Article Text

Abstract
Background It is unknown if adults born <28 weeks or <1000 g since surfactant has been available are reaching their full airway growth potential.
Objective To compare expiratory airflow at 25 years and from 8 to 25 years of participants born <28 weeks or <1000 g with controls, and within the preterm group to compare those who had bronchopulmonary dysplasia with those who did not.
Methods All survivors born <28 weeks or <1000 g in 1991–1992 in Victoria, Australia, were eligible. Controls were born contemporaneously, weighing >2499 g. At 8, 18 and 25 years, expiratory airflows were measured and the results converted to z-scores. Outcomes were compared between groups at age 25 years, and trajectories (change in z-scores per year) from childhood were contrasted between groups.
Results Expiratory airflows were measured at 25 years on 164 of 297 (55%) preterm survivors and 130 of 260 (50%) controls. Preterm participants had substantially reduced airflow compared with controls at age 25 years (eg, zFEV1; mean difference −0.97, 95% CI −1.23 to –0.71; p<0.001). Preterm participants had lower airflow trajectories than controls between 8 and 18 years, but not between 18 and 25 years. Within the preterm group, those who had bronchopulmonary dysplasia had worse airflows and trajectories than those who did not.
Conclusions Young adults born <28 weeks or <1000 g in the surfactant era, particularly those who had bronchopulmonary dysplasia, have substantially reduced airway function compared with controls. Some are destined to develop COPD in later adult life.
- Paediatric Lung Disaese
- COPD epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
What is the airway capacity for survivors born <28 weeks or <1000 g since the introduction of exogenous surfactant into neonatal intensive care from the early 1990s?
What is the bottom line?
The current study confirms that survivors born either <28 weeks or <1000 g in the surfactant era, particularly those who had bronchopulmonary dysplasia in the newborn period, are not attaining the normal peak of expiratory airflow by the time they are 25 years of age.
Why read on?
As many more infants born <28 weeks or <1000 g birth weight are surviving into adulthood since the 1990s, many will present with symptoms of airflow obstruction later in life, particularly those who had bronchopulmonary dysplasia in the newborn period.
Airway growth, and hence expiratory airflow, peaks in the early 20s, followed by a brief plateau, and then steadily declines with age, which is asymptomatic in most people.1 However, some adults develop COPD, which is one of the leading causes of death in high-income countries.2 Adults born very preterm (VP; <32 weeks’ gestational age) or very low birth weight (VLBW; <1500 g) in the era before surfactant was available have more airway obstruction than do adults born at term (>36 weeks) or of normal birth weight (>2499 g).3 Not only are the mean scores for expiratory airflow in adults born VP/VLBW reduced by up to 1 SD compared with controls, but four to five times as many have expiratory flows <5th centile.3 Moreover, among preterm survivors, expiratory flows are even lower in those who had bronchopulmonary dysplasia (BPD) than those who did not.3
There are some reports of reduced expiratory airflow in late adolescence of survivors born preterm in the era when surfactant became available clinically,4 5 but the airway capacity of adult survivors of prematurity in the surfactant era is yet to be reported. Worryingly, we have shown that the rate of change in expiratory airflow through childhood into late adolescence from the surfactant era is lower in children born extremely preterm (EP; <28 weeks’ gestational age) or extremely low birth weight (ELBW; birth weight <1000 g) compared with controls.4 However, the rate of change in expiratory airflow into adulthood of survivors born EP/ELBW, including those who had BPD, in the surfactant era is unknown.
The first aim of this study was to compare expiratory airflow in early adulthood of participants born either EP or ELBW with controls of normal birth weight. The second aim was to determine if the trajectory of change in expiratory airflow from mid-childhood to early adulthood differed between the two groups. The third aim was to compare adult outcomes and trajectories from childhood between those who had BPD and those who did not within the EP/ELBW group only. It was hypothesised that expiratory airflow at 25 years and the trajectories of expiratory airflow from mid-childhood would be worse in survivors born EP/ELBW than in controls, and that among survivors born EP/ELBW those who had BPD in the newborn period would be even worse than those who did not have BPD.
