Article Text

Abstract
Background: A study was undertaken to determine the relation between urinary cadmium levels and lung function in a nationally representative cohort of current, former, and never smokers in the US. Urinary cadmium levels reflect the total body burden of cadmium.
Methods: The following data from the Third National Health and Nutrition Examination Survey were analysed: urinary cadmium (adjusted for urinary creatinine), lung function, sex, race/ethnicity, age, education level, job category, body mass index, serum cotinine level, and smoking history. Linear regression models were developed to predict lung function using urinary cadmium as the main predictor, adjusting for other covariates and stratified by smoking status.
Results: Data were available on 16 024 adults. Current smokers had higher mean (SE) urinary cadmium/creatinine levels (0.46 (0.01) μg/g) than former (0.32 (0.01) μg/g) or never smokers (0.23 (0.01) μg/g). Higher levels of urinary cadmium were associated with significantly lower forced expiratory volumes in 1 second (FEV1) in current (−2.06%, 95% confidence interval (CI) –2.86 to −1.26 per 1 log increase in urinary cadmium) and former smokers (−1.95%, 95% CI –2.87 to −1.03) but not in never smokers (−0.18%, 95% CI –0.60 to 0.24). Similar results were obtained for forced vital capacity (FVC) and FEV1/FVC.
Conclusions: Cadmium, which is known to cause emphysema in occupational settings, may also be important in the development of tobacco related lung disease.
- cadmium
- smoking
- lung function
- chronic obstructive pulmonary disease
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is an important cause of morbidity and mortality throughout the world.1,2 A large proportion of people with impaired lung function have never been diagnosed with any lung disease,3 suggesting that the true impact of COPD may be greatly underestimated.
Current understanding of the risk factors and pathogenesis of COPD remains incomplete. While smoking is the biggest known risk factor for developing COPD, not all smokers develop the disease.4,5 Other known risk factors for COPD—including occupational exposure, air pollution, airway hyperresponsiveness, asthma, and genetic disease such as α1-antitrypsin deficiency—are also important.6–9 The mechanisms that make certain smokers more susceptible to developing COPD remain a subject of ongoing investigation.10–12
One toxicant in tobacco smoke that may be important in the development of COPD is cadmium. Cadmium has been linked to emphysema in occupationally exposed workers13,14 and has been shown to induce emphysema in laboratory animals.15 A recent review, however, stated that it seems “improbable that smoking induced emphysema could be attributed to cadmium”.16
We examined the relationship between smoking, urinary cadmium levels, and pulmonary function in a nationally representative population using data from the National Health and Nutrition Examination Survey, 1988–1994 (NHANES III).
METHODS
Study population
NHANES III was conducted from 1988 to 1994 by the National Center for Health Statistics of the Centers for Disease Control and Prevention, Atlanta, Georgia.17 A stratified multistage clustered probability design was used to select a representative sample of the US population, yielding results that can be extrapolated to the non-institutionalised civilian US population. Study participants completed extensive questionnaires in the household and a comprehensive physical examination, including pulmonary function testing either in the household or at a specially equipped mobile examination centre. A total of 81 sites was included in the final sample. The study was approved by Institutional Review Board of the National Center for Health Statistics.
Subjects and demographic characteristics
Our study sample was limited to adult participants aged 17 years and older in NHANES III (1988–94) in whom pulmonary function tests were performed, urine cadmium and creatinine samples were taken, and who had data on sex, race/ethnicity, smoking status, occupation, and body mass index. Of the 20 050 adult survey participants in NHANES III, 1888 did not have the examination, 1467 did not perform pulmonary function tests, urine samples were not obtained from 638, and in 33 there were missing data on other variables. After the exclusions, data were available from 16 024 subjects for the main analysis. Excluded subjects were older and more likely to have fewer than 12 years of education than included subjects (p<0.05 for both), but were similar in race/ethnicity, sex, and smoking status.
