Article Text

Abstract
Background Orthopnoea and paroxysmal nocturnal dyspnoea are common entities regularly confronting thoracic physicians, particularly those with an interest in sleep medicine or non-invasive ventilatory support. One major cause is heart failure (HF), usually associated with abnormal lung function tests, and either obstructive or central sleep apnoea with Cheyne–Stokes respiration (CSA–CSR). Whereas obstructive apnoea is considered injurious to the cardiovascular system, the effects of CSA–CSR are less clear and may be a compensatory response to severe HF.
Aim To determine whether there are compensatory or possibly beneficial aspects caused by CSA–CSR in HF.
Methods Literature review.
Results CSA–CSR can be detrimental in terms of intermittent hypoxaemia, arousals and autonomic dysregulation. However, it is also associated with the beneficial effects of hyperventilation-related increases in end-expiratory lung volume, intrinsic positive airway pressure, assistance to stroke volume, attenuation of excessive sympathetic nervous activity, avoidance of hypercapnic acidosis and finally the provision of periodic rest to fatigue-prone respiratory pump muscles.
Conclusions CSA–CSR has physiological features more likely to be compensatory and beneficial than injurious in HF. Some aspects of CSA–CSR are similar to those seen with positive airway pressure.
- Non-invasive ventilation
- pulmonary oedema
- sleep apnoea
Statistics from Altmetric.com
Heart failure (HF) is a condition of increasing prevalence and incidence associated with a mortality equivalent to many malignancies.1 Thoracic physicians care for acute unstable, and chronic stable HF, by virtue of their skills of non-invasive positive airway pressure ventilatory support (a treatment known to reduce intubation rates and mortality),2 the frequent need to provide oxygen therapy and the reporting of characteristically abnormal pulmonary function such patients have at rest and exercise.3
Moreover, over 50% of HF patients exhibit either obstructive sleep apnoea (OSA) or central sleep apnoea with a Cheyne–Stokes pattern of respiration (CSA–CSR),4 explaining much of the morbidity and possibly the mortality of HF.5 The two apnoea types occur sometimes within the same patient at different times of the same night;6 however, they have different pathophysiological consequences that underpin different therapeutic strategies. Whereas OSA is considered injurious,5 this commentary will argue that CSA–CSR is a compensatory response to severe HF, and in itself may not be injurious to the cardiovascular system.
CSA–CSR is characterised by a crescendo decrescendo pattern of 20–30 s hyperventilation followed by 10–40 s hypopnoeas or apnoeas during exercise, wakefulness or stages 1 and 2 non-rapid eye movement sleep.7 The ratio of ventilation to the overall cycle length has been considered a marker of loop gain.8 CSA–CSR is associated with elevated pulmonary capillary wedge pressure, ventricular dilatation, atrial fibrillation, elevated sympathetic activity plasma brain natriuretic peptide levels,9 10 increased central and peripheral chemosensitivity7 and a restrictive ventilatory defect with impaired transfer factor of the lung for carbon monoxide.3 11 Clinically, CSA–CSR is more common in men and worse in the supine body position.12 CSA–CSR is exquisitely sensitive to arterial carbon dioxide levels, which, if elevated by 1–2 mm Hg (either by inhaled carbon dioxide or added deadspace), can switch off CSA–CSR; however, with persistent tachypnoea and no improvement in sleep quality.13
Treatment of CSA–CSR with HF can be directed at the cause (HF) or the end result (CSA–CSR). The rationale for therapy towards the underlying cause, namely HF, is based on the observation that pharmacological treatment, cardiac resynchronisation therapy and surgical treatment (eg, cardiac transplant) significantly diminish the severity of, and at times sometimes abolish, CSA–CSR.7
Therapies directed specifically towards CSA–CSR include oxygen, respiratory stimulants (eg, carbon dioxide, theophylline, acetazolamide) and continuous positive airway pressure (CPAP). CPAP has the effects of stabilising the upper airway in addition to pulmonary (increasing lung volume, preventing alveolar collapse, assisting inspiratory muscles) and cardiac (reducing afterload and preload) effects, which are operational to differing degrees depending on the apnoea type and HF severity.7 Variants of CPAP, such as adaptive servo-controlled ventilation may offer benefits above CPAP and are currently under investigation.
Is CSA–CSR detrimental?