Methods
This cohort study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology statement.6 The state of Victoria comprises approximately a quarter of Australia’s population. It has four tertiary neonatal intensive care nurseries (NICUs), all located in the capital city of Melbourne. All four NICUs have collaborated along with the state-wide newborn transport service and the state government’s data collection agencies to obtain long-term outcome data of all liveborn infants who were either EP or ELBW in discrete eras from the late 1970s. One such cohort was born in the 2-year period 1991–1992; exogenous surfactant became available clinically in Victoria from March 1991. Controls were infants of normal birth weight recruited in the newborn period and matched for the mother’s country of birth (primarily English-speaking or not) and health insurance status (as a proxy for social class), and the sex of the infant and the expected date of birth of a surviving infant born EP/ELBW. Perinatal data were collected prospectively during the newborn period; BPD was defined as oxygen dependency at 36 weeks’ postmenstrual age.
The EP/ELBW and control cohorts born in 1991–1992 have been assessed at 2, 5, 8 and 18 years of age; age has always been corrected for prematurity to avoid a small bias in cognitive test scores, particularly at earlier ages.7 To be consistent we have used corrected age for all assessments, including lung function, although it makes little difference to expiratory airflow conversions to z-scores to do so.8 At the 8-year and 18-year assessments, expiratory flows were measured and the results have been reported previously.4 9 At 8 years of age children were also assessed neurologically and psychologically.10 Major neurosensory disability comprised any of moderate or severe cerebral palsy, blindness, deafness or an IQ <−2 SD in those assessed at 8 years.
The cohorts were reassessed again at 25 years of age—the full protocol has been published.11 One part of the protocol related to forced expiratory airflow, which was measured using spirometry according to the American Thoracic Society and the European Respiratory Society guidelines12 by technicians who were blinded to group status of the individuals. The following values were obtained: FEV1, FVC, FEV1:FVC, and the airflow between 25% and 75% of the vital capacity (FEF25%−75%). Inhaled salbutamol was administered and the FEV1 measurement repeated—participants who improved by more than 12% from the baseline were noted. Results, including the same measures from 8 and 18 years, were converted to z-scores, % predicted and percentiles for age, height, sex and ethnicity.13 The proportions with values for airflow <5th percentile were computed.
Data analysis
Data were analysed using Stata V.15.1.14 Data at 25 years were compared between EP/ELBW and control groups, and within the EP/ELBW groups between those with and without BPD, using linear and logistic regression models fitted using generalised estimating equations reported with robust (sandwich) estimation of SEs to account for lack of independence within multiple births from the same family. If models did not converge, data were analysed using standard linear or logistic regression with error terms adjusted for clustering of multiple births.
Generalised linear mixed models were used to compare the trajectories of lung function variables over time applied to the outcomes at 8, 18 and 25 years of age between groups. Three trajectories (rates of change in z-score per year) were compared: overall from 8 to 25 years, and separately from 8 to 18 years and from 18 to 25 years. For each dependent variable, models included a fixed effect for group, age and the interaction between group and age, and a random effect for individual to allow for the repeated measures within individuals. Similar models were used for the trajectories within the EP/ELBW groups for those with and without BPD in the newborn period. Results are reported as the differences in the slopes between the respective groups, along with their 95% CIs and p values.
In subgroup analyses we compared spirometry between control and EP groups only, and between control and ELBW groups only, to determine if criteria for selection of the preterm cohort influenced any major conclusions.
Results
The flow of participants from birth, to hospital discharge, then to 8, 18 and 25 years is shown in figure 1. Ultimately there were 297 consecutive infants originally recruited in the newborn period during the calendar years 1991 and 1992 who were born EP/ELBW, and 260 controls who survived to 25 years of age, of whom 164 (55%) and 130 (50%), respectively, had expiratory airflows measured at age 25 years. Among both the EP/ELBW and control groups, there were no substantial differences in perinatal variables between those who did and those who did not have expiratory airflow data at 25 years (online supplementary table 1). Among those with expiratory airflow data at 25 years, there were expected differences between the EP/ELBW and control groups in gestational age and birth weight, and several perinatal variables, such as treatment with antenatal and postnatal corticosteroids and surfactant, and rates of BPD (table 1). Notably, there were more multiple births in the EP/ELBW group and they were shorter than the controls at each age of respiratory function testing. At 8 years of age more survivors born EP/ELBW had major neurosensory disability compared with controls, and more had asthma. At 25 years, sex, ethnicity, tobacco smoking and the mean age at testing were similar in both groups (table 1). Among the EP/ELBW group, those who had BPD in the newborn period (table 1) were less mature and lighter at birth, more were male, more were treated with surfactant and postnatal corticosteroids, more had major neurosensory disability at 8 years, and they were taller at 18 and 25 years compared with those who did not have BPD.
