Article Text

Abstract
Studies of seasonal patterns of incidence of sarcoidosis may provide a better understanding of potential environmental triggers of the disease. In this study, Olmsted County, Minnesota residents who were diagnosed with sarcoidosis between 1976 and 2013 were identified based on individual medical record review. The seasonal variation of incident sarcoidosis was then calculated. The age-adjusted and sex-adjusted incidence rate of sarcoidosis was lower in autumn (2.0/100 000; 95% CI 1.5 to 2.5) compared with winter (3.2/100 000; 95% CI 2.6 to 3.8), spring (2.8/100 000; 95% CI 2.2 to 3.4) and summer (2.9/100 000; 95% CI 2.2 to 3.5, p=0.024). Subgroup analysis per decade consistently showed lower incidence of sarcoidosis in autumn.
- Sarcoidosis
- Clinical Epidemiology
Statistics from Altmetric.com
Introduction
Sarcoidosis is a systemic disorder characterised by the presence of non-caseating granuloma. It has been hypothesised that the interaction between genetic predisposition and environmental factors plays an essential role in the pathogenesis of sarcoidosis even though the exact aetiology of sarcoidosis is still not known. Studies of seasonal and regional patterns of incidence of sarcoidosis may provide a better understanding of a potential environmental trigger of this disease. However, previous studies on the seasonality of sarcoidosis have yielded conflicting results.1–5
Patients and methods
Through the resources of the Rochester Epidemiology Project (REP), all Olmsted County, Minnesota residents diagnosed with sarcoidosis between 1 January 1976 and 31 December 2013 were identified. The data linkage system allows an essentially complete identification of all clinically recognised cases of sarcoidosis as complete access to medical records of all residents seeking medical care (both inpatient and outpatient) for over six decades was available.6 Potential cases were identified from diagnostic codes related to sarcoidosis and non-caseating granuloma. Diagnosis of sarcoidosis was confirmed by individual medical record review which required physician diagnosis supported by presence of non-caseating granuloma, radiographic findings of intrathoracic sarcoidosis and compatible clinical presentations. Patients with evidence of other granulomatous diseases such as TB were excluded. The only exception for the histopathological confirmation was stage I pulmonary sarcoidosis that required only the presence of bilateral hilar adenopathy on thoracic imaging. Cases with a diagnosis of sarcoidosis prior to residency in Olmsted County were excluded. The date of diagnosis was the date that the histopathological confirmation was made. If biopsy was not obtained, the date of first abnormal thoracic imaging was used as the date of diagnosis.
Age-adjusted and sex-adjusted incidence rates were calculated using monthly population estimates for adults as the denominators. Monthly population estimates were based on decennial census counts with adjustment for estimated monthly variation in residency obtained from REP.7 Seasonal variation was compared using quasi-Poisson regression models to account for overdispersion.