The rationale for treatment to be directed specifically towards CSA–CSR is based on the premise that CSA–CSR may be detrimental in itself. Evidence in support of this is based on arousals, hyperventilation and hypoxaemia during sleep with CSA–CSR and the associated neurohumoral and autonomic dysfunction, which may contribute to increased mortality. However, these proposed detrimental effects of CSA–CSR are speculative associations, and do not necessarily indicate causation.
CSA–CSR-related hyperventilation and the related respiratory pump muscle activity may result in a relative ‘steal’ phenomenon of an already reduced cardiac output,14 although unobstructed hyperventilation is far less likely to cause fatigue and demand on a diminished cardiac output than would obstructed ventilation (eg, snoring). The hyperventilation-related intrathoracic pressure (ITP) swings (and accordingly left ventricular afterload) seen in CSA–CSR are significantly less (eg, <25 mm Hg) than those seen in OSA (30–120 mm Hg).15 16 Arousals with CSA–CSR are associated with elevations in systemic blood pressure and fragmented sleep similar to OSA. However, arousals do not appear to cause objective or subjective sleepiness in HF populations.17 Excessive sympathetic activity is thought to be injurious in HF. CSA–CSR has been observed to be associated with greater sympathetic activity compared with control groups without sleep apnoea.18 However, when controlled for the severity of HF (ie, with pulmonary artery pressure) the additional effect of apnoea type (either CSA–CSR or OSA) on sympathetic activity is negligible.19 20 By inference, the heightened sympathetic activity due to HF results in hyperventilation and thus CSA–CSR.
A few studies have observed an increased mortality in patients with CSA–CSR compared with HF patients without sleep-disordered breathing, but not all and with insufficient controls for known HF mortality risk factors.7 21 When CSA occurs in non-HF conditions (eg, sudden infant death syndrome siblings, high altitude periodic breathing, idiopathic CSA, narcotic ingestion, oxygen therapy and stroke) it has not been shown to cause mortality. In the largest community-based study, CSA–CSR was not found to be associated with increased mortality.22
Is CSA–CSR a compensatory mechanism for severe HF?
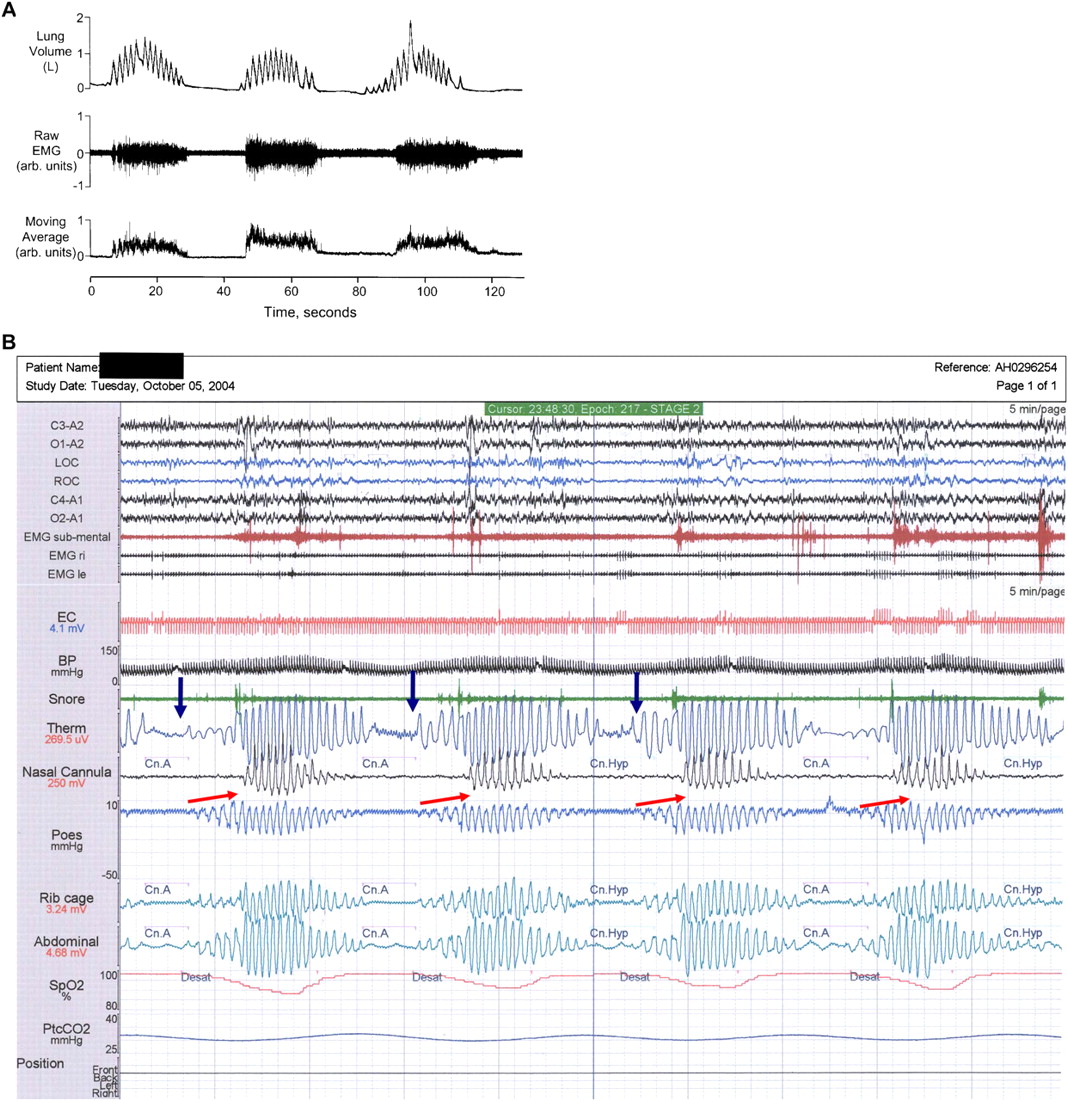
Several lines of argument support this hypothesis. First, end-expiratory lung volume increases by 0.1–1.5 l (mean 400 ml) with the cyclic hyperventilation of CSA–CSR (see figure 1A).23 Increased lung volume would increase oxygen stores, offset the restrictive ventilatory defect and impaired transfer factor of the lung for carbon monoxide commonly observed in advanced HF,3 thus increasing peripheral oxygen saturation, reducing loop gain and resulting in reduced severity of CSA–CSR.24 The increase in end-expiratory lung volume that occurs periodically with CSA–CSR is similar to the effects observed constantly with CPAP of approximately 500 ml.25