Supplemental material

Participant flow from birth to 25 years. EP/ELBW, extremely preterm/extremely low birth weight. *not applicable
Demographic data contrasted between EP/ELBW and control groups and between BPD and no BPD groups within the EP/ELBW cohort
EP/ELBW participants had substantially reduced airflow at 25 years of age compared with controls, whether expressed as z-scores, % predicted, percentiles or the FEV1:FVC ratio (table 2). Few participants improved their FEV1 by more than 12% after salbutamol (EP/ELBW 11% (18/159); controls 6% (7/124); OR 2.13, 95% CI 0.86 to 5.29; p=0.10). The proportion with an FEV1:FVC ratio <0.70 postbronchodilator was substantially higher in the EP/ELBW group (14%, 23/159) than in the controls (1%, 1/124) (OR 18.8, 95% CI 2.49 to 143; p=0.004).
Expiratory airflows at 25 years of age contrasted between EP/ELBW and control groups and between BPD and no BPD groups within the EP/ELBW cohort
Lung function results were almost identical in the EP-only and the ELBW-only groups, so the difference between these groups and controls were almost identical and no conclusions were altered (online supplementary table 2).
Supplemental material
Among the EP/ELBW group, those who had BPD had lower airflow at 25 years than did those who did not have BPD (table 2). Among the EP/ELBW group, few participants improved their FEV1 by more than 12% after salbutamol regardless of whether they had BPD or not (BPD 14% (9/63); no BPD 9% (9/96); OR 1.61, 95% CI 0.60 to 4.31; p=0.34). The proportion with an FEV1:FVC ratio <0.70 postbronchodilator was substantially higher in the BPD group (25%, 16/63) than in the no BPD group (7%, 7/96) (OR 4.27, 95% CI 1.66 to 11.0; p=0.003).
Substantially more EP/ELBW participants had airflow values <5th centile than did controls (table 3). Within the EP/ELBW group, those who had BPD were approximately twice as likely to have airflow values <5th centile than those who did not have BPD (table 3).
Proportions with expiratory airflows at 25 years of age <5th centile contrasted between EP/ELBW and control groups and between BPD and no BPD groups within the EP/ELBW cohort
Of the 297 participants born EP/ELBW, expiratory flows were measured in 239 (80%) at 8 years and in 209 (70%) at 18 years; 266 (90%) had expiratory flows measured at least once at 8, 18 or 25 years of age and were included in the longitudinal analysis. Of the 260 controls, expiratory airflows were measured in 208 (80%) at 8 years and in 154 (59%) at 18 years; 221 (85%) had expiratory flows measured at least once at 8, 18 or 25 years of age.
The means and their 95% CIs for z-scores for expiratory airflows at each age for EP/ELBW and control groups are shown in figure 2, along with lines joining the means illustrating the trajectories in z-scores for each airflow variable over time each group. The expected mean z-score for any variable at any age is 0, and if there was no change in expiratory airflow relative to age, height, sex or ethnicity over time, then a horizontal line for the trajectories would result.
