and IL-6 levels are raised and predict survival in renal failure.20
These biomarkers have so far been analysed primarily in populations with incident PAH in single separate studies. We set out to examine and directly compare the performance of RDW, GDF-15, IL-6 and creatinine as putative markers of prognosis as well as NT-proBNP in a ‘real-life’ clinical setting including both incident and prevalent patients with IPAH and to explore the value of adding these biomarkers to established clinical measures in predicting survival of patients with IPAH.
Subjects and methods
Study subjects
Plasma samples from the pulmonary hypertension biorepository, Imperial College London, were used in this study. This biorepository includes samples from 139 patients with IPAH (40 incident untreated cases, 99 prevalent treated cases) attending Hammersmith Hospital, London, between 2002 and 2009 who consented to providing a blood sample for research. Ethical approval was received via the National Research Ethics Service (reference numbers 2001/6157 and 09/H0711/4). The diagnosis of IPAH was based on standard criteria, with confirmation by right heart catheterisation and exclusion of other forms of pulmonary hypertension according to the most recent guidelines.
To maximise homogeneity of data, we selected only patients with IPAH as other presentations of pulmonary hypertension are associated with differing prognoses. The inclusion of both incident and prevalent cases is also consistent with two recently published registry studies analysing survival in IPAH populations in the USA21 and France,22 though the complex bootstrapping techniques applied in the French study could not be reproduced in this smaller cohort study.
WHO functional class and 6 min walk distance (6MWD) were determined on the same day as blood sample collection. Blood samples were obtained from patients with IPAH upon enrolment either at diagnosis or at outpatient appointments during the course of the disease. Survival status was censored on 26 July 2010. Death was defined as the primary end point, and no patient was lost to follow-up. Samples were also analysed from healthy volunteers from Imperial College London, UK.
Methods
All EDTA blood samples were immediately cooled (4°C) and centrifuged at 1000 rpm for 5 min, then the plasma was removed and frozen (−80°C). Plasma GDF-15 and IL-6 levels were measured using ELISA kits (R&D Systems, Abingdon, UK) according to the manufacturer's instructions. Creatinine was measured by standard clinical pathology accreditation-approved hospital assay. RDW was measured on the Sysmex XE-2100 automated analyser (Sysmex, UK); a method based upon electrical impedance using hydrodynamic focusing. NT-proBNP levels were measured using a non-competitive assay as previously described.23
Statistical analysis
Data are presented as absolute numbers, percentages, mean (±SD), or median and centile range. The relationship between patient characteristics and biomarkers was assessed by Spearman's rank test or Mann–Whitney U and Kruskal–Wallis tests for categorical variables. Receiver operating characteristic (ROC) curves assessing 2-year all-cause mortality and all possible biomarker cut-off points and their area under the curve were used to compare prognostic values of biomarkers. Kaplan–Meier plots illustrated events during follow-up in relation to biomarker levels, assessed by the log-rank test. Several parameters were not normally distributed, as shown by the Kolmogorov–Smirnov test, and were therefore respectively transformed to their natural logarithm (ln) and square root, as appropriate to best normalise the data, before Cox analysis. Cox regression analyses identified prognostic predictors. All variables with p<0.05 were tested by proportional hazard ratios Cox regression analysis; variables were removed at p>0.10. All calculations were performed with SPSS V.17.0 (SPSS, Inc).
Results
Biomarker levels and clinical and haemodynamic measurements in IPAH
Baseline patient characteristics of all 139 patients recruited are detailed in table 1. Forty-nine patients died during follow-up. Median time since diagnosis at sampling was 1.17 years (IQR 0.2–2.5 years). Samples from 40 sex- and age-matched healthy controls were also collected (table 1). Forty patients were treatment-naïve at sampling, and 99 were sampled during the course of treatment; median time from diagnosis in the latter group was 1.40 years (IQR 0.56–2.82 years).
Subject demographics and biomarker correlations
RDW levels were, on average, towards the upper end of the normal range (15.54±2.92%) and GDF-15 (1015±933 pg/ml), IL-6 (8.6±18.7 pg/ml) and NT-proBNP (909±849 fmol/ml) levels were all raised in patients with IPAH, whereas creatinine levels were mostly within the normal range (96±30 μmol/l) (online supplementary figure 1). Levels of GDF-15 and IL-6 in healthy volunteers measured with the assays used in this study are shown in supplementary figure 2.
