Article Text

Abstract
Background Pulmonary rehabilitation is a cornerstone of care for COPD but uptake of traditional centre-based programmes is poor. We assessed whether home-based pulmonary rehabilitation, delivered using minimal resources, had equivalent outcomes to centre-based pulmonary rehabilitation.
Methods A randomised controlled equivalence trial with 12 months follow-up. Participants with stable COPD were randomly assigned to receive 8 weeks of pulmonary rehabilitation by either the standard outpatient centre-based model, or a new home-based model including one home visit and seven once-weekly telephone calls from a physiotherapist. The primary outcome was change in 6 min walk distance (6MWD).
Results We enrolled 166 participants to receive centre-based rehabilitation (n=86) or home-based rehabilitation (n=80). Intention-to-treat analysis confirmed non-inferiority of home-based rehabilitation for 6MWD at end-rehabilitation and the confidence interval (CI) did not rule out superiority (mean difference favouring home group 18.6 m, 95% CI −3.3 to 40.7). At 12 months the CI did not exclude inferiority (−5.1 m, −29.2 to 18.9). Between-group differences for dyspnoea-related quality of life did not rule out superiority of home-based rehabilitation at programme completion (1.6 points, −0.3 to 3.5) and groups were equivalent at 12 months (0.05 points, −2.0 to 2.1). The per-protocol analysis showed the same pattern of findings. Neither group maintained postrehabilitation gains at 12 months.
Conclusions This home-based pulmonary rehabilitation model, delivered with minimal resources, produced short-term clinical outcomes that were equivalent to centre-based pulmonary rehabilitation. Neither model was effective in maintaining gains at 12 months. Home-based pulmonary rehabilitation could be considered for people with COPD who cannot access centre-based pulmonary rehabilitation.
Trial registration number NCT01423227, clinicaltrials.gov.
- Pulmonary Rehabilitation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
Can a home-based pulmonary rehabilitation programme, including structured goal setting and unsupervised exercise training, deliver equivalent benefits to a traditional centre-based pulmonary rehabilitation programme in people with COPD?
What is the bottom line?
This home-based pulmonary rehabilitation model resulted in short-term improvements in functional exercise capacity and health-related quality of life (HRQoL) that were at least equivalent to conventional centre-based training, and HRQoL outcomes were equivalent at 12 months following programme completion.
Why read on?
Despite being strongly recommended in treatment guidelines, pulmonary rehabilitation is currently delivered to less than 10% of people with COPD who would benefit; structured home-based pulmonary rehabilitation may be useful to enhance access for people with COPD who cannot engage in traditional programme models.
Introduction
Pulmonary rehabilitation is a cornerstone of care for people with COPD. There is robust evidence that pulmonary rehabilitation improves exercise capacity, enhances health-related quality of life (HRQoL) and reduces healthcare utilisation.1 ,2 It is strongly recommended in guidelines for COPD management.3 Over 85% of centres use an outpatient model,4 where participants attend two to three sessions each week of supervised exercise and self-management training for a period of 8 weeks or more.
Despite the compelling evidence for its benefits, pulmonary rehabilitation is delivered to fewer than 10% of people with COPD who would benefit.5 ,6 Access is particularly challenging in rural settings, where COPD is often prevalent and programmes may not be available. However, uptake and completion are also poor in metropolitan areas—up to 50% of those who are referred to pulmonary rehabilitation will never attend and of those who present at least once, up to a third will not complete the programme.7 Frequent travel to a centre-based programme, in the setting of distressing dyspnoea and mobility limitation, is regularly reported as a barrier to attendance.7 Despite consistent identification of access barriers, the pulmonary rehabilitation model has not changed in over 30 years.8
Home-based pulmonary rehabilitation is an alternative model that could improve uptake and access. Initial reports suggest that home-based pulmonary rehabilitation is safe and may improve clinical outcomes.9–12 However these studies have limitations related to the trial methods (underpowered studies, lack of assessor blinding, high attrition) and the home-based rehabilitation protocols (expensive models requiring multiple home visits, not delivering all the essential components of pulmonary rehabilitation or not entirely home-based).9–12 As a result, there has been little uptake in clinical practice, with home-based pulmonary rehabilitation offered in less than 5% of centres worldwide.4
The most recent American Thoracic Society/European Respiratory Society Policy Statement on Pulmonary Rehabilitation identified increasing the accessibility of pulmonary rehabilitation as a key priority.13 For home-based pulmonary rehabilitation to fulfil this role it must be accessible to patients, deliver the essential components of pulmonary rehabilitation, be easy to implement and result in equivalent benefits to the current ‘gold standard’ of centre-based pulmonary rehabilitation. We developed a structured model of home-based pulmonary rehabilitation to meet these requirements.14 The aims of this study were to (1) compare completion rates of home-based versus centre-based pulmonary rehabilitation in people with COPD; (2) compare the clinical benefits of the two approaches; and (3) compare the costs of home-based and centre-based pulmonary rehabilitation. This paper reports on the clinical outcomes and direct programme costs. A full economic analysis will be published separately.