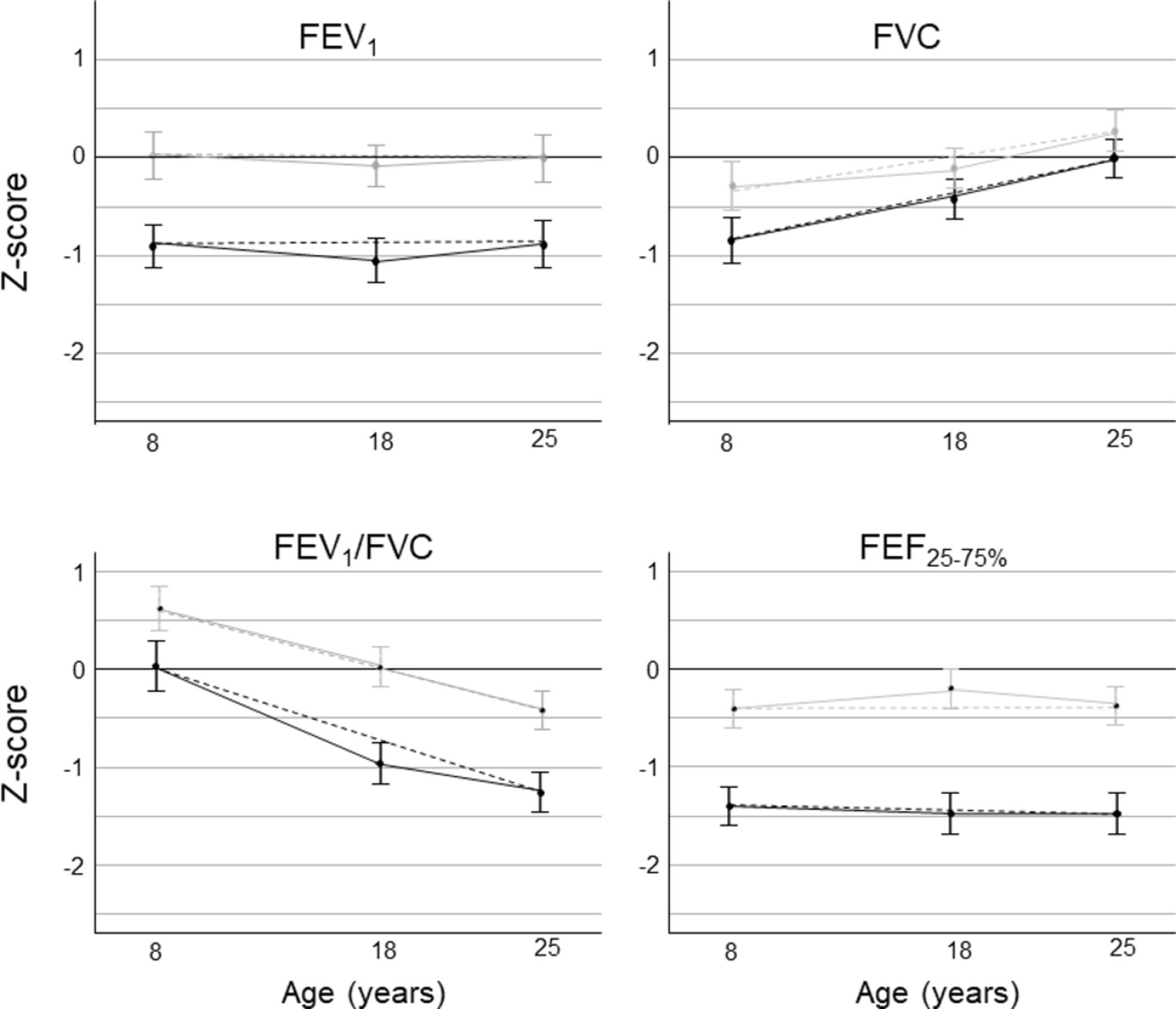
Mean values (95% CIs) for expiratory airflow z-scores at each age comparing EP/ELBW (black) and control groups (grey). Trajectories of z-scores linking the means for each expiratory airflow variable between 8 and 18 years, then between 18 and 25 years, are shown as solid lines, and between 8 and 25 years as dashed lines. EP/ELBW, extremely preterm/extremely low birth weight; FEF25%–75%, airflow between 25% and 75% of the vital capacity.
For the controls, the mean values were all close to 0 at all ages, particularly for zFEV1 (figure 2). Because there was an increase in zFVC over time with little change in zFEV1, zFEV1:FVC fell over time. zFEF25%−75% was just below but parallel to 0 over time. The mean values for the EP/ELBW group were lower than those for the controls for all variables at all ages. The patterns of trajectories for the EP/ELBW group followed those of the controls, but the gap between the EP/ELBW group and the controls seemed to diminish for zFVC and to widen for zFEV1:FVC and zFEF25%−75%, but only between 8 and 18 years.
From the mixed models regression analyses, EP/ELBW participants had higher rates of change for zFVC, but lower rates of change in z-scores per year than controls between 8 and 25 years for zFEV1:FVC and zFEF25%−75% (table 4). Most of the differences in trajectories occurred between 8 and 18 years, with little change between the two groups from age 18 to 25 years.