Biomarker relationships with coincident clinical/biochemical and baseline haemodynamic data were analysed; p values are shown in table 1. Cardiac index and mean right atrial pressures correlated with GDF-15 (ρ=−0.229, p=0.039 and ρ=0.234, p=0.030), creatinine (ρ=−0.276, p=0.012 and ρ=0.253, p=0.018) and NT-proBNP levels (ρ=−0.378, p<0.001 and ρ=0.283, p=0.008). NT-proBNP levels correlated significantly with pulmonary vascular resistance (ρ=0.321, p=0.006). RDW, GDF-15, IL-6 and creatinine levels all increased significantly with WHO functional class (p<0.01) whereas NT-proBNP did not (p=0.1). All biomarkers except creatinine correlated significantly with 6MWDs (RDW: ρ=−0.250, p=0.008; GDF-15: ρ=−0.480, p<0.001; IL-6: ρ=−0.434, p<0.001; NT-proBNP: ρ=−0.217, p=0.028) and with each other except RDW and creatinine (all others p<0.05). GDF-15 in particular correlated with all four other biomarkers (p<0.001).
Biomarkers and outcomes in IPAH
ROC curve analysis of 2 year all-cause mortality confirmed that all biomarkers measured except creatinine were significantly powerful predictors of survival (supplementary figure 2 and supplementary table 1). RDW was the strongest performer in this analysis, with an area under the curve of 0.82, followed by GDF-15 and 6MWD (0.76/0.75) which both outperformed NT-proBNP and IL-6 (0.67/0.66).
From the ROC analysis, highly sensitive cut-off values were derived (supplementary table 2) to predict mortality for RDW (15.7%, 82.4% sensitivity), GDF-15 (779 pg/ml, 88.2% sensitivity), IL-6 (2.5 pg/ml, 82.4% sensitivity), creatinine (80.5 μmol/l, 85.7% sensitivity), NT-proBNP (491 fmol/ml, 82.4% sensitivity) and 6MWD (322 m, 88.2% sensitivity). All five circulating biomarker cut-off points significantly predicted survival over time (figure 1) stratifying low- and high-risk patient groups (all p<0.05).
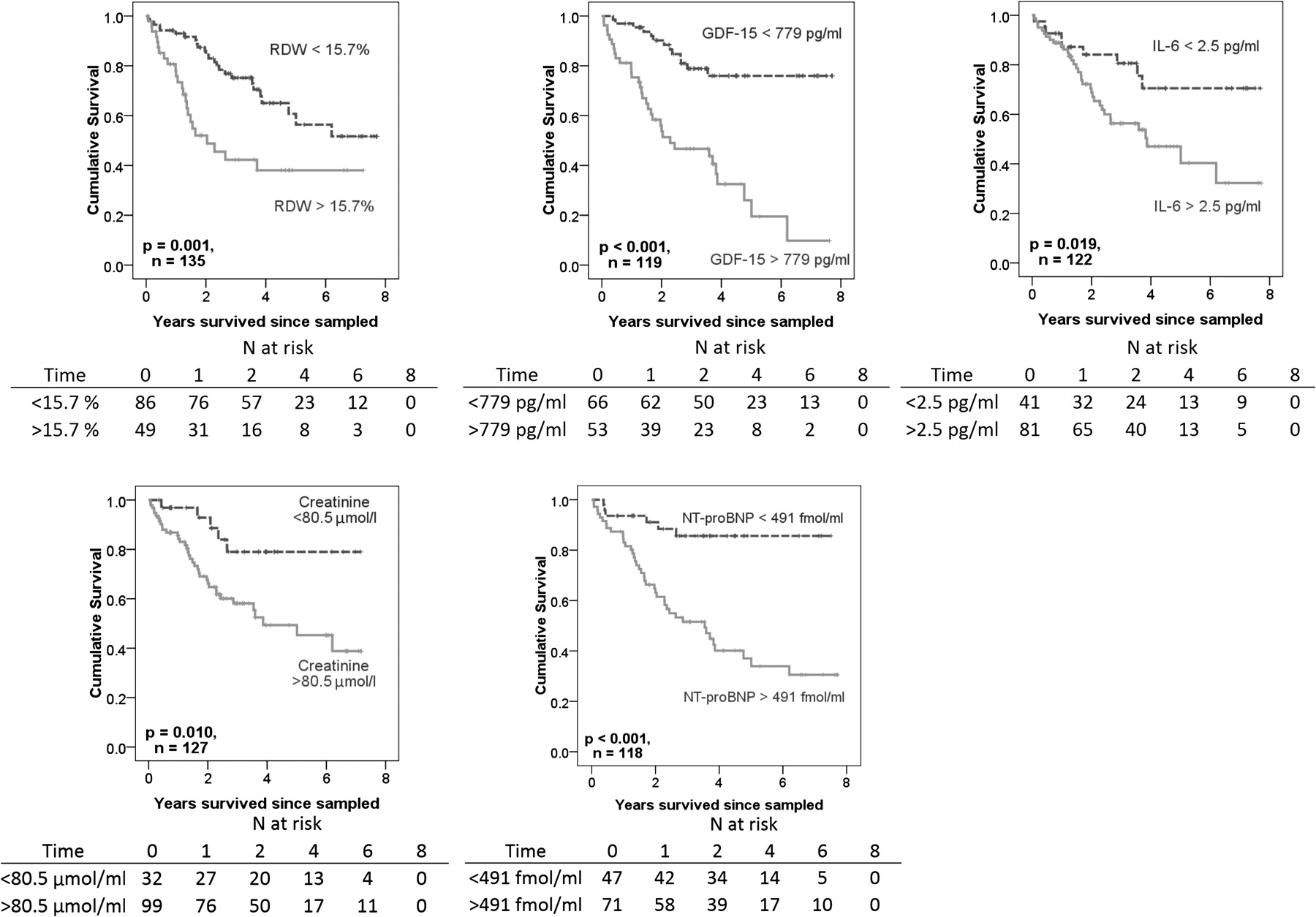