{kind=link}
Two polysomnograms indicating (A) elevation in end-expiratory lung volume during hyperpnoeic phase23 and (B) intrinsic positive end-expiratory pressure (arrows) towards the end of the central apnoea with upper airway closure arrows.
Second, deep breaths of periodic breathing and lung inflation promote vagal and reduce sympathetic activity in normal individuals.26 In HF, although it has been shown that CSA–CSR is associated with greater urinary and plasma norepinephrine levels, tritiated norepinephrine spillover and muscle sympathetic nerve activity (MSNA), when controlled for HF severity this difference is no longer significant.19 Large tidal breaths (similar to CSA–CSR) were shown to attenuate MSNA in a group of HF patients during wakefulness.20 During sleep, periods of CSA–CSR were associated with a small rise in overall MSNA; however, attenuation of the MSNA occurred during the hyperventilation phase27 consistent with the hypothesis that large swings in tidal volume attenuate sympathetic activity.
Third, hyperventilation results in respiratory alkalosis, commonly observed in CSA–CSR. The mechanical in-vitro properties of heart muscle are beneficially maintained during hypoxia when in an alkaline pH although depressed when in neutral or acidaemic pH conditions.28 Hypercapnia aggravates canine ischaemic HF, whereas hypocapnia has no deleterious effect.29 Hypocapnia may assist myocardial oxygen extraction (Haldane effect) and reduce myocardial lactate production. Hypocapnia reduces experimentally induced cardiotoxicity30 and causes no adverse effect on cardiac output in humans with coronary artery disease.31 As approximately 25–50% of acute cardiogenic pulmonary oedema patients arrive in emergency departments in hypercapnic acidosis,2 a tendency to keep the pH alkalotic long term when stable would be protective and advantageous.
Fourth, the normal respiratory pump is capable of achieving ITP swings of −120 to +120 mm Hg, and thereby act as an additional cardiac pump during hyperventilation. Episodic rises in ITP, induced by coughing every 1–3 s, can maintain cardiac output in an otherwise asystolic heart for periods of over 40 s.32 However, in HF, the inspiratory ITP are thought to be significantly attenuated15 compared with non-HF patients with OSA.16 Despite this, however, stroke volume has been reported to increase by 25% during the hyperventilation period compared with the apnoeic period in HF33 perhaps by the mechanism above.