Differences in trajectories of expiratory airflow z-scores between 8 and 25 years, 8 and 18 years, and 18 and 25 years of age contrasted between EP/ELBW and control groups and between BPD and no BPD groups within the EP/ELBW cohorts
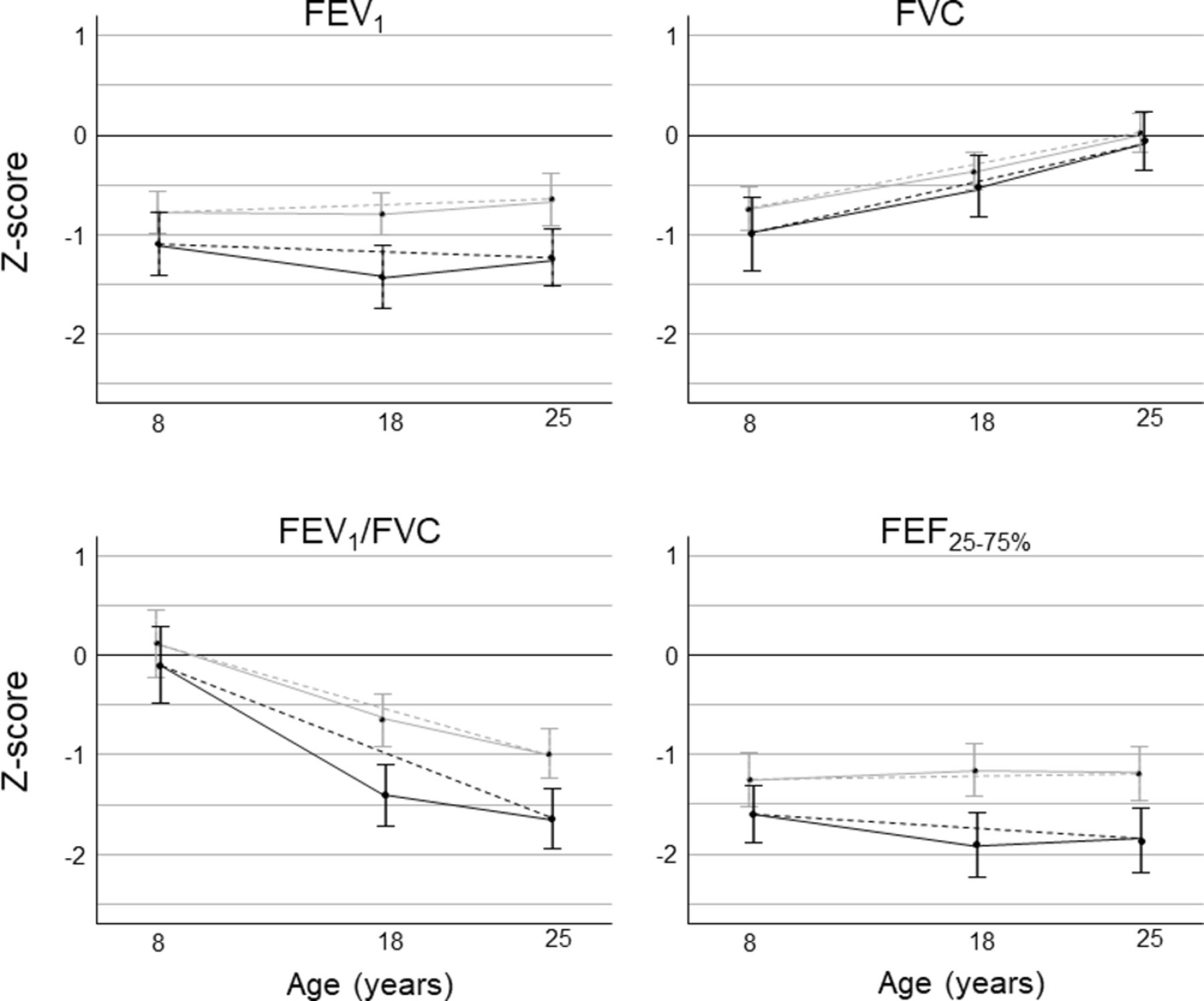
Within the EP/ELBW group, those who had BPD had lower mean values than those who did not have BPD for all variables at all ages (figure 3). The patterns of the trajectories for the BPD and no BPD groups followed each other, but between 8 and 18 years the differences between the groups seemed to widen for zFEV1, zFEV1:FVC and zFEF25%−75%. However, from the mixed models regression analyses, those who had BPD had lower rates of change in z-scores per year than those who did not have BPD between 8 and 18 years, and between 8 and 25 years for zFEV1:FVC and zFEF25%−75% only, and higher rates of change for zFVC (table 4).

