Article Text

Abstract
BACKGROUND A survey of overnight oximetry was conducted to estimate the prevalence of nocturnal hypoxaemia in patients with cryptogenic fibrosing alveolitis and to establish whether nocturnal hypoxaemia is related to quality of life.
METHODS All patients with cryptogenic fibrosing alveolitis attending Nottingham City Hospital were invited to enter the study. Spirometric measurements and capillary blood gas tensions were obtained and overnight oxygen saturation was recorded at home. Quality of life was assessed using the Short Form-36, Chronic Respiratory Questionnaire, Hospital Anxiety Depression Scale, and Epworth Sleepiness Score questionnaires.
RESULTS Sixty seven eligible patients were identified and 50 agreed to enter the study, although two were subsequently excluded because they already used oxygen overnight. In the remaining 48 the mean (SD) overnight oxygen saturation (Sao 2) was 92.5 (4.3)% and the median number of dips greater than 4% per hour was 2.3 (interquartile range 1.5–5.3). Daytime oxygen level predicted mean overnight Sao 2 (1.94%/kPa, 95% CI 1.22 to 2.66, p<0.001) but percentage predicted forced vital capacity (FVC) did not (0.018%/% predicted FVC, 95% CI –0.04 to 0.08, p=0.5). Nocturnal hypoxaemia was associated with decreased energy levels and impaired daytime social and physical functioning, and these effects were independent of FVC.
CONCLUSIONS Nocturnal hypoxaemia is common in patients with cryptogenic fibrosing alveolitis and may have an impact on health related quality of life.
- cryptogenic fibrosing alveolitis
- sleep
- health related quality of life
Statistics from Altmetric.com
The outlook for patients with cryptogenic fibrosing alveolitis is poor; the symptoms of breathlessness and cough are usually progressive and about 50% of patients die within 3 years of diagnosis.1 The response to currently recommended treatments2 in terms of survival is disappointing.3-5 There is therefore a need to consider the use of treatments designed primarily to palliate the symptoms of the disease. The short term use of oxygen following exertion has been shown to improve symptoms of breathlessness6 ,7 and some patients have oxygen cylinders at home for this purpose. The use of long term oxygen therapy is currently only recommended on a short term basis for patients awaiting lung transplantation or when the resting daytime oxygen level is less than 8 kPa.7 Two small studies have shown that nocturnal hypoxaemia is common in the presence of severe lung fibrosis.8 ,9 Since nocturnal hypoxaemia may cause daytime symptoms,10 ,11 nocturnal oxygen supplementation is a potential palliative treatment for patients with cryptogenic fibrosing alveolitis. As a prelude to an intervention study we have therefore estimated the prevalence of nocturnal hypoxaemia in patients with cryptogenic fibrosing alveolitis attending one hospital in Nottingham, and investigated whether nocturnal hypoxaemia has an impact on quality of life.
Methods
All patients with a diagnosis of cryptogenic fibrosing alveolitis attending Nottingham City Hospital were eligible to enter the study. Since only a few patients in the UK have an open lung biopsy12 we used our previous clinical criteria to define the diagnosis13 but, in addition, in this study patients with connective tissue disease were also included. Patients were identified using a combination of lung function records, hospital discharge codes, and our local cryptogenic fibrosing alveolitis database.
Following consent from the relevant general practitioner, we wrote to patients inviting them to take part in the study. Patients who agreed attended Nottingham City Hospital for one visit and, following a full explanation of the study, gave written consent. They attended the lung function laboratory for spirometric tests (dry bellows spirometer, Vitalograph Ltd, Bucks, UK) and, after 20 minutes at rest, capillary blood gas analysis and to complete health status questionnaires. The questionnaires used were the Short Form 36 (SF-36)14 to provide generic data on health status, the Epworth Sleepiness Score (EPSS)15 to provide a measure of daytime sleepiness, a self-completion version of the Chronic Respiratory Questionnaire (CRQ-SR)16 ,17 to provide symptoms of respiratory disease, and the Hospital Anxiety Depression Scale (HADS)18 to provide a measure of anxiety and depression. In order to confirm the relevance of these questionnaires to patients with cryptogenic fibrosing alveolitis we carried out a brief qualitative study using a semi-structured interview to collect data from two patients with moderately severe disease. All questionnaires were administered by one of us (MC) who was blind to the lung function results. Nocturnal oxygen saturation (Sao 2) was measured using a Minolta Pulsox 3i wrist oximeter which was worn by patients overnight at home and returned to us the next day. Data from the oximeters were downloaded onto an IBM compatible personal computer and analysed using software supplied by Minolta. If the probe attached time was less than 5 hours the test was deemed to be unsatisfactory and was repeated.