Methods
A randomised, controlled equivalence trial with assessor blinding was conducted at two tertiary hospitals in Melbourne, Australia. Ethical approval was granted and the trial protocol was published.14 Participants were recruited from pulmonary rehabilitation waiting lists between 21 October 2011 and 3 April 2014. Included participants were diagnosed with COPD; had a smoking history ≥10 pack years; had no exacerbations within 4 weeks or comorbidities which precluded exercise training; and had not undertaken pulmonary rehabilitation within 2 years. Written informed consent was obtained.
Participants were randomised to treatment groups (1:1) at the completion of their baseline assessment, using a computer generated sequence that was concealed using opaque envelopes. The sequence was generated by an individual unrelated to the study. Randomisation was stratified for site of recruitment and disease severity (FEV1<50% vs ≥50% predicted).3 All subsequent assessments were performed by an individual blinded to group allocation, who had no involvement in provision of either intervention. The success of assessor blinding was evaluated after the 12-month assessment by asking the assessor to nominate the group to which they thought the participant had been assigned.
Interventions
Participants in both groups received the core components of pulmonary rehabilitation, namely aerobic exercise training, resistance training and self-management education. All participants received a copy of Better Living with COPD: A Patient Guide, developed by Lung Foundation Australia to assist people with COPD to better understand their condition and actively participate in their care.15 Programme completion for both groups was defined as undertaking 70% of planned sessions, consistent with attendance criteria for pulmonary rehabilitation reported in a recent systematic review.16
Centre-based pulmonary rehabilitation was an 8-week, twice weekly outpatient group-based supervised programme, with individually prescribed exercise training and self-management education.17 At least 30 min of aerobic training was performed each session, including walking training (treadmill or corridor) and cycle training. Resistance exercises used functional activities such as stair climbing and sit-to-stand practice, as well as free weights for the upper limbs. Participants were encouraged to exercise at home on an additional three occasions each week. Self-management training included structured (lecture-based) and unstructured disease management education and goal setting, covering standard topics including management of exacerbations, understanding medications and ongoing participation in exercise.17
Home-based pulmonary rehabilitation commenced with one home visit by a physiotherapist to establish exercise goals, assess inhaler technique and supervise the first exercise session. At least 30 min of aerobic training was recommended for each session, using a modality accessible to the participant, which was usually walking. Participants recorded the distance walked using a pedometer (Omron Walking Style Pro). Resistance training included functional activities and equipment that were accessible in the home environment, including sit-to-stand from a dining chair, step ups on an internal or external step, and water bottles for upper limb weights. The home visit was followed by seven once-weekly structured telephone calls from a physiotherapist, using a motivational interviewing approach.18 Participants were informed that the aim of the exercise programme was to improve their strength and fitness. Structured telephone modules were used to explore and build motivation for exercise participation, then move towards commitment and action. Exercise goals were discussed and documented in a diary each week. Participants also recorded their unsupervised exercise sessions in the diary, including duration and distance walked, and the number and type of resistance exercises performed. Participants were provided with a menu of topics relevant to COPD self-care and encouraged to select a topic of relevance to them for discussion each week, providing opportunity for self-management education and goal setting. Management of acute exacerbations and ongoing participation in exercise were discussed at least once with all participants. Physiotherapists were trained in motivational interviewing and there were periodic checks on fidelity by an independent motivational interviewing practitioner. More details regarding the home-based programme are provided in the online supplementary material.
Supplemental material
Outcomes
Participants were evaluated at baseline, end of rehabilitation and 12 months later. The primary outcome was change in 6 min walk distance (6MWD), a measure of functional exercise capacity obtained from the 6 min walk test (6MWT). The test was performed on a 30 m corridor with standardised instructions and encouragement.19 Two tests were performed at each time point and the best distance used for analysis. Secondary outcomes were programme completion, modified Medical Research Council dyspnoea scale,20 HRQoL on the Chronic Respiratory Questionnaire (CRQ),21 Pulmonary Rehabilitation Adapted Index of Self-Efficacy (PRAISE),22 and Hospital Anxiety and Depression scale.23 Objective measurement of physical activity was undertaken in a subgroup of consecutively recruited participants using the Sensewear Armband24 from the time when additional funding became available until the end of the trial (see online supplementary material). Comorbidities were obtained from medical record review and documented using the COPD-specific COmorbidity TEst (COTE).25 The number of participants with a COTE index ≥4, indicating increased mortality risk, was recorded. Hospitalisation was assessed by medical record review at 12 months and verified by monthly telephone calls to participants. Detailed documentation of direct programme costs was undertaken (see online supplementary material).
Statistical analysis
Sample size calculations indicated that 144 participants were required to be 80% sure that the 95% CI excluded a difference in the change in 6MWD of more than the equivalence limit of 25 m, which was the minimal important difference (MID) established in our population,26 assuming an SD of 51 m.27 This also gave sufficient power to exclude a difference in the CRQ dyspnoea domain greater than the MID of 2.5 points.14 Anticipating 15% dropout, we randomised 166 participants.