Variable definitions
The race of the participants was classified as white, black, Mexican-American or other and was determined by self-report on the questionnaire. Other demographic covariates included were sex, education (⩽11 years, 12 years, or ⩾13 years), and age. Subjects were stratified into six age strata; 17–24, 25–44, 45–64, 65–74, 75–84, and 85+ years. The body mass index was calculated by dividing the weight in kg by the square of the height in metres and classified as follows: <18.5, ⩾18.5–24, 25–29, and ⩾30 kg/m2.18 Subjects were defined as current smokers, former smokers, pipe or cigar smokers, or never smokers based on their responses to a series of questions. Current pipe or cigar smokers were considered “current smokers”. Subjects had to have smoked at least 100 cigarettes, 50 cigars, or 3 ounces of pipe tobacco to qualify as a former or current smoker. Data from the reported smoking history were used to calculate pack years of cigarettes smoked and, for former smokers, years since they stopped smoking. Subjects were asked what occupation they had worked in for the longest period of time and this was classified into one of six categories: agriculture, mining/manufacturing, transportation, service, other/unemployed, and retail. Subjects reported their average monthly intake of dairy products, vegetables, fruits, meats, and grains.
Pulmonary function data
Using either a dry rolling seal spirometer in the mobile examination centre (98.5% of included subjects) or a portable spirometer in the home, spirometric tests were conducted on the participating subjects. Procedures for testing were based on the 1987 American Thoracic Society recommendations.19 In order to obtain curves acceptable according to the protocol, subjects performed 5–8 forced expirations. They were excluded from the analysis if they either did not perform spirometric tests or had results that were not reliable. Values used in this analysis included forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and the FEV1/FVC ratio. Predicted values of FEV1 and FVC were determined using previously published prediction equations.20 The sex specific model for white participants was applied to people of “other” race. Criteria from the Global Initiative on Obstructive Lung Disease (GOLD) were used to define subjects with stage 2 or worse COPD (FEV1/FVC <0.70 and FEV1 <80% predicted).21
Urine samples
Participants provided urine samples in either the home or mobile examination centre. Urine cadmium and creatinine measurements were included in the analysis. Cadmium levels were measured by graphite furnace atomic absorption spectrophotometry at the Centers for Disease Control and Prevention laboratory.22 The limit of detection was 0.03 μg/l; subjects with levels below the limit of detection were assigned a level of 0.01 μg/l. Cadmium levels were below the level of detection in 6.8% of the urine samples. Cadmium levels were adjusted for the urine creatinine concentration23 and the natural logarithm of these levels was used in the analyses because of a skewed distribution.
Cotinine levels
Serum cotinine levels were determined using high performance liquid chromatography atmospheric pressure chemical ionisation tandem mass spectrometry as described elsewhere.24 The study population was stratified into five groups on the basis of cotinine levels: below the limit of detection of 0.050 ng/ml (no smoke exposure), 0.050–0.29 ng/ml (low smoke exposure), 0.29–14.9 ng/ml (high smoke exposure), 15–99 ng/ml (light smoker), and ⩾100 ng/ml (moderate/heavy smoker).