Kaplan–Meier survival curves displaying survival estimates in patients with idiopathic pulmonary arterial hypertension, stratified by biomarker levels above and below receiver operating characteristic-derived values. Tables indicate numbers at risk over time in years. GDF, growth differentiation factor; IL, interleukin; NT-proBNP, N-terminal pro-brain natriuretic peptide; RDW, red cell distribution width.
Clinical and haemodynamic parameters and outcomes in IPAH
Baseline haemodynamic data, along with functional class and 6MWD data collected coincident with blood samples was analysed by ROC in the same manner as the biomarkers above. Cut-off values were derived for haemodynamic measurements, including mean pulmonary artery pressure (57.5 mm Hg), pulmonary vascular resistance (10.9 Woods units) and cardiac index (1.87 l/min/m2). These cut-off values significantly predicted survival over time in patients with IPAH (all p<0.05, figure 2). A cut-off value of 322 m for 6MWD also significantly predicted survival over time (p<0.0001), and the two arms further separated into quartiles of 6MWD were also analysed to illustrate the powerful prognostic information provided by this simple clinical measure (figure 2). The four WHO functional classes also significantly distinguished higher mortality risks in patients with IPAH as functional class deteriorated (both p<0.01, figure 2).

{kind=link}
{kind=link}
Kaplan–Meier survival curves displaying survival estimates in patients with idiopathic pulmonary arterial hypertension, stratified by haemodynamic and clinical parameters. Cut-off points were receiver operating characteristic-derived, and 6MWD is also represented by quartiles. Tables indicate numbers at risk over time in years. mPAP, mean pulmonary artery pressure; mRAP, mean right atrial pressure; 6MWD, 6 min walk distance; PVR, pulmonary vascular resistance.