Data were analysed using SPSS V.22.0 (IBM New York, USA). All data were analysed by intention-to-treat analysis. Differences between groups for change over time were analysed with linear mixed models. Models included treatment group, time, group × time interaction and a random effect for participants. The baseline value of the outcome variable was included as a covariate. As per Consolidated Standards of Reporting Trials (CONSORT) recommendations for equivalence trials, a per-protocol analysis was also conducted to minimise type 1 error.28 The relative risk of non-completion was determined. Time to hospital admission was evaluated using Kaplan-Meier curves and Cox proportional hazards modelling. α was set at 0.05. The trial was registered at clinicaltrials.gov (NCT01423227).
Results
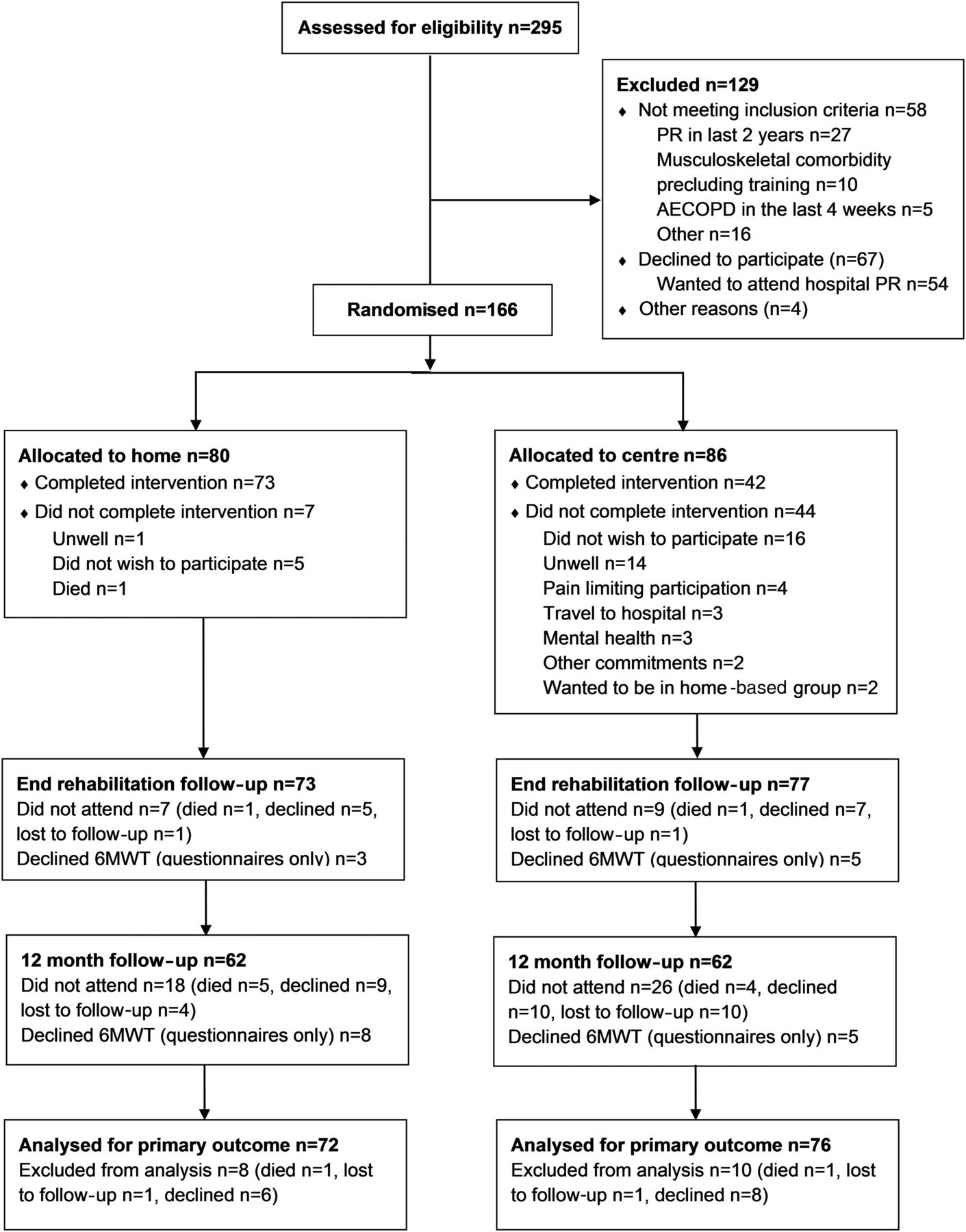
The flow of participants through the trial is in figure 1. Of eligible patients who did not consent (n=67), the majority (n=54) wanted to undertake rehabilitation in a centre-based programme. One hundred and sixty-six participants were randomised. At the end of the trial, data were available for the primary outcome in 90% of the home-based group and 88% of the centre-based group. Most participants had moderate or severe lung disease, and one in five had significant anxiety (table 1). Participants had a median of four comorbid conditions (IQR 3–6) and 21% had a COTE index ≥4.25 The comorbidities documented most commonly were hypertension (50%), hyperlipidaemia (44%), gastro-oesophageal reflux (40%), arthritis (30%) and depression (30%). Participants had low levels of physical activity at baseline (table 1).