Results
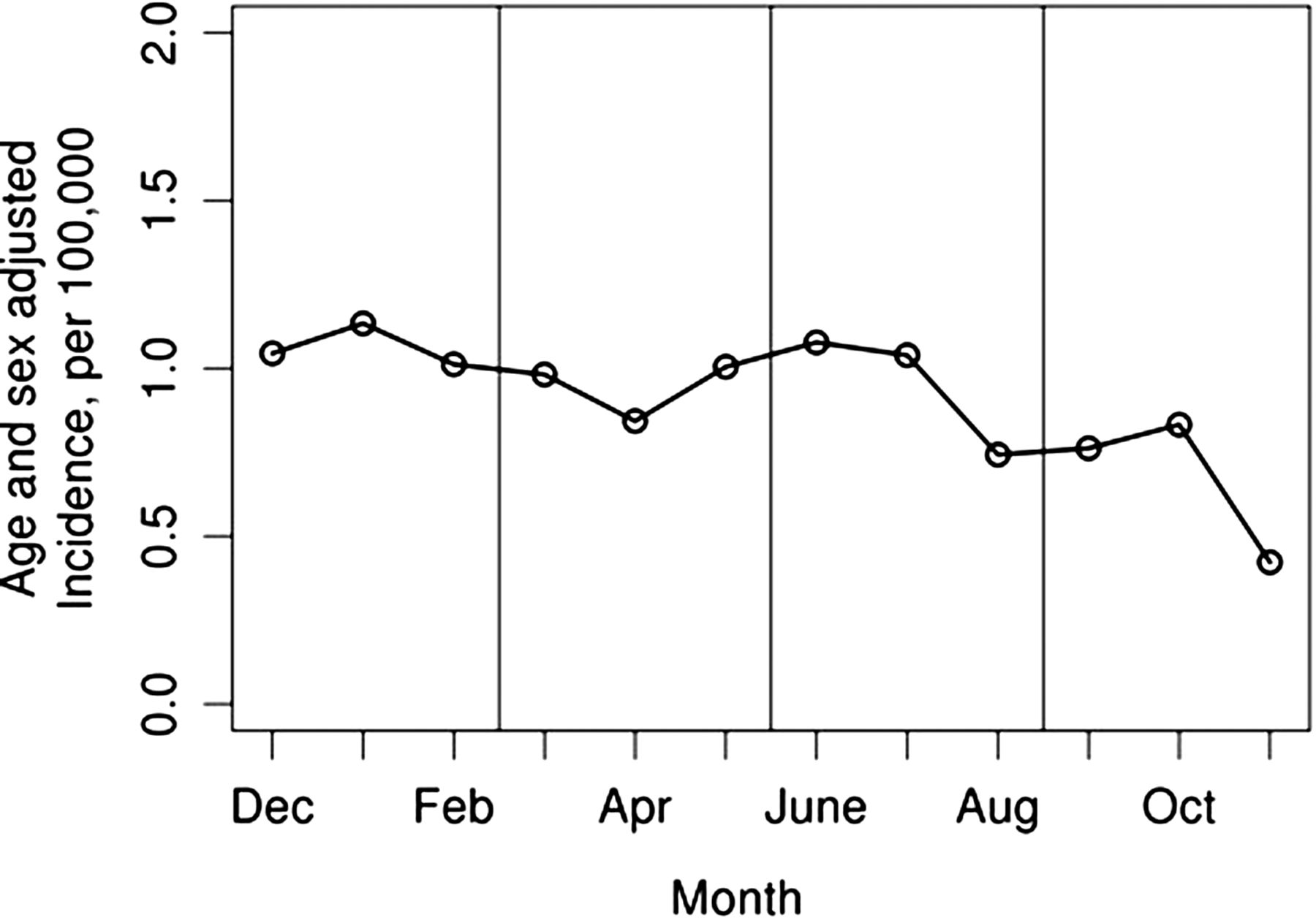
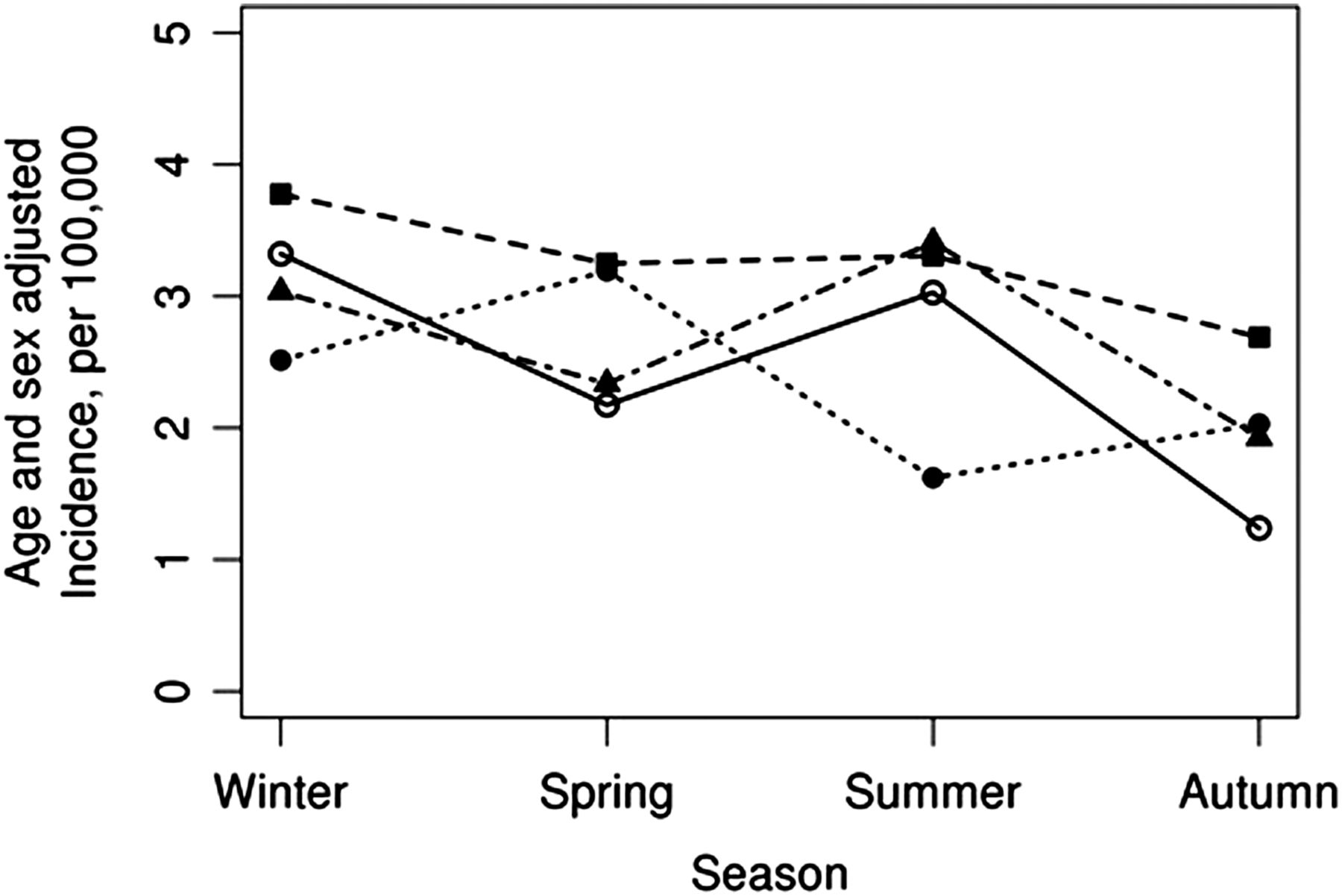
The cohort included 345 cases of incident sarcoidosis (mean age 35.4 years, 50% female, 90% Caucasian and 5% African-American). Patients in this cohort were less likely to have incident sarcoidosis in the autumn season with an age-adjusted and sex-adjusted rate of 2.0/100 000 (95% CI 1.5 to 2.5) compared with winter (3.2/100 000; 95% CI 2.6 to 3.8), spring (2.8/100 000; 95% CI 2.2 to 3.4) and summer (2.9/100 000; 95% CI 2.2 to 3.5, p=0.024; figure 1). Subgroup analysis per decade (1976–1985, 1986–1995, 1996–2005 and 2006–2013) revealed that the incidence of sarcoidosis was consistently lower in autumn (rate ratios for autumn compared with spring were 0.53, 0.70, 0.64 and 0.85, respectively; figure 2), with the exception of 1996–2005 when the lowest incidence was in summer. However, statistical power was insufficient to demonstrate statistical significance at p<0.05 for the individual decades.

Sarcoidosis incidence rates by month among Olmsted County, Minnesota residents in 1976–2013.

{kind=link}
{kind=link}
Sarcoidosis incidence rates by season among Olmsted County, Minnesota residents in 1976–2013 by decade (solid line with blank circle represents 1976–1985; dotted line with square represents 1986–1995; dotted line with filled circle represent 1996–2005; dotted line with triangle represent 2006–2013).