Analysis of data
All estimates were calculated using the sampling weight to represent adults aged 17 years and older in the US. The purpose of these sampling weights was to adjust for unequal probabilities of selection and to account for non-response. All percentages shown are weighted and age adjusted to the distribution of participants in the final analytical sample.
Multivariate linear regression models were developed to describe the predictors of the urine cadmium/creatinine levels and to define the relation between measures of lung function and the urine cadmium/creatinine level, stratified by smoking status. We also used logistic regression models to predict subjects who met GOLD stage 2 or higher criteria for COPD (compared with subjects with normal lung function). Multivariate models adjusted for age, sex, race, body mass index, education level, cotinine level, pack years of cigarettes, and years since smoking cessation (for former smokers). Models were evaluated for interaction. SAS and SUDAAN, a program that adjusts for the complex sample design when calculating variance estimates, were used for the analysis.25,26
RESULTS
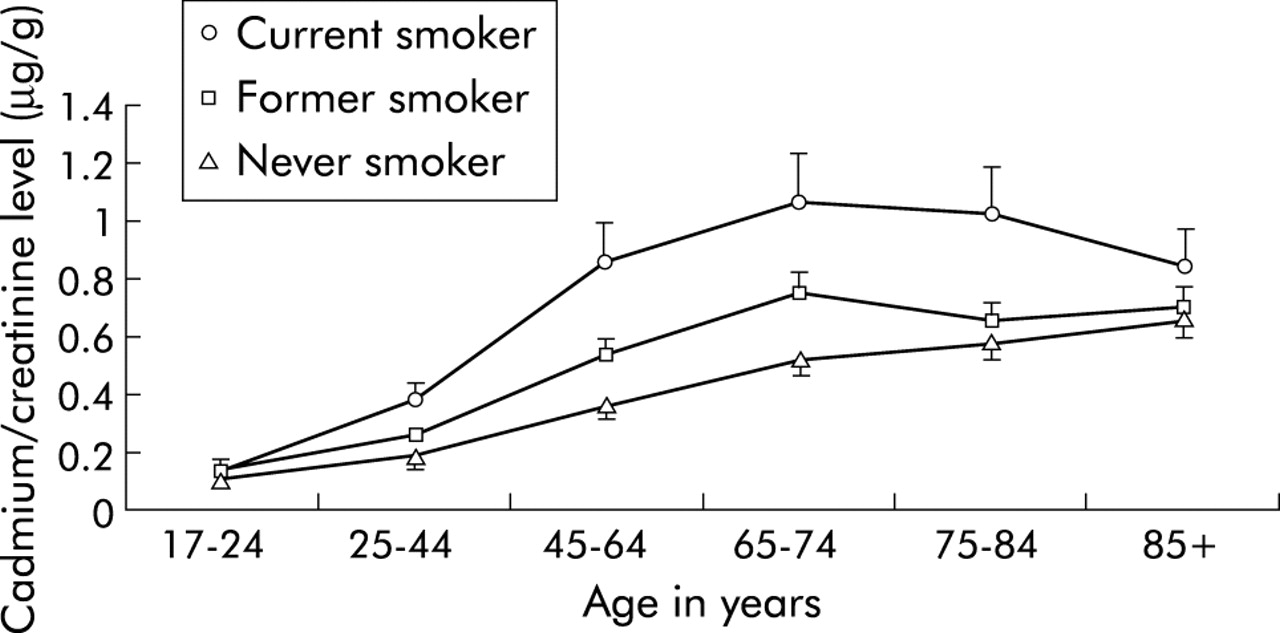
Creatinine adjusted urine cadmium levels were higher in smokers and increased with age (table 1, fig 1). Linear regression models for log urine cadmium/creatinine showed that higher age, black or Mexican-American race/ethnicity, and female sex were associated with higher levels in all three smoking categories (table 2). Indicators of smoking status (pack years for current smokers, years since smoking cessation for former smokers, and cotinine levels for all three categories) were also significant predictors of the urine cadmium/creatinine level (table 2). Working in the mining/manufacturing or transportation fields was associated with higher levels in current and former smokers (table 2). These levels also varied dramatically among smokers with similar smoking histories. For example, among 71 current smokers aged 50–60 years with a 40–50 pack year history the median urine cadmium/creatinine level was 1.3 μg/g with 10% having levels >2.2 μg/g and 10% having levels <0.6 μg/g.
Study population stratified by covariates with the weighted proportion in each stratum, the age adjusted geometric mean urine cadmium/creatinine level, and age adjusted forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio for each stratum
Results of regression models for log urine cadmium/creatinine adjusted for age, race/ethnicity, sex, education, job category, body mass index, years ago quit smoking (for former smokers), pack years of cigarettes, cotinine level, and daily intake of dairy products, fruits, vegetables, meats and grains

Geometric mean creatinine adjusted urine cadmium levels stratified by smoking status. From the Third National Health and Nutrition Examination Survey, 1988–94.
The age adjusted measures of lung function (percentage predicted FEV1, percentage predicted FVC, and FEV1/FVC) also varied with covariates. As expected, current smokers had a lower percentage predicted FEV1 (91.4 (0.4) v 97.8 (0.4)) and FEV1/FVC ratio (76.5 (0.2) v 80.7 (0.2)) than never smokers (table 1).