Demographic characteristics of participants

Flow of participants through the trial. 6MWT, 6 min walk test; PR, pulmonary rehabilitation. AECOPD; acute exacerbation of chronic obstructive pulmonary disease.
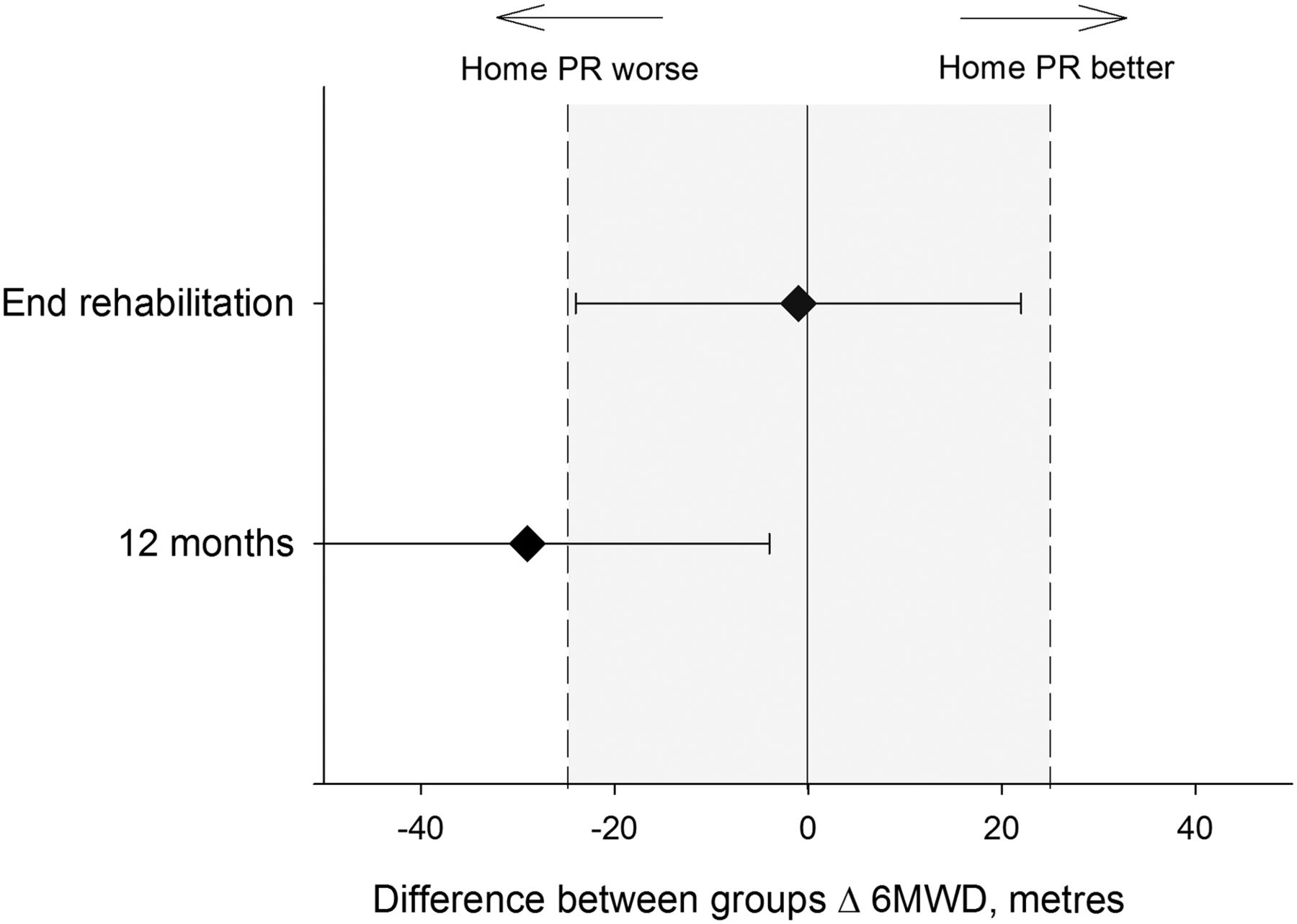
The intention-to-treat analysis showed improvements in 6MWD and HRQoL outcomes at the end of rehabilitation that generally returned to baseline by 12 months (table 2). There were no significant between-group differences. For the primary outcome of change in 6MWD at the end of rehabilitation, the lower end of the CI was above the lower bound of the equivalence limits (figure 2) indicating that home-based rehabilitation was not inferior to centre-based rehabilitation. The upper end of the CI was above the upper bound of the equivalence limits and superiority cannot be excluded. At 12 months, the lower end of the CI fell below the lower bound of the equivalence limit, so inferiority could not be excluded. For CRQ dyspnoea (figure 3) the results showed non-inferiority of the home-based programme at the end of rehabilitation and could not exclude superiority, while 12-month data demonstrated equivalence. The CRQ fatigue domain showed a similar pattern, while emotional function and mastery domains demonstrated equivalence at both time points, with CIs for the between-group difference that were less than the MID (table 2). There were no differences between groups for self-efficacy on PRAISE (table 2). The proportion of participants free from anxiety increased at 12 months (63% at baseline vs 69% at 12 months, p<0.001) with similar results for depression (74% vs 80%, p<0.001) and no differences between groups (see online supplementary figures S1 and S2).