An initial descriptive analysis was performed to compare continuous variables using the unpaired t test with prior log transformation of non-normally distributed variables. The main outcome variables were mean overnight Sao 2and the proportion of study time spent with an Sao 2 of less than 90%. Linear regression was used to establish the association between mean overnight Sao 2 and both lung function measurements and health related quality of life measures, adjusting for the effects of age and sex. Nearly all subjects spent at least some of the night with an Sao 2 of less than 90%. When these data were examined graphically it was found that, for about 50% of the subjects, this proportion was short at less than 2%. We therefore arbitrarily defined the sleep study as abnormal if more than 2% of the recording was spent at an Sao 2 of less than 90% and used logistic regression to establish the association between the presence of an abnormal sleep study defined in this way and health related quality of life. Where consistent associations were found between health related quality of life outcomes and both measures of nocturnal hypoxaemia, these analyses were adjusted further for percentage predicted forced vital capacity (FVC) and were also repeated following exclusion of patients with a daytime oxygen level of less than 8 kPa.
The study was reviewed and approved by the Nottingham City Hospital ethics committee.
Results
Sixty seven eligible patients were identified of whom 50 agreed to take part in the study. Of the remaining 17, 15 declined to take part (in five cases because they did not feel well enough) and we were unable to contact two. Of the 50 who did take part, 33 (66%) were men, the mean (SD) age was 67.7 (8.7) years, and seven (14%) had coexisting connective tissue disease. In each case the connective tissue disease was rheumatoid arthritis and these patients tended to be younger than patients with “lone” cryptogenic fibrosing alveolitis (61.6v 68.9 years, p=0.04). The median time between date of diagnosis and recruitment was 2.1 years (interquartile range 1.0–4.4 years). A high resolution CT scan was used to confirm the diagnosis in 40 patients (80%). Subjects who did not have a CT scan tended to be those who were diagnosed longer ago (median time from diagnosis 8.0 v 1.7 years, p=0.003) and those who were older (mean age 74.7 v 66.3 years, p=0.009). The mean (SD) percentage predicted forced vital capacity (FVC) was 80.9 (25.0)% and mean daytime capillary oxygen concentration was 9.3 (1.6) kPa.