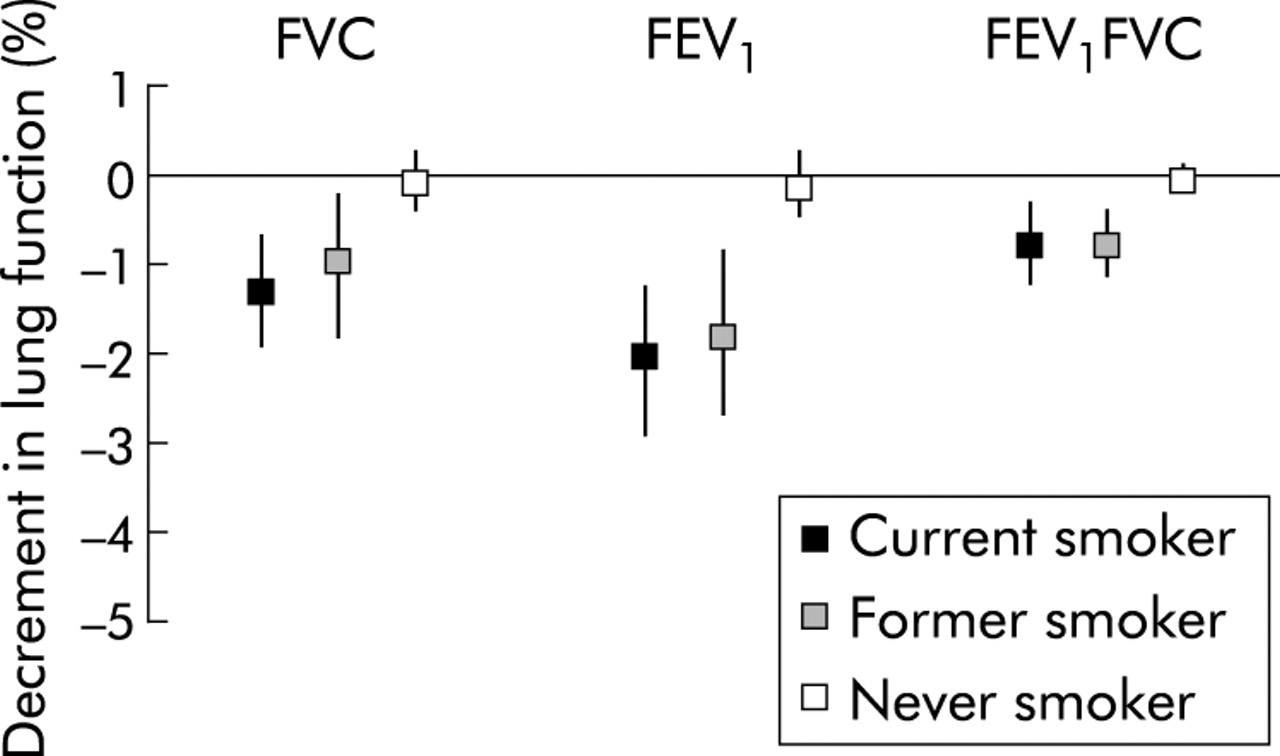
Among current and former smokers, higher levels of urinary cadmium were associated with significantly lower values of FEV1, FVC, and FEV1/FVC ratio in models that adjusted for age, race, sex, education level, job category, body mass index, cotinine level, pack years of smoking, and years since regular smoking (for former smokers) (fig 2 and supplementary tables S1–3 shown on the Thorax website at www.thoraxjnl.com/supplemental). For example, among the 50–60 year old current smokers with a smoking history of 40–50 pack years, the mean decrease in FEV1 in subjects in the 90th percentile of urine cadmium level compared with those in the 10th percentile was 3.2%. There was no significant relation between urine cadmium levels and lung function among never smokers (fig 2 and supplementary tables S1–3)
{kind=link}
{kind=link}
Decrease in lung function for a one log increase in urine cadmium/creatinine level for forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and FEV1FVC ratio, stratified by smoking status. Results from linear regression models adjusted for age, race, sex, education level, job category, body mass index, pack years of smoking, cotinine level, and years since regular cigarette smoking. From the Third National Health and Nutrition Examination Survey, 1988–1994.
Logistic regression models showed that, after adjusting for covariates, a higher urine cadmium/creatinine level was associated with GOLD stage 2 or higher COPD in current smokers (odds ratio (OR) 2.29, 95% confidence interval (CI) 1.67 to 3.15) and former smokers (OR 1.90, 95% CI 1.38 to 2.63) but not in never smokers (OR 1.25, 95% CI 0.98 to 1.60) (table S4 available on the Thorax website at www.thoraxjnl.com/supplemental).