Clinical outcomes—intention-to-treat analysis

Difference between groups for 6 min walk distance (6MWD) and equivalence limits. PR, pulmonary rehabilitation. Data are mean and 95% CI for difference between groups. Shaded area represents equivalence limits, which are ±minimal important difference.
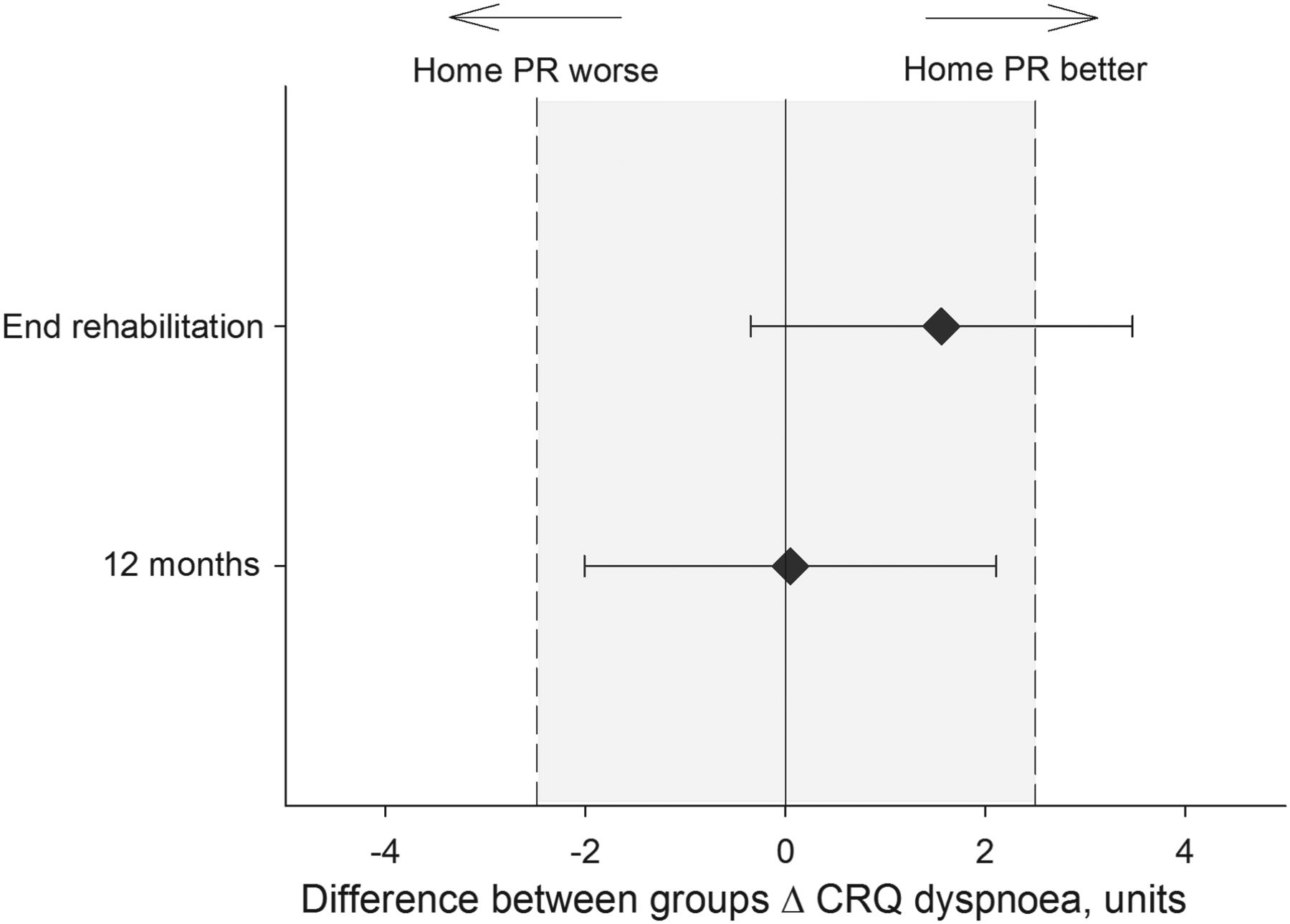
Difference between groups for Chronic Respiratory Disease Questionnaire (CRQ) dyspnoea domain and equivalence limits. PR, pulmonary rehabilitation. Data are mean and 95% CI for difference between groups. Shaded area represents equivalence limits, which are ±minimal important difference.
Physical activity data were available for n=29 and n=38 in home-based and centre-based groups, respectively. Across the whole sample there was a decrease in awake sedentary time following rehabilitation (mean −44 min, −75 to −13 min) which was not sustained at 12 months. Following rehabilitation the home-based group increased time spent in bouts of moderate to vigorous physical activity lasting at least 10 min (mean 16 min, 3–30 min), however there were no significant between-group differences for any physical activity variables (table 3).