Fifth, the ‘apnoea’ in CSA–CSR, is more accurately described as a prolonged slow expiration during which the upper airway usually closes mid ‘apnoea’ resulting in 5–10 mm Hg ‘intrinsic’ positive end-expiratory pressure (PEEP) (see figure 1B) similar to that reported during wakefulness in HF over 75 years ago.34 Small elevations of ITP would have an effect to prevent HF-related alveolar collapse, similar to the effects of intrinsic PEEP in chronic obstructive pulmonary disease and HF.35
Sixth, deep inspiration overcomes bronchoconstriction induced by methacholine. Intrinsic PEEP (as with CPAP) may act as a bronchodilator.36 37 The deep breaths associated with CSA–CSR may thus also serve to overcome airflow obstruction related to bronchial wall oedema seen in HF.
Seventh, anaemia is common and an adverse risk factor in HF.38 The aetiology of anaemia is multifactorial related to haemodilution, malnutrition, renal impairment, medication side effects or simply an anaemia of chronic disease. One study10 of patients with HF and anaemia reported a rise in haemoglobin and a fall in CSA–CSR with 3 months of treatment with erythropoietin and iron. High altitude periodic breathing is associated with an increase in red cell mass in normal individuals.39 Whether hypoxia related to CSA–CSR would offset anaemia in HF is speculative; however, it does warrant further study.
Finally, mathematical modelling indicates that intermittent work followed by rest or recovery is more advantageous than continuous work.40 Maximal inspiratory and expiratory pressures are reduced by approximately 25–50% in middle-aged HF patients with impaired systolic function,41 and a model that provided cyclic work (hyperventilation) and rest (central apnoea) would offset the risk of developing respiratory muscle fatigue.
Asthma and fever offer complementary analogies of CSA–CSR. Asthma-related small airway remodelling has up until recently been thought to be a hallmark of severe uncontrolled asthma, and to be deleterious in itself. However, a recent view has suggested that airway remodelling may protect against smooth muscle shortening and otherwise fatal bronchoconstriction.42 43 Similarly, fever is thought to be compensatory and possibly therapeutic in septic patients. Animal models44 of bacterial sepsis indicate fever to be an adaptive host immunological defence associated with improved survival. And in humans, the cure of syphilis by inducing fever with malaria won Dr Wagner von Jauregg the 1927 Nobel Prize for medicine!45
What are the clinical consequences of viewing CSA–CSR as a compensatory mechanism for advanced HF?
The first is to appreciate that the beneficial consequences of CSA–CSR mirror the effects of upper airway, pulmonary and cardiac effects of CPAP, although periodically rather than continuously. The second is to use the periodicity of cardiac autonomic control (eg, heart rate), controlled by the powerful periodic respiratory drive, as a useful surrogate marker of underlying CSA–CSR when ventilation is ‘stabilised’ by treatments directed specifically at CSA–CSR, such as adaptive servo-controlled ventilation. Finally, ‘treatments’ that replace periodic central apnoeas (and rest) with continuous stimulation of ventilation (and work), such as theophylline, inhaled carbon dioxide or dead space, may lead to detrimental respiratory muscle fatigue.
In summary, the physiological benefits of CSA–CSR in HF include increased lung volume with intrinsic PEEP, augmented stroke volume, avoidance of hypercapnic acidosis, attenuated sympathetic activity, bronchodilation and cyclic respiratory muscle rest. These effects are akin to those seen with episodic CPAP. Treatment of CSA–CSR in isolation of the underlying cause is an uncharted territory and the benefits need to be proved with an individual HF patient's best interest foremost in mind. Treatments that result in the abolition of CSA–CSR by providing a continuous respiratory drive, with agents such as inhaled carbon dioxide, dead space or respiratory stimulants (eg, acetazolamide) need to be counterbalanced by continuous respiratory effort, which may result in a loss of respiratory muscle rest and thus worsening of respiratory muscle fatigue.41 46 In relation to positive airway devices that abolish CSA–CSR, based on respiratory plethysmography, attention should be paid to the presence or absence of the underlying periodic breathing rhythm. Future studies on the pathogenesis of CSA–CSR in HF and analogous conditions will assist in our understanding of this condition.
Acknowledgments
The author would like to thank Ms Teanau Roebuck and Drs Irene Szollosi, Kirk Kee, Scott Sands and Philip Berger for technical aspects related to polysomnography and intellectual discussion, plus Professors Jean Bousquet and Denis Spellman for the insights into analogous physiological processes of fixed airflow obstruction in asthma and the benefits of fever, respectively.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.