DAYTIME PHYSIOLOGICAL PREDICTORS OF NOCTURNAL HYPOXAEMIA
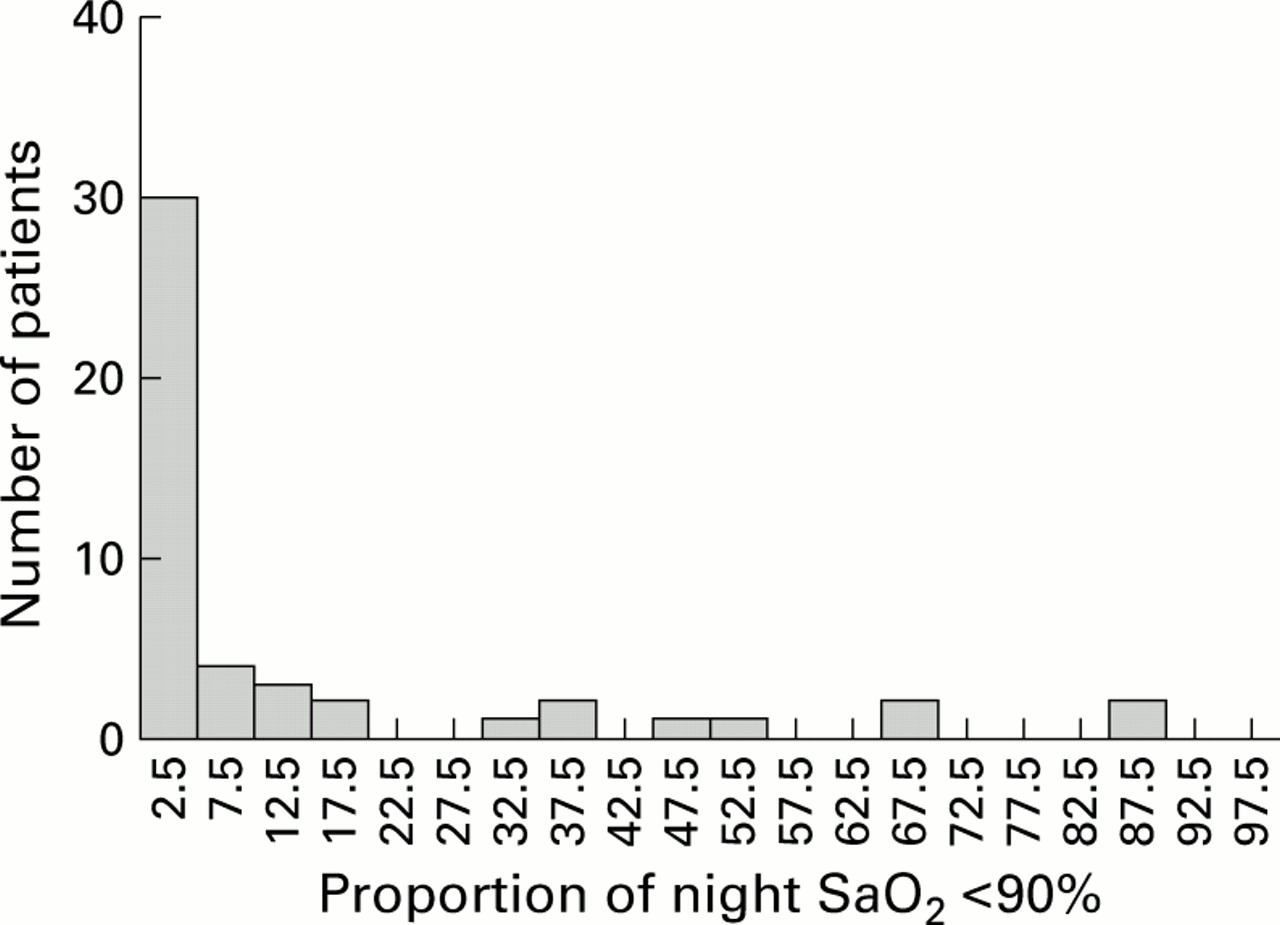
Two patients were already using oxygen at night and so were excluded from overnight oximetry measurements. In the remaining 48 none had a medical history suggestive of obstructive sleep apnoea. The mean duration of sleep recording was 7 hours and 53 minutes (range 5 hours 52 minutes to 10 hours 2 minutes) and the mean (SD) overnight Sao 2 was 92.5 (4.3)% (fig 1). Every subject had at least two dips in Sao 2 of greater than 4%, and the median number of dips per hour was 2.3 (interquartile range 1.5–5.3). A plot of the proportion of time spent with an Sao 2 of less than 90% (fig 2) showed that just under half of the patients (n=21) spent more than 2% of the night with an Sao 2 of less than 90%. Only four patients spent no time overnight with an Sao 2 of less than 90%. Age, sex, and percentage predicted FVC were not predictors of mean overnight Sao 2 or the proportion of time spent with an Sao 2 of less than 90%, but resting daytime capillary oxygen level strongly predicted both (table1).
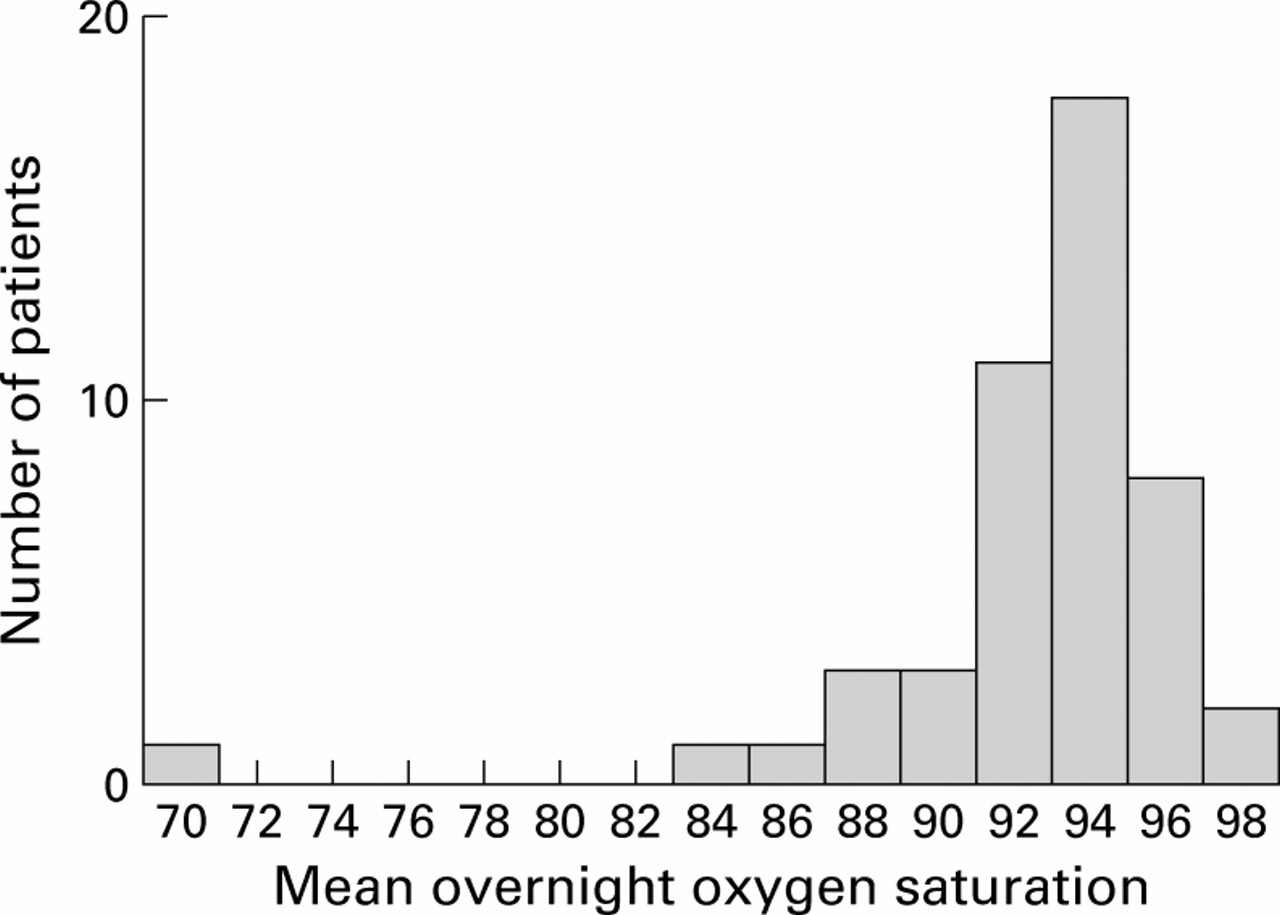
Distribution of mean overnight oxygen saturation values.
{kind=link}
{kind=link}
Distribution of proportion of time spent with an Sao 2 of <90%.
Age, sex, focred vital capacity (FVC), and daytime oxygen level (Sao 2) as predictors of nocturnal hypoxaemia
RELATION BETWEEN PERCENTAGE PREDICTED FVC AND HEALTH RELATED QUALITY OF LIFE
Within the CRQ-SR questionnaire domains we found evidence of a strong association between percentage predicted FVC and mastery and a weaker association with dyspnoea (table 2). For the SF-36 the strongest association was found between health perception and percentage predicted FVC, although there was also some evidence of an association with the physical functioning, mental health, and energy domains. For the HADS questionnaire there was some evidence of an association with depression but not anxiety. There was no association between the Epworth sleepiness score and percentage predicted FVC.