{kind=link}
{kind=link}
{kind=link}
Mean values (95% CIs) for expiratory airflow z-scores at each age among EP/ELBW survivors comparing those who had BPD (black) with those who did not have BPD (grey). Trajectories of z-scores linking the means for each expiratory airflow variable between 8 and 18 years, then between 18 and 25 years, are shown as solid lines, and between 8 and 25 years as dashed lines. EP/ELBW, extremely preterm/extremely low birth weight; FEF25%–75%, airflow between 25% and 75% of the vital capacity.
Discussion
The major finding of the current study is that survivors born EP/ELBW in the surfactant era had substantially reduced expiratory flows at 25 years of age compared with normal birthweight controls. Most of the airway obstruction was fixed, with few participants in either group having substantial responses to bronchodilation. Particularly worrisome is that many more survivors born EP/ELBW than controls had values for expiratory airflow that were <5th centile. Survivors born EP/ELBW had a slower rate of change in expiratory airflow z-scores over time for some, but not all variables between 8 and 25 years of age compared with controls. The difference in trajectories between the groups primarily occurred between 8 and 18 years, with little evidence of a difference in the trajectories between 18 and 25 years. Within the EP/ELBW group, those who had BPD in the newborn period had even poorer airflow at 25 years of age and poorer growth of airflow (lower trajectories) between 8 and 25 years for some variables than those who did not have BPD. All the main findings were consistent with what we expected to find.
The differences in airflows at 25 years of age between survivors born EP/ELBW and controls are larger than the differences between 935 survivors born VP/VLBW and 722 controls from mostly the presurfactant era who were aged 16 years or more reported in a recent individual participant data meta-analysis (IPDMA).3 In the IPDMA, the mean reductions in the expiratory airflow variables between preterm and control groups were as follows: zFEV1 −0.78, zFVC −0.25, zFEV1:FVC −0.74 and zFEF25%−75% −0.88, compared with the current study: zFEV1 −0.97, zFVC −0.33, zFEV1:FVC −0.96 and zFEF25%−75% −1.20. In the IPDMA just over 50% were born EP or ELBW; the remainder were more mature and heavier at birth. The current study cohort contributed data to the IPDMA when they were 18 years of age; of the other 10 cohorts in the IPDMA, there were only 34 participants who had been treated with surfactant and there was no comparison between those exposed and those not exposed to surfactant.
The reductions in airflow in our cohort born EP/ELBW at 25 years of age have persisted from earlier in childhood.4 9 We had previously reported that there was evidence for deterioration in airflows in the small airways, reflected in the zFEF25%−75%, between 8 and 18 years in this cohort.4 Importantly, in the current study there was no evidence for further deterioration between 18 and 25 years in survivors born EP/ELBW relative to controls, or within the EP/ELBW group, between those with or without BPD. In the IPDMA, there were 117 VP/VLBW participants and 53 controls born in the presurfactant era who had airflow measured on two occasions around the same ages, 18 years and 25 years, as in the current study.3 In the IPDMA, zFVC increased between 18 and 25 years in both groups, but less so in the VP/VLBW group, whereas zFEV1:FVC decreased between the two ages, more in the controls; there was no evidence for differences in the changes between 18 and 25 years in zFEV1 or zFEF25%−75% between the groups,3 consistent with the lack of differences in the changes between 18 and 25 years in zFEV1 or zFEF25%−75% between the groups in the current study.
A major strength of the current study is the geographical cohort encompassing all survivors born EP/ELBW in the state of Victoria over 2 years in the early 1990s who have been followed to 25 years of age. The longitudinal data on expiratory flows at ages 8, 18 and 25 years in survivors born EP/ELBW in the surfactant era are unique. A control group recruited from birth with longitudinal expiratory airflow data at the same ages is also a strength, as they provide a contemporaneous group with which to compare results, rather than relying solely on reference ranges derived from different regions at different times.