Identification of independent prognostic markers in IPAH
Cox regression survival analysis was performed to identify prognostic markers from the variables measured in this study (table 2). Time since diagnosis and the use of PAH-targeted treatments and treatment type were included as parameters to capture the effects of treatment and disease progression. Age, WHO class, 6MWD, time since diagnosis and all five biomarkers measured were identified as significant prognostic markers in IPAH (all p<0.05). All parameters with p<0.1 were entered into multivariable modelling for completeness. RDW, NT-proBNP and 6MWD were identified as significant, independent prognostic markers in IPAH (all p<0.01, table 2). No other measurements could add significant prognostic information to this model. The prognostic value of RDW was still evident in combination with either haemoglobin or mean cell volume and both RDW and IL-6 were independently prognostic when combined with creatinine (supplementary table 3).
Cox regression survival analysis
Discussion
Several novel biomarkers have been identified as prognostic in IPAH2–4 24 but rarely validated in a second cohort or directly compared in a multiple biomarker analysis. We have measured and compared RDW, levels of GDF-15 and IL-6, as well as NT-proBNP and creatinine with established clinical and baseline haemodynamic data. RDW was the strongest performer in stringent comparative statistical interrogations (ROC and Cox regression survival analyses), leading to its identification as an independent predictor of survival, even when measured in combination with 6MWD, NT-proBNP and other clinical indices.
RDW is routinely measured as part of a full blood count but has only recently emerged as a predictor of cardiovascular disease and mortality.2 6–8 It is used to distinguish anaemias, and is raised in iron-deficiency anaemia. Iron status is thought to be important in the regulation of pulmonary vascular tone,25 26 and significant iron deficiency has been demonstrated in IPAH.27–29 RDW may also be raised owing to haemolysis, but contemporaneous haemoglobin and haptoglobin (low levels indicate haemolysis) measurements did not correlate with RDW in this study and the prognostic value of RDW was independent of haemoglobin or mean cell volume. In heart failure, RDW levels are thought to represent a combination of chronic inflammation, dysfunctional erythropoiesis, kidney dysfunction, oxidative stress and nutritional state.30 For these reasons, RDW may reflect many factors relevant to the prognosis of PAH and hence provide additional prognostic information to NT-proBNP, while outperforming more specific markers such as IL-6, creatinine and GDF-15.
A variety of stimuli, including chemical, mechanical and hypoxic stress, can induce GDF-15 in many tissues. Circulating levels may reflect the function of several organs and complement NT-proBNP measurements in predicting survival in IPAH.3 Conversely, the prognostic utility of GDF-15 in a variety of cardiovascular diseases which stress the myocardium10–12 suggests that cardiomyocytes may be the predominant source of the protein. GDF-15 levels in patients with IPAH correlated with cardiac index and mean right atrial pressure, supporting this argument, though other tissue sources cannot be excluded. GDF-15 is also sensitive to iron status14 and this may explain in part its correlation with RDW values. The potential importance of the right ventricle and iron status in determining GDF-15 levels in these patients may partially explain why this biomarker did not emerge as an independent predictor of survival after adjustments for other factors, including NT-proBNP and RDW.
Inflammation is a component of pulmonary hypertension and IL-6 in particular has been linked to the development of pulmonary hypertension in experimental models.16 17 Recently, increased levels of cytokines have been shown to predict poor survival in IPAH.4 In both studies, levels above the normal range for the assay were associated with mortality, indicating that the presence of an inflammatory component in IPAH can be indicative of poor survival. However, levels do not predict survival once exercise capacity and NT-proBNP/RDW measurements have been taken into consideration. This suggests that while IL-6 measurements may be of future use in determining whether anti-inflammatory treatment strategies are appropriate in individual patients, they have limited additional clinical utility in stratifying patient risk over and above currently accepted markers.
Renal failure should be an indicator of poor prognosis in pulmonary hypertension18 and serum creatinine measurements have shown that even mild renal dysfunction is associated with poorer survival in this disease.5 Renal function is also related to haemodynamics as decreased arterial perfusion (ie, cardiac output) in the kidneys and increased renal vein pressure (ie, right atrial pressure) lead to decreased glomerular filtration rates in PAH. Indeed, we found significant correlations between serum creatinine levels and both right atrial pressures and cardiac index as well as NT-proBNP. Increased creatinine levels were also associated with a significantly poorer survival. However, it did not predict survival independently of RDW, NT-proBNP and 6MWD, and this may reflect the close relationship between renal and cardiac function, captured by NT-proBNP measurements.