DISCUSSION
In a representative US population higher levels of urinary cadmium were found to be significant predictors of lower FVC, FEV1, and FEV1/FVC in current and former smokers but not in never smokers. In addition, variability in urine cadmium levels was found among current smokers. It is not clear whether this finding is related to the dose of cadmium to which smokers are exposed or to variability in the uptake and metabolism of cadmium in smokers. It is possible that the variability in cadmium levels in smokers is related to the intensity of smoking—that is, smokers with higher cadmium levels extract more tar and nicotine out of each cigarette than smokers with lower levels. It is also possible that the variability in lung function in smokers is similarly related to variability in smoking intensity, and that cadmium levels are just a long term marker of tobacco dose.
Cadmium intake in humans is either through ingestion or inhalation, with the major source of exposure in never smokers being ingestion and in smokers being inhalation.27 The differences we observed—with significant decreases in lung function occurring only in current and former smokers—may be because urinary cadmium levels reflect lung cadmium better in smokers than in never smokers.28
One cigarette contains about 2 μg cadmium, 2–10% of which is transferred to primary cigarette smoke.29 Data from the Massachusetts Benchmark Study showed considerable variation in the cadmium content of mainstream smoke from 27 brands of tested cigarettes, ranging from 31 to 222 ng/cigarette with a median level of 137 ng/cigarette.30 Smokers have previously been shown to have higher blood and urinary cadmium levels22,31,32 as well as higher lung tissue cadmium levels.33–35 Urinary cadmium levels have been found to correlate closely with lung cadmium levels in current and former smokers.28 Urinary levels of cadmium rise with renal dysfunction36,37 and need to be adjusted accordingly. Adjustment of urinary cadmium to creatinine reduces variability between individuals.23 Cadmium levels in the lung and urine remain raised for many years after smoking cessation.22,34
Cadmium damages pulmonary cells in vitro, affecting several levels of function including repair of DNA,38 cellular enzyme activity and membrane structure,39 and α1-antitrypsin inhibitory capacity.40 Cadmium has been shown to be associated with the development of emphysema in occupationally exposed cohorts,13 although its role in the development of lung cancer is less clear.41–43
Bjorkman et al found that up to 10% of the variability in cadmium concentrations was related to genetic factors.44 The expression and regulation of metallothionein proteins, which absorb and sequester cadmium and protect against cadmium toxicity,45,46 may be part of the mechanism of genetic variation observed in cadmium uptake and metabolism.
This study is subject to some limitations. Because it is cross sectional in design, we cannot say that higher cadmium levels led to lower lung function. Smoking status and smoking histories were self-reported, with the potential for misclassification of these critically important measures. Occupational or non-vocational exposures to cadmium (such as alloy making, jewellery making, etc) were not specifically asked about.
In conclusion, we found that urinary cadmium levels, which reflect the total body burden of cadmium, are inversely associated with lung function in current and former smokers but not in never smokers. Future research should examine whether lung cadmium levels are predictors of lung function decline, the extent to which variation in cadmium levels among smokers reflects cadmium dose versus cadmium uptake and metabolism, and whether increased levels of cadmium in the lung are amenable to intervention.
REFERENCES
Supplementary materials
Web-only Tables
The tables are available as downloadable PDFs (printer friendly files).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [View PDF] - Table S1 Results of regression models for FEV1/FVC adjusted for log urine cadmium/creatinine, age, race/ethnicity, sex, education, job category, body mass index, years ago quit smoking (for former smokers), pack years of cigarettes, and cotinine level. From the Third National Health and Nutrition Examination Survey, 1988�94
- [View PDF] - Table S2 Results of regression models for FEV1 adjusted for log urine cadmium/creatinine, age, race/ethnicity, sex, education, job category, body mass index, years ago quit smoking (for former smokers), pack years of cigarettes, and cotinine level. From the Third National Health and Nutrition Examination Survey, 1988�94
- [View PDF] - Table S3 Results of regression models for FVC adjusted for log urine cadmium/creatinine, age, race/ethnicity, sex, education, job category, body mass index, years ago quit smoking (for former smokers), pack years of cigarettes, and cotinine level. From the Third National Health and Nutrition Examination Survey, 1988�94
- [View PDF] - Table S4 Results of logistic regression models for GOLD stage 2 or worse COPD* adjusted for log urine cadmium/creatinine, age, race/ethnicity, sex, education, job category, body mass index, years ago quit smoking (for former smokers), pack years of cigarettes, and cotinine level. From the Third National Health and Nutrition Examination Survey, 1988�94
Linked Articles
- airwaves