A limitation is that not all survivors had expiratory flows measured at 25 years. However, given the stringent requirements for valid respiratory function tests, it is impossible to obtain expiratory airflow data from 100% of any population, and particularly not 100% of a population which has substantially higher rates of neurological impairments than controls (table 1), which preclude sufficient cooperation with the testing requirements. Follow-up rates inevitably declined with time from birth as more participants moved to other areas, states or countries, and they were unable to travel back to the centre for respiratory function testing. We had much higher proportions of both cohorts with expiratory airflow data at 8 years of age (80%), but this dwindled by 25 years of age. The follow-up rates into late adolescence/early adulthood in the studies reporting outcomes from complete cohorts included in the IPDMA were less than 50% apart from one region in Norway.3 We chose not to impute data at age 25 for those not assessed but instead used mixed models to allow us to include all the data available from any ages to calculate the trajectories of interest in the longitudinal analyses.
Another limitation is that the use of exogenous surfactant was restricted to an early surfactant, Exosurf, which contains no surfactant proteins and is rarely used today. Furthermore, when first released in 1991, infants had to have established lung disease and be in more than 50% oxygen to qualify for treatment, before that restriction was eased during 1992. Despite the restrictions on its use, 40% of the EP/ELBW cohort were treated with exogenous surfactant. The expiratory flows for adults treated with different surfactants that may be more effective than Exosurf and for those treated earlier in their clinical course may differ when they are eventually assessed at the same age as in our study. Not all infants born EP/ELBW need exogenous surfactant after birth—in the state of Victoria in 2016–2017, only 72% of EP/ELBW survivors were treated with surfactant (Cheong JLY et al, manuscript in preparation, 2019).
Asthma rates were higher in the EP/ELBW group than controls only at 8 years, and not later. The apparent disconnect between measured flow rates and symptomatic asthma in adulthood might be because few individuals were responsive to bronchodilation.
Combining EP and ELBW groups did not affect any conclusions; results were almost identical if the controls were compared with the EP and ELBW groups separately.
At the clinical level, the current study of expiratory flows to age 25 years, beyond the expected peak of expiratory flows in the early 20s, confirms that survivors born EP/ELBW in the surfactant era, particularly those who had BPD in the newborn period, are not achieving their full airway growth potential. Our results are consistent with those obtained from preterm participants in early adulthood in the presurfactant era,3 and are applicable to survivors born EP/ELBW in the early surfactant era. On a positive note, there was little evidence that the rate of change in expiratory flows was different between groups from 18 and 25 years of age, in contrast with a greater decline in variables reflecting small airway airflow (FEF25%−75%) between 8 and 18 years in the EP/ELBW group compared with controls, and within the EP/ELBW group between those with and without BPD. However, even with a normal rate of future decline with age, survivors born EP/EBW, particularly those who had BPD, are very likely to be predisposed to higher rates of COPD, or other forms of airway compromise, in later adulthood.3 This has important clinical implications in the identification, treatment and management of obstructive respiratory disease in survivors born EP/ELBW.
Areas for future research include the need for other cohorts of survivors born EP/ELBW from the surfactant era and treated with other surfactants and sooner after birth to report results into adulthood to confirm or refute our findings. However, we have reported that survivors born EP in more recent eras who were treated with other surfactants and earlier in the clinical course had more oxygen dependency, more BPD and worse expiratory flows at 8 years than those born in 1991–1992,3 so more recent cohorts may not achieve any better expiratory airflows than those reported in the current study. Clearly, our cohorts born in 1991–1992 must be reassessed later in adulthood to determine the true long-term trajectory for expiratory airflow for the earliest survivors born EP/ELBW in the surfactant era.
Footnotes
Contributors LWD: conception and design of the study, data analysis and interpretation, drafting and revising the article, and approval of the final manuscript as submitted. LI, AH, JC: conception and design of the study, data collection, revising the article, and approval of the final manuscript as submitted. KL: conception and design of the study, data analysis and interpretation, revising the article, and approval of the final manuscript as submitted. SR: conception and design of the study, revising the article, and approval of the final manuscript as submitted.
Funding Grants from the National Health and Medical Research Council of Australia (Program Grant #606789; Project Grant #491246; Centre of Clinical Research Excellence #546519; Centre of Research Excellence #1060733; Centre of Research Excellence #1153176; Project Grant #1104300; Career Development Fellowship #1141354 to JC and #1127984 to KL) and Operational Infrastructure Support Program from the state government of Victoria.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Human Research Ethics Committees at the Royal Women’s Hospital, Mercy Hospital for Women and Monash Medical Centre in Melbourne, and participants gave written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Linked Articles
- Airwaves