In a recent study of cytokines in PAH, haemodynamic measurements performed poorly as prognostic markers. Consistent with other studies, we found significant prognostic utility in these measures, though none was independent in the final modelling. Our results agree with the NIH registry data that showed the prognostic power of mean pulmonary artery and right atrial pressures and cardiac index.31
Biomarkers with different tissue origins that provide information about different signalling pathways may give a more complete insight into disease pathology and perform better in stratifying disease when used in combination than when used alone. Hampole et al2 found that NT-proBNP added little to RDW in a population of patients with pulmonary hypertension of mixed aetiology, whereas we found the combination gave higher predictive value. The relatively long follow-up period in our study, mean 4.0±2.4 years versus 2.1±0.8 years in the study by Hampole et al, and the fact that we studied only patients with IPAH might have provided more power to detect contributions by different covariates. The inclusion of clinical measures such as 6MWD and WHO class might have also altered the relative contributions of these markers in our model. The power of RDW to improve survival predictions in combination with established measures, along with the fact RDW is already established as a standard clinical assay, suggests it may be the easiest and most useful test to add to clinical practice in the management of IPAH.
Serial BNP measurements have previously been shown to add prognostic value in cohort studies,32 but there is considerable interindividual variation in response, which compromises the use of serial BNP measurements to monitor individual patient response to treatment. RDW predicted survival independently of NT-proBNP, suggesting that these markers could be used in combination with NT-proBNP to improve risk estimates, thus providing better detection of high-risk cases than NT-proBNP alone.
A strength of this study is that it is hypothesis-driven and independently validates several of the novel biomarkers currently of interest in IPAH, comparing them not only with each other but also with the more established NT-proBNP, and clinical and haemodynamic parameters. Future studies assessing the usefulness of novel prognostic biomarkers should compare their value against other potential candidates as well as established measures. The number of patients and events analysed (139 patients, 49 deaths) in this study compares favourably with previously published biomarker studies in this condition.2–4 24 We recognise that survival modelling of both incident and prevalent patients in IPAH has its limitations. Survival in PAH is not constant over time; >10% of high-risk and very-high-risk subjects died in the first 2 months after diagnosis in the REVEAL registry study.21 We attempted to allow for this by the inclusion of treatment status and time since diagnosis as covariables in the modelling. Neither of these measures proved to be related independently to survival; this emphasises that it is the response to treatment, which can be captured through clinical observations and biochemical measurements, rather than the presence of treatment itself which is important in determining patient prognosis. It is also vitally important that no ‘immortal time’ is introduced into survival analysis33; if survival from diagnosis were considered in a group of prevalent patients their initial survival would inevitably be high. We were careful to analyse survival from sample date, reflecting our attempt to analyse the use of these biomarkers in stratifying risk at clinical follow-up appointments irrespective of the treatment status of our subjects. The majority of patients in this study were WHO class III or above and therefore these results are most relevant to severe disease.
The results of this study suggest that RDW and NT-proBNP could be used in combination to improve prognostication in patients with IPAH. This hypothesis must now be validated prospectively from diagnosis with repeat measures to test its true value in disease monitoring.
Conclusions
RDW, GDF‐15, IL‐6, creatinine and NT‐proBNP are all related to disease severity and may be used to predict survival in patients with IPAH. RDW added significant prognostic value to measurements of NT-proBNP and exercise capacity and therefore could prove of value in the future in a multiple biomarker approach to disease monitoring.
Acknowledgments
We thank Professor Ng (University of Leicester, UK) for the NT-proBNP measurements. We thank the staff of the Sir John McMichael Centre, Imperial College Healthcare NHS Trust.
References
Supplementary materials
Web Only Data hrt.2011.224857
Files in this Data Supplement:
Web Only Data hrt.2011.224857
Files in this Data Supplement:
Footnotes
Funding The work was supported by grants from the British Heart Foundation, Medical Research Council and by the NIHR Imperial Healthcare Comprehensive Biomedical Research Centre.
Competing interests None.
Ethics approval This study was conducted with the approval of the National Research Ethics Service (reference numbers 2001/6157 and 09/H0711/4).
Provenance and peer review Not commissioned; externally peer reviewed.