Physical activity outcomes—intention-to-treat analysis
In the per-protocol analysis (including only those who completed the programmes) the centre-based group demonstrated larger improvements in exercise capacity and HRQoL than in the primary analyses, with no significant between-group differences (see online supplementary table S1). For change in 6MWD, the mean difference between groups at the end of rehabilitation was 1 m (95% CI −24 to 22), which demonstrates equivalence (figure 4). The change in 6MWD at 12 months favoured the centre-based group (−29 m, 95% CI −54 to 4) and inferiority of the home programme could not be excluded. The CRQ dyspnoea domain showed non-inferiority of the home-based programme at the end of rehabilitation and could not exclude superiority (0.95 units, −1.32 to 3.21) but inferiority could not be excluded at 12 months (−0.53 units, −3.00 to 1.94).

Difference between groups for 6 min walk distance (6MWD) and equivalence limits, per protocol analysis. PR, pulmonary rehabilitation. Data are mean and 95% CI for difference between groups. Shaded area represents equivalence limits, which are ±minimal important difference.
On average, participants in centre-based rehabilitation attended 8.3 of 16 scheduled sessions (range 0–16 sessions). Participants in the home-based group attended 7.4 of 8 scheduled sessions (range 0–8). No adverse events occurred in either group. Using the a priori criterion for programme completion, 42 participants (49%) completed the centre-based programme and 73 participants completed the home programme (91%), giving a relative risk of non-completion in the centre-based group of 1.91 (95% CI 1.52 to 2.41). In the home-based group, the average duration for the first telephone call was 27 min (SD 8 min) and for subsequent calls 20 min (SD 7 min). On average home participants recorded five unsupervised exercise sessions in their diaries each week (range 0–7 sessions) with an average walking duration of 32 (SD 7) minutes and four (SD 1) resistance exercises performed per session.
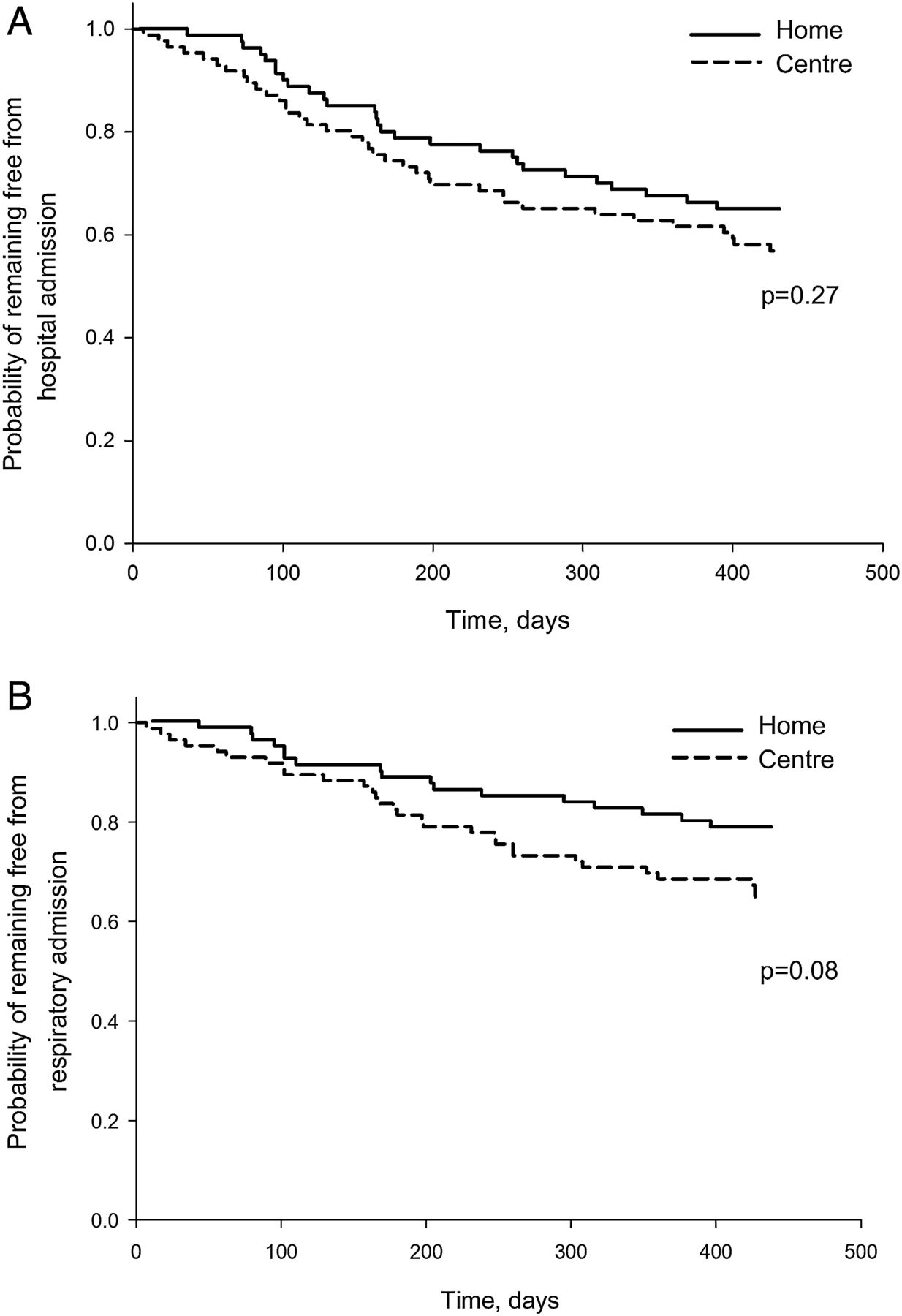
In the 12 months following rehabilitation 37 participants (43%) in the centre-based group were hospitalised compared with 28 participants (35%) in the home-based group (relative risk 0.81, p=0.29). There were no differences between groups in the number of hospitalisations or total hospital days (table 4). The home-based group tended to have fewer hospitalisations with a respiratory cause (17 vs 29, relative risk 0.63, p=0.07) and a longer time to first respiratory-related hospitalisation (figure 5). In a Cox proportional hazards model, programme completion appeared to mediate the effect of group on time to admission (HR for group 0.848, p=0.64; HR for programme completion 0.439, p=0.02; see online supplementary figure S3).