Relation of health related quality of life to percentage predicted forced vital capacity (FVC)
RELATION BETWEEN NOCTURNAL HYPOXAEMIA AND HEALTH RELATED QUALITY OF LIFE
Within the domains of the CRQ-SR there was some evidence of an association between mastery and mean overnight Sao 2 but not with the presence of an abnormal sleep study as defined by the proportion of time spent with an Sao 2 of less than 90% (table 3). Within the SF-36 scores the physical functioning, social functioning, and energy domains were associated with lower overnight Sao 2 and an abnormal sleep study. The strongest associations were with the energy domain, and these were essentially unchanged by adjusting for percentage predicted FVC (adjusted regression coefficient 0.41% per questionnaire score, 95% CI 0.12 to 0.71, adjusted odds ratio 0.77, 95% CI 0.64 to 0.93) and, although attenuated, remained when the analysis was limited to patients with a daytime Sao 2 of more than 8 kPa (regression coefficient 0.26% per questionnaire score, 95% CI 0.03 to 0.50, odds ratio 0.80, 95% CI 0.64 to 1.01). The effect of adjusting for percentage predicted FVC and restricting the analysis to patients with a daytime oxygen of more than 8 kPa was similar for the physical functioning and social functioning domains. There was no consistent evidence for an association between nocturnal hypoxaemia and the anxiety or depression domains of the HADS questionnaire. The presence of an abnormal sleep study was related to the Epworth sleepiness score but there was no association with mean overnight Sao 2.
Relation between health related quality of life and nocturnal hypoxaemia
Discussion
The results of this study show that nocturnal hypoxaemia is common in patients with cryptogenic fibrosing alveolitis attending hospitals in the UK. The best physiological predictor of nocturnal hypoxaemia was resting daytime oxygen level while, in contrast, FVC was a poor predictor. On the basis of the questionnaires used, nocturnal hypoxaemia appears to be associated with a reduction in energy levels and impairment of physical and social functioning, and these effects are independent of FVC.