Discussion
This is the first study to use a population-based cohort to investigate the seasonality of sarcoidosis. There was a seasonal variation in the incidence of sarcoidosis with the lowest incidence observed in autumn. This observation was consistent over four decades except for 1996–2005. There are several possible explanations for this seasonality.
First, several environmental exposures have been identified as potential triggers for the initiation and development of granuloma in sarcoidosis.8 Thus, it is possible that the seasonality of sarcoidosis may reflect the seasonal variation in the occurrence of environmental triggers associated with its pathogenesis.
Second, the seasonal variation of sunlight may have an influence on the observed seasonality of sarcoidosis. Hypercalcaemia is a well-recognised complication of sarcoidosis as a result of upregulated 1-α-hydroxylase activity within granulomas resulting in increased conversion of 25-hydroxy vitamin D3 to 1,25-dihydroxy vitamin D3. Exposure to sunlight is important for converting 7-dehydrocholesterol to vitamin D3 and it has been demonstrated that 1,25-dihydroxy vitamin D3 as well calcium levels of patients with sarcoidosis are elevated in summer.9 This might explain the higher incidence of sarcoidosis in summer as some patients were diagnosed with sarcoidosis after they were found to have hypercalcaemia. Of course, this is speculative, and would not explain the higher incidence in winter compared with autumn.
It is also possible that the apparent seasonality is actually a result of detection bias. For example, patients might undergo thoracic imaging more often in winter and spring because of respiratory tract infections, resulting in a higher likelihood of sarcoidosis detection.
Previous studies on seasonality of sarcoidosis from different parts of the world have yielded different observations. For example, a study from Turkey2 reported the highest incidence of sarcoidosis in spring and the lowest incidence in summer, while a study from India3 showed the peak incidence in summer and the lowest incidence in winter. On the other hand, the only other study from North America, using the US Veteran Health Administration national outpatient claim database,5 did not find a significant variation in the incidence of sarcoidosis over the year. It is possible that the different patterns of seasonality between studies might reflect the different environmental stimuli in different regions/populations or it might reflect different patterns of disease presentation among different populations. For example, patients with sarcoidosis who have uveitis or Lofgren's syndrome may seek medical attention sooner than those with asymptomatic stage I pulmonary sarcoidosis, resulting in a shorter duration from onset of symptoms to diagnosis.
The major strengths of this study are that it is a population-based cohort that captures the true spectrum of sarcoidosis in the community, unlike referral-based studies. The risk of disease misclassification in this cohort is minimised as the diagnosis was individually verified by medical record, histopathology and radiographic study review.
The major limitations are those inherent in the retrospective nature of the study as the potential cases of sarcoidosis were not systematically evaluated and case ascertainment depends on diagnosis being made by the healthcare providers. Therefore, the exact burden of undiagnosed disease remains unclear. Chronological data on the onset of symptoms are often not documented, but while detection certainly follows onset of symptoms for a variable amount of time,10 case incidence is based upon when the patients came to clinical attention, reflected in the seasonality patterns reported here. Finally, the ethnic background of this cohort is predominately of northern European ancestry with a higher proportion of healthcare workers. Therefore, the observations may not be generalisable to a more diverse population.
In conclusion, seasonal variation of sarcoidosis was observed in this population with the lowest incidence observed in autumn.
Footnotes
Contributors PU: conception and design; acquisition and interpretation of data; drafting of the manuscript; statistical analysis. CSC: conception and design; analysis and interpretation of data; critical revision of the manuscript for important intellectual content; statistical analysis. ELM: conception and design; acquisition and interpretation of data; critical revision of the manuscript for important intellectual content; statistical analysis; supervision.
Funding This study used resources of the Rochester Epidemiology Project, which is supported by the National Institute on Aging of the National Institutes of Health under Award Number R01AG034676, and CTSA Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Ethics approval Mayo Clinic IRB and Olmsted County medical centre IRB.
Provenance and peer review Not commissioned; externally peer reviewed.