Hospitalisation in the 12 months following pulmonary rehabilitation (PR)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time to first hospitalisation for (A) all admissions and (B) admissions with a respiratory cause. p Value is for difference between groups on log-rank test.
At the end of the trial, the assessors correctly identified group allocation for 52% of participants (κ=0.26), demonstrating the success of blinding. Programme costs were $A298 per participant for home-based rehabilitation and $A312 for centre-based rehabilitation (₤156 and ₤164, respectively).
Discussion
This study shows that this highly structured home-based pulmonary rehabilitation model, using minimal resources and little direct supervision, results in short-term improvements in 6MWD and HRQoL that are equal to or greater than those seen in a centre-based programme. Equivalent quality of life outcomes were observed at 12 months following programme completion, although it was not possible to exclude inferiority for 6MWD at this time point. Gains in both groups were poorly maintained at 12 months.
Although the traditional centre-based model of pulmonary rehabilitation is highly effective in clinical trials,1 in clinical practice there is poor uptake and adherence. While some barriers to uptake reflect health system inefficiencies, inadequate commissioning and low referral rates, there are also patient-related barriers to uptake. These include travel and transport to the rehabilitation centre; illness and comorbidities; inconvenient timing; and disruption to established routines.7 Home-based programmes have the potential to overcome many of these limitations. We found that programme completion was significantly higher in those undertaking pulmonary rehabilitation at home. It must be acknowledged that it is easier to ‘attend’ a telephone call in one's home than a rehabilitation session at the hospital. However the removal of barriers to attendance was a major goal of our study and thus we consider this a strength of the model. On average home-based participants reported exercising five times each week, and the clinically relevant improvements in outcomes suggest that they may have engaged meaningfully in exercise training.
Using our a priori definition of completion (attending 70% of sessions), the completion rate in the centre-based group was poor (49%). Previous reports of non-completion in real world pulmonary rehabilitation programmes have ranged from 10% to 50%.7 A recent audit of pulmonary rehabilitation programmes in the UK reported that, on average, 39% of patients who attended their initial assessment did not complete the programme.29 The inability of participants to attend sufficient centre-based sessions to accrue benefits impacted on our intention-to-treat analysis of clinical outcomes, with improvements in exercise capacity in the centre-based group that were smaller than expected (table 2). This can be contrasted with the per-protocol analysis, which demonstrates clinically important gains in both exercise capacity and HRQoL in those who completed the programme, with a trend towards better 6MWD results in the centre-based group at 12 months (see online supplementary table S1). The low completion rate for the centre-based programme is a limitation to the study and our results may not be generalisable to settings where the completion rate is consistently higher. There are a number of possible reasons for the low completion rate in the centre-based group. Our inclusion criteria were broad, to ensure the external validity of our findings. Participants had a range of comorbid conditions (median 4 comorbidities, ranging up to 12 comorbidities), which are a well documented barrier to completion of centre-based programmes.7 We made great efforts to assess all available participants at the designated time points, regardless of whether they had been able to complete rehabilitation. As a result, our intention-to-treat results may more closely reflect the real world clinical outcomes of pulmonary rehabilitation than some previous trials. In a recent Cochrane review, over 40% of the studies contributing to meta-analysis for 6MWD were at risk of bias due to incomplete reporting of outcome data and lack of intention-to-treat analysis, suggesting that the magnitude of effect could be overestimated.1 The number of patients who did not consent because they wished to attend a centre-based programme should also be noted, as they may have been more likely to succeed under this model. Patient preferences and motivation regarding the site of pulmonary rehabilitation may impact on the outcomes that are achieved in different settings.
Participants in the home-based rehabilitation group demonstrated improvements in exercise capacity and HRQoL that met or exceeded the MID at programme completion. These results suggest that it is possible to deliver an effective rehabilitation dose using minimal resources and in a largely unsupervised programme. The home-based programme followed a highly structured format, with telephone calls conducted by respiratory physiotherapists who were trained in motivational interviewing techniques. Goal setting for exercise was an essential component of every telephone appointment and participants were also encouraged to set other health goals. There are other important differences to previous home-based pulmonary rehabilitation trials. We used equipment that was readily available in the home environment (eg, resistance exercises using water bottles), rather than bringing specialised exercise equipment into the home.12 Unlike previous studies11 our model incorporated only one home visit from a physiotherapist, which contributed to its low cost. All programme components were delivered at home, including exercise, self-management training and monitoring, which obviates the need for visits to a health facility.9 ,10 ,12 These are key factors that would need to be replicated for this home-based model to be implemented in clinical practice with both low cost and efficacy of outcomes.
Following rehabilitation there was a trend for home-based participants to have a longer time to hospital admission (p=0.08, figure 5). It appears that this effect was mediated by programme completion, with a significantly longer time to hospital admission for those who completed pulmonary rehabilitation, regardless of group allocation (see online supplementary figure S3). This suggests that the location of pulmonary rehabilitation may be less important than the delivery of an effective rehabilitation dose. We defined programme completion as attending 70% of sessions over 8 weeks and our results suggest that this could be sufficient to delay future hospitalisation, regardless of the rehabilitation model. This threshold requires further testing. Participants in both groups had varied reasons for failing to attend individual sessions including respiratory and non-respiratory illnesses, work commitments, medical appointments and family responsibilities. To achieve good attendance and outcomes will require flexible pulmonary rehabilitation models that acknowledge the complex demands on patient time, as well as the preferred site of care.
The failure to achieve long-term maintenance of benefits following pulmonary rehabilitation in either group is disappointing. This is consistent with previous studies17 and indicates that neither model achieved the necessary behavioural change for ongoing health maintenance. It has been suggested that programmes conducted in the home environment may better effect behaviour change through early integration into daily life.11 However our results indicate that this did not occur. It is possible that programmes of longer duration may be required to achieve such changes.30 We could not rule out inferiority of 6MWD in the home-based group at 12 months, although the CI falls within the currently accepted MID of 30 m19 and this difference may not be clinically important. The failure to achieve meaningful gains in physical activity in either group, which is also consistent with previous literature,31 supports a lack of integration of health-enhancing behaviours into daily life. Investigation of new methods to achieve sustainable behaviour change and maintenance of benefits following pulmonary rehabilitation remains a high priority.17
The strengths of this study include a rigorous methodology, powering for equivalence and successful blinding of outcome assessors. We recruited patients who are typical of those attending pulmonary rehabilitation programmes, with few exclusions. Our home-based model delivers all the essential components of pulmonary rehabilitation and does not require specialised equipment. Direct programme costs were low and similar to those for our centre-based programme. Our model could thus be widely generalised, although training in motivational interviewing will be required for most physiotherapists. We made every attempt to assess all participants at all time points, even if they were unwell or had not completed the programme. This may have affected the overall magnitude of benefit, but is reflective of the real world challenges of pulmonary rehabilitation.
Limitations include lack of objective measures of adherence to the home-based exercise programme, although given its unsupervised nature this was unavoidable. A limitation to the programme model is that the 6MWT, which was the primary trial outcome, could not be performed in the home environment32 and all participants had to attend the hospital for assessments. New tests of exercise capacity that can be accurately performed at home are urgently needed for home-based pulmonary rehabilitation to be effectively translated into clinical practice. The benefits achieved in this home-based pulmonary rehabilitation model may not be generalisable to all patient groups. Notably, we recruited participants who were medically stable; recent data suggest that home-based training may not be suitable for those who have had a recent exacerbation.33 Few of our participants were morbidly obese and only 5% were on long-term oxygen therapy. Whether our home-based pulmonary rehabilitation model is effective for these groups is unknown. We only included people with a diagnosis of COPD, so the effects of our home-based rehabilitation model in people with other chronic respiratory disorders remains to be established. Importantly, the programme completion rate in the centre-based group was low, which may not reflect completion rates in all real world centre-based services and may limit the generalisability of results.
In conclusion, a home-based pulmonary rehabilitation programme, using minimal resources and little direct supervision, delivers short-term improvements in functional exercise capacity and HRQoL that are at least equivalent to conventional centre-based pulmonary rehabilitation in people with COPD. Quality of life outcomes are also equivalent at 12 months following programme completion. Further research is required to develop strategies that maintain benefits at 12 months for both programmes. Home-based pulmonary rehabilitation may be useful to enhance access for the many patients with COPD who cannot engage in traditional programme models.
Acknowledgments
The authors thank all the trial participants for generously contributing their time to this study.
References
Footnotes
Contributors Conception and design: AEH, AM, CFM. Data acquisition: AEH, CJH, ALL, ATB, NSC, RM, CN, PO, AL, RG. Data analysis: AEH, AM, ATB, NSC, AL, ALL. Drafting and critically revising the manuscript, and final approval for publication: all authors.
Funding This study was funded by a Lung Foundation Australia / Boehringer Ingelheim COPD Research Fellowship and a National Health and Medical Research Council (Australia), project grant 1046353.
Competing interests None declared.
Ethics approval Alfred Hospital HREC, Austin Health HREC, La Trobe University HEC.
Provenance and peer review Not commissioned; externally peer reviewed.