In this study the aim was to recruit patients who were representative of those with cryptogenic fibrosing alveolitis being cared for by chest and general physicians in the UK. For this reason we tried to include all patients, including those with coexisting connective tissue disease, and chose to study nocturnal hypoxaemia at home using simple wrist pulse oximeters which are easy to use, cheap, and convenient for patients. Patients with coexisting connective tissue disease may have changes in health related quality of life outcomes because of symptoms resulting from the comorbid illness. However, comorbidity is also common in patients with “lone” cryptogenic fibrosing alveolitis—particularly heart disease19 ,20 and lung cancer19 ,21 ,22—so we decided not to exclude patients with additional illnesses. In fact, the results of the study were similar when the analysis was restricted to patients with “lone” cryptogenic fibrosing alveolitis. The use of additional sleep studies on consecutive nights would have been beneficial in giving an assessment of night-to-night variation in nocturnal hypoxia but, in order to keep the study simple for patients and more relevant to clinical practice, we did not do this.
Since our study is cross sectional it includes only prevalent cases so patients with a better prognosis will tend to be over-represented1 as those who die rapidly are not under long term follow up. Therefore, although we tried to include patients with the full spectrum of disease severity, our sample is likely to be made up of patients with a better prognosis than a cohort of newly diagnosed cases. This bias is unlikely to alter the physiological finding that nocturnal hypoxaemia is common in patients with cryptogenic fibrosing alveolitis and that daytime oxygen concentration is the best predictor of nocturnal hypoxaemia, but it may lead to some dilution of the associations between physiological measures and health related quality of life scores because, with time, patients will reset their goals and develop coping mechanisms.
The strong association between daytime oxygen levels and nocturnal hypoxaemia is not surprising. In a study of 11 patients with severe interstitial lung disease9 the five patients with a daytime Sao 2 of less than 90% had a significantly lower overnight Sao 2 than the six with a daytime Sao 2 of more than 90%. Furthermore, previous studies in patients with chronic obstructive pulmonary disease (COPD) have shown that mean awake Sao 2 is a strong predictor of both mean and lowest overnight Sao 2.10 ,23 In patients with COPD who have nocturnal hypoxaemia the main mechanism appears to be hypoventilation, particularly during periods of rapid eye movement sleep (REM)10 and, as for our patients with cryptogenic fibrosing alveolitis, daytime spirometric parameters are poor predictors of nocturnal Sao 2.
The measures of health related quality of life suggest that nocturnal hypoxaemia leads to decreased daytime energy levels and impaired social and physical functioning, and that these effects are independent of FVC. Although FVC was associated with the dyspnoea domain of the CRQ-SR, neither were associated with nocturnal hypoxaemia. The most obvious explanation for these findings is that nocturnal hypoxaemia disturbs the sleep patterns of patients with cryptogenic fibrosing alveolitis and that this has an impact on daytime health related quality of life. One previous study has shown that patients with severe interstitial lung disease have fragmented sleep and spend more time in stage 1 sleep and less time in REM sleep.9 The alternative explanation is that the associations we found are due to disease severity in general, and that nocturnal hypoxaemia is merely another marker of disease severity not adequately captured by FVC. Ultimately, this issue can only be resolved by studying the efficacy of nocturnal oxygen supplementation on health related quality of life in patients with cryptogenic fibrosing alveolitis. Our finding of associations between nocturnal hypoxaemia and health related quality of life for patients with a daytime oxygen level of more than 8 kPa—that is, patients for whom long term oxygen therapy is not currently recommended7—suggests that such a trial should include the full spectrum of patients with cryptogenic fibrosing alveolitis.
In summary, nocturnal hypoxaemia is a common problem in patients with cryptogenic fibrosing alveolitis and is associated with decreased daytime energy levels and impaired social and physical functioning independent of the level of FVC. Daytime oxygen level is the best predictor of nocturnal hypoxaemia and FVC is a poor predictor. Overnight oxygen supplementation is a potential palliative treatment for patients with cryptogenic fibrosing alveolitis and should be assessed in a randomised clinical trial
Acknowledgments
The authors would like to thank lung function technicians Sue Hazard, Philomena Dennis, Julie Christian, Rachel Anthony and Karen Lakin, the City Hospital Chaplaincy and, in particular, Martin Kerry for allowing them to use a quiet room for the study.
References
Footnotes
Funding: Trent National Health Service Research and Development